
Abstract
Objective
The distal transradial approach (dTRA) may reduce puncture-site complication rates compared with the conventional transradial approach (cTRA). However, the treatment outcomes of dTRA performed with large-bore catheters and the factors associated with procedural success remain unclear. We report the treatment outcomes of neurointerventional therapy performed via dTRA with a sheathless 8-Fr balloon guide catheter (BGC) and identify factors associated with procedural failure.
Methods
We retrospectively reviewed 51 consecutive patients who underwent neurointerventional therapy via dTRA with a sheathless 8-Fr BGC at our institution between April 2023 and March 2025. The primary endpoint was the procedural success rate. The secondary endpoint was the rate of puncture-site-related complications. We also analyzed factors associated with crossover from dTRA to cTRA or to a transfemoral approach (TFA).
Results
Procedural success was achieved in 42 of the 51 patients (82.4%). Crossover to cTRA was required in 5 cases (9.8%), and to TFA in 4 cases (7.8%). Patients requiring crossover to cTRA were significantly older than those who completed the procedure via dTRA (p = 0.02). Acute ischemic stroke (p < 0.01) and use of local anesthesia with light sedation (p < 0.01) were independently associated with crossover to TFA. No major complications occurred. Minor puncture-site hematoma was developed in two patients (3.9%), severe radial-artery spasm in three (5.9%), and asymptomatic distal radial artery occlusion in three (5.9%).
Conclusion
The dTRA for neurointerventional procedures with a sheathless 8-Fr BGC demonstrates an acceptable success rate and safety profile. However, challenges remain with these procedures in older patients and cases with mechanical thrombectomy or local anesthesia with light sedation.
Keywords
Introduction
The transfemoral approach (TFA) remains the gold-standard access route for most neurointerventional procedures. However, randomized cardiology trials have demonstrated that the transradial approach (TRA) lowers the risk of puncture-site complications, morbidity and mortality compared with the TFA,1,2 prompting guidelines to recommend TRA as the first-line access in interventional cardiology.3,4 TRA is now increasingly adopted in neurointerventional procedures as well.5-8
Although major TRA-related complications are infrequent, bleeding events and radial artery occlusion (RAO) still occur. The distal TRA (dTRA), which involves puncturing the radial artery in the anatomical snuffbox, has been proposed to further reduce bleeding complications and RAO.9,10 However, experience and evidence regarding the use of large-bore balloon guide catheters (BGCs) via dTRA in neurointerventions remain limited.11,12 We therefore evaluated the treatment outcomes of neurointerventions performed via dTRA with a sheathless 8-Fr BGC and analyzed factors associated with procedural failure.
Materials and methods
Study design and patients
This single-center, retrospective cohort study was approved by the institutional ethics committee of Ohkawara Neurosurgical Hospital (approval no. O2023-004). We reviewed consecutive patients who underwent neurointerventional procedures—including mechanical thrombectomy (MT), carotid artery stenting (CAS), and coil embolization for intracranial aneurysms—via dTRA using the sheathless 8-Fr BGC between April 2023 and March 2025. For elective cases, access feasibility was assessed preoperatively by computed tomography angiography (CTA). Patients were not assigned to dTRA if CTA revealed extreme vascular tortuosity, a radial artery diameter less than 2 mm, or RAO. For emergency procedures (e.g. acute ischemic stroke), dTRA was attempted if a distal radial pulse was palpable. Final approach selection was left to the discretion of the individual operator.
Procedural technique
MT was performed under local anesthesia with light sedation, defined as a modified Richmond Agitation-Sedation Scale score between −1 and −3; all other procedures were performed under general anesthesia. Ultrasound guidance was not used in this study. After skin preparation, a 22-G needle was inserted at the point of the strongest distal radial pulse in the anatomical snuffbox. Following radial arteriography, a 0.025-inch guidewire was advanced and a 4-Fr, 11-cm introducer sheath was inserted. Severe vasospasm was treated with 100 to 200 µg of intra-arterial nitroglycerin. A 0.035-inch, 180-cm half-stiff guidewire was then advanced into the brachial artery, and the 4-Fr sheath was exchanged over this wire for a sheathless 8-Fr BGC equipped with a dilator. A TMP dilator I (Tokai Medical Products, Aichi, Japan), which has an outer diameter of 6.5-Fr and a total length of 107.8-cm, was used. This dilator was specifically designed for compatibility with an 8-Fr BGC to emphasize procedural rationale. A 5-Fr Simmons catheter and the same guidewire were used to catheterize the target common carotid artery, after which the BGC was navigated to the intended cervical segment. (See Figure 1 for a representative procedural roadmap.)
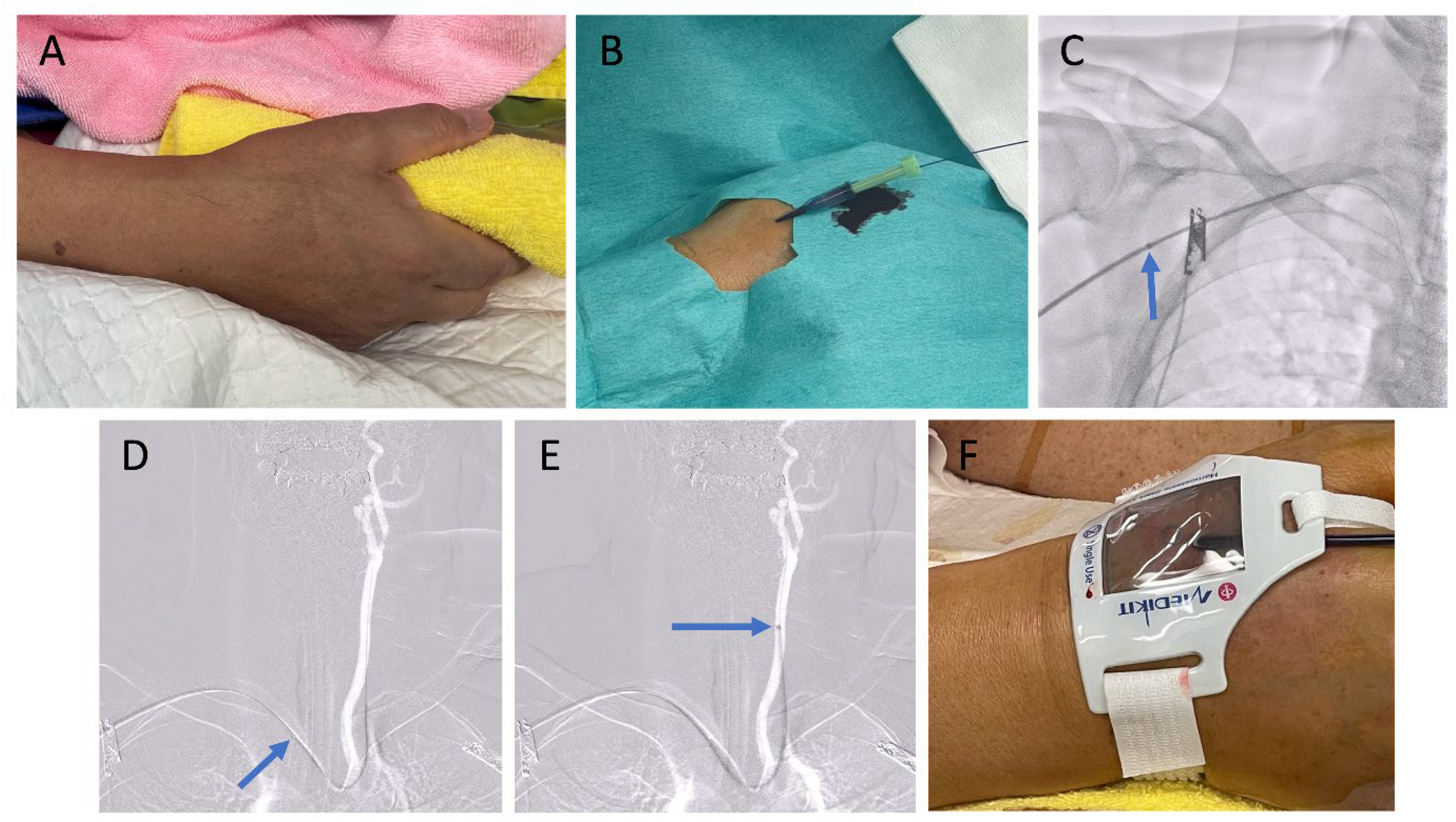
A case of CAS with dTRA using a sheathless 8-Fr BGC to treat a 73% stenosis with unstable plaque at the origin of the left ICA. (A) Hand positioning: holding a towel helps bring the distal radial artery closer to the surface. (B) Puncture of the distal radial artery using a 22-G needle, followed by insertion of a 0.025-inch guidewire. (C) A 4-Fr short sheath is inserted, then exchanged for a sheathless 8-Fr BGC (arrow) using a dilator. (D) A 5-Fr Simmons-shaped catheter is advanced into the left CCA, and a 0.035-inch, 180-cm half-stiff guidewire is placed in the left external carotid artery. (E) The 8-Fr BGC is advanced to the left CCA. (F) Hemostasis is achieved using a hemostasis device after the procedure. Abbreviations: CAS, carotid artery stenting; dTRA, distal transradial approach; BGC, balloon guide catheter; ICA, internal carotid artery; CCA, common carotid artery.
Hemostasis was achieved with a BleedSafe™ compression device (Medikit Co., Tokyo, Japan). The balloon was fully inflated during catheter removal, then gradually deflated until slight oozing occurred, after which 2 mL of air was reinjected.
If arterial puncture failed, the operator converted to conventional TRA (cTRA); if cannulation of the target vessel was unsuccessful, the procedure was converted to TFA.
Endpoints and definitions
The primary endpoint was procedural success, defined as completion of the planned intervention without crossover to any other access site. The secondary endpoint was the incidence of puncture-site-related complications. Major complications comprised infection, hand dysfunction, nerve palsy, arteriovenous fistula, large hematoma, or pseudoaneurysm requiring transfusion or surgical repair. Minor complications included radial artery spasm, RAO without distal ischemia, and small hematoma not requiring transfusion or surgery. Subgroup analyses examined factors associated with crossover from dTRA to either cTRA or TFA.
Statistical analyses
Categorical variables are presented as counts (percentages) and compared using Fisher's exact test. Continuous variables are expressed as the median and interquartile range and were compared using the Mann–Whitney U test. Values of p < 0.05 were considered statistically significant. All analyses were performed with EZR software (version 1.62; Saitama Medical Center, Jichi Medical University, Saitama, Japan).
Results
Baseline characteristics
The study enrolled 51 patients (Table 1). Median age was 75 years and 60.8% of patients were men. Cardiovascular risk factors were common in patients, with hypertension in 86.3%, dyslipidemia in 70.6%, diabetes mellitus in 23.5%, smoking in 19.6%, and chronic kidney disease in 17.6%. The procedures performed were CAS in 35 cases (68.6%), coil embolization of intracranial aneurysms in 9 cases (17.6%), and MT in 7 cases (13.7%). All interventions were attempted via right-sided dTRA. The most frequent target territory was the right anterior circulation (52.9%). Eight procedures (15.7%) were performed as emergencies. Local anesthesia with light sedation was used in 6 patients (11.8%), whereas the remaining 45 patients (88.2%) were treated under general anesthesia. Pre-procedural CTA of the radial artery was obtained in 23 cases (45.1%). Two types of 8-Fr sheathless BGC were employed: Optimo (Tokai Medical Products, Aichi, Japan) in 25 cases (49.0%) and Branchor (Asahi Intecc, Aichi, Japan) in 26 cases (51.0%).
Baseline characteristics of the study population.
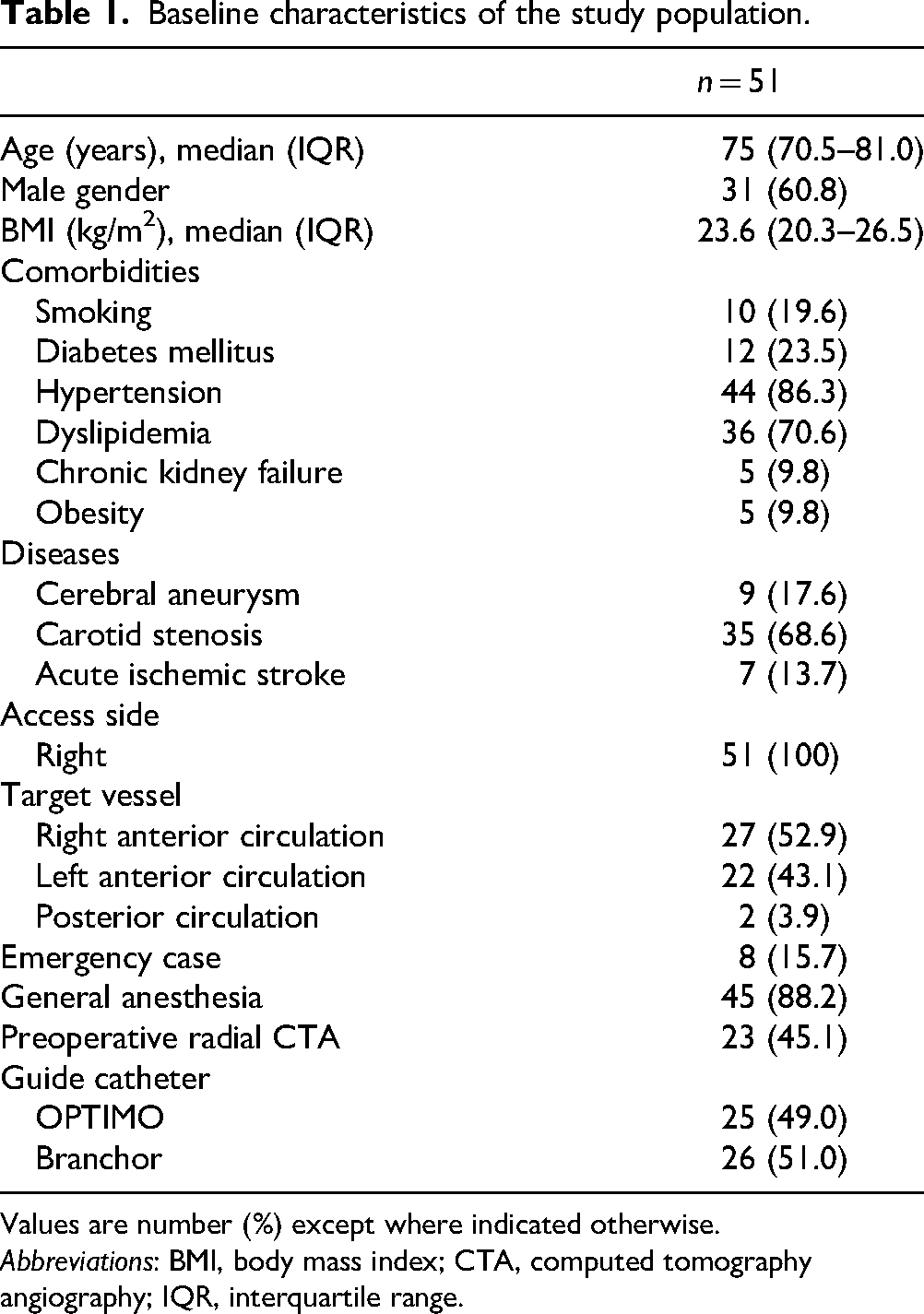
Values are number (%) except where indicated otherwise.
Abbreviations: BMI, body mass index; CTA, computed tomography angiography; IQR, interquartile range.
Crossover and procedural success
The intended procedure was completed via dTRA in 42 of the 51 cases, yielding a procedural success rate of 82.4%. Crossover to cTRA occurred in 5 cases (9.8%), all attributable to cannulation failure. Crossover to TFA was required in 4 cases (7.8%) due to severe vascular tortuosity (subclavian artery in 1 case; radial artery in 3 cases).
On subgroup analyses (Table 2), patients who required conversion from dTRA to cTRA were significantly older than those who did not (p < 0.05). Factors independently associated with conversion from dTRA to TFA (Table 3) were presentation with acute ischemic stroke (p < 0.01) and use of local anesthesia with light sedation (p < 0.01).
Comparison of demographic characteristics between the dTRA group and the crossover-to-cTRA group.
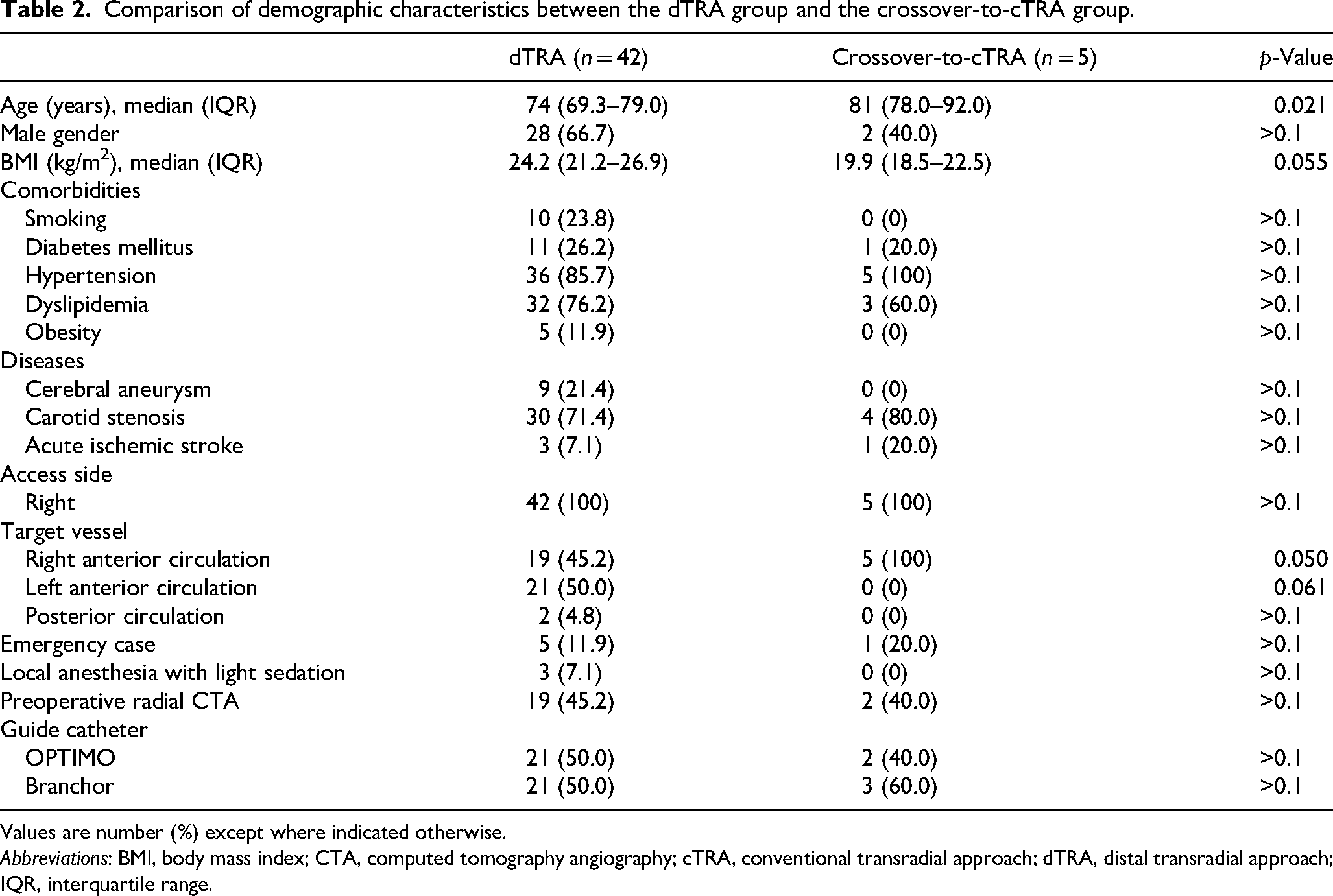
Values are number (%) except where indicated otherwise.
Abbreviations: BMI, body mass index; CTA, computed tomography angiography; cTRA, conventional transradial approach; dTRA, distal transradial approach; IQR, interquartile range.
Comparison of demographic characteristics between the dTRA group and the crossover-to-TFA group.
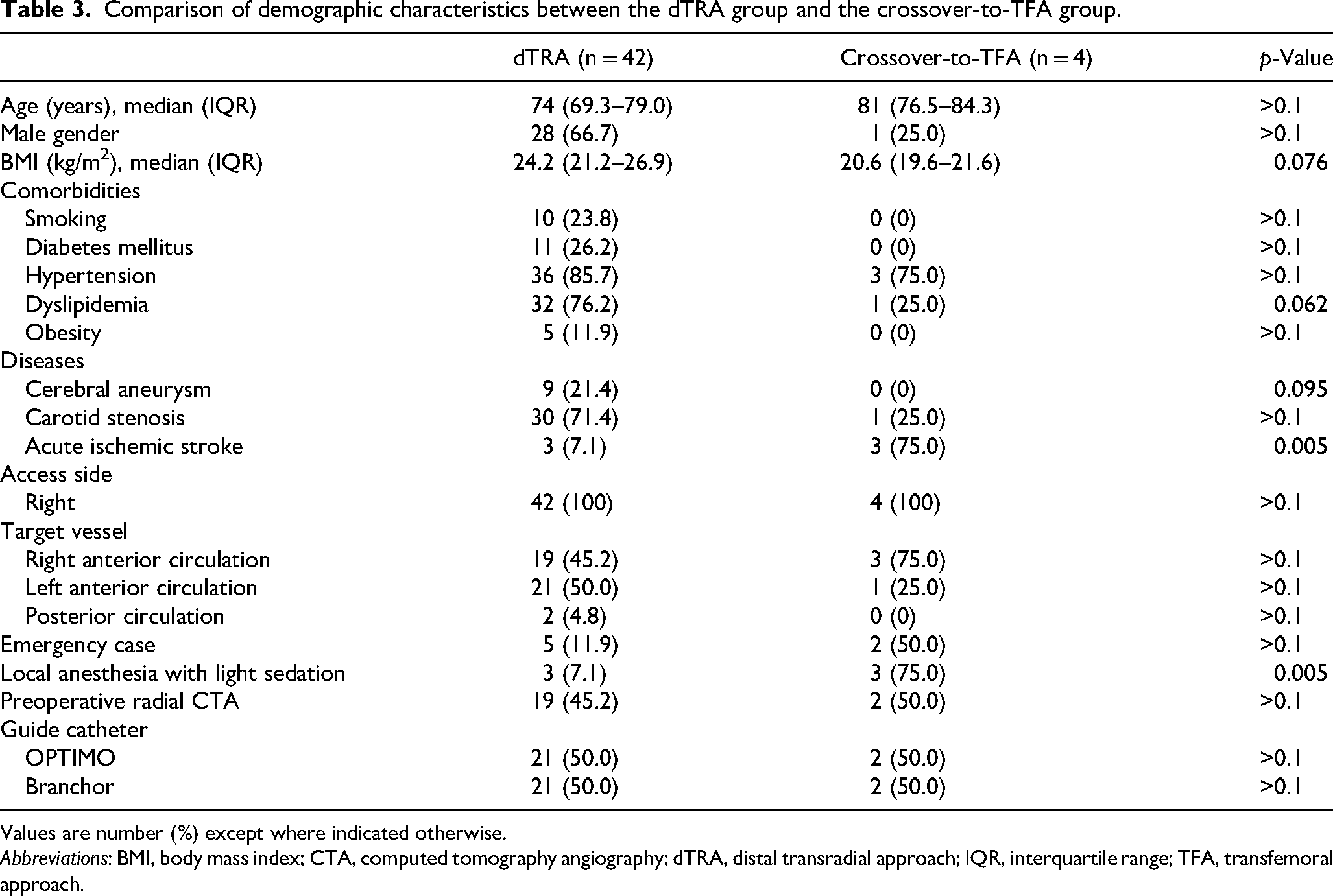
Values are number (%) except where indicated otherwise.
Abbreviations: BMI, body mass index; CTA, computed tomography angiography; dTRA, distal transradial approach; IQR, interquartile range; TFA, transfemoral approach.
Access-site complications
Access-site events are summarized in Table 4. No major complications were observed. Minor events included puncture-site hematoma in 2 cases, and severe radial-artery spasm in three cases. Routine follow-up ultrasonography of the distal radial artery was performed in 34 patients (66.7%), with asymptomatic distal RAO detected in 3 patients (8.8%). Radial artery diameter tended to be smaller in cases with RAO (2.2 mm) than in cases without RAO (2.6 mm, p = 0.115).
Adverse events reported in this study.
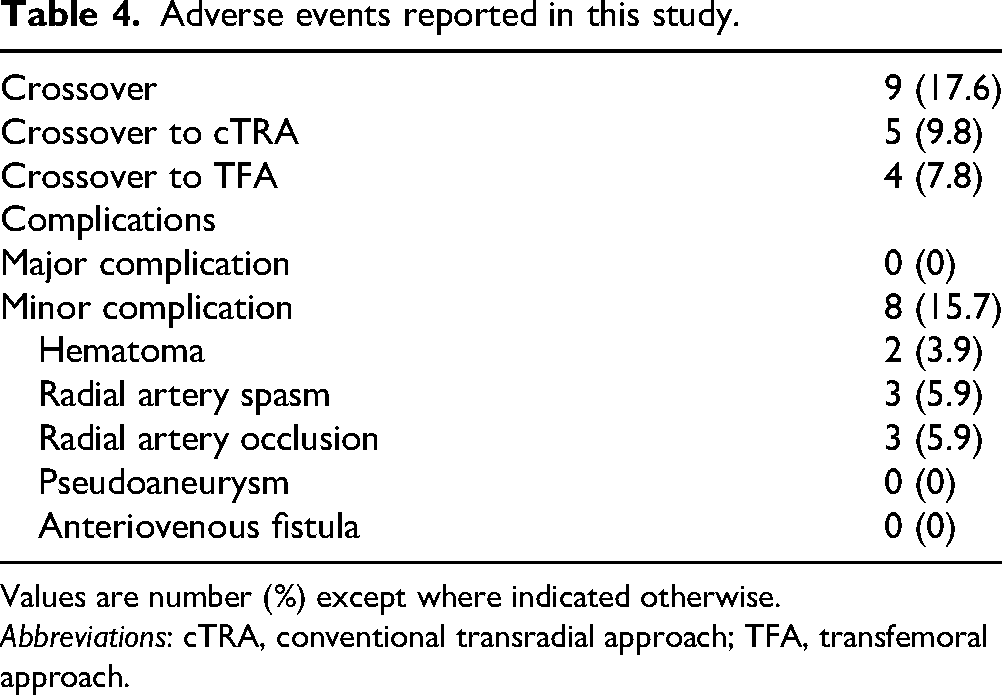
Values are number (%) except where indicated otherwise.
Abbreviations: cTRA, conventional transradial approach; TFA, transfemoral approach.
Discussion
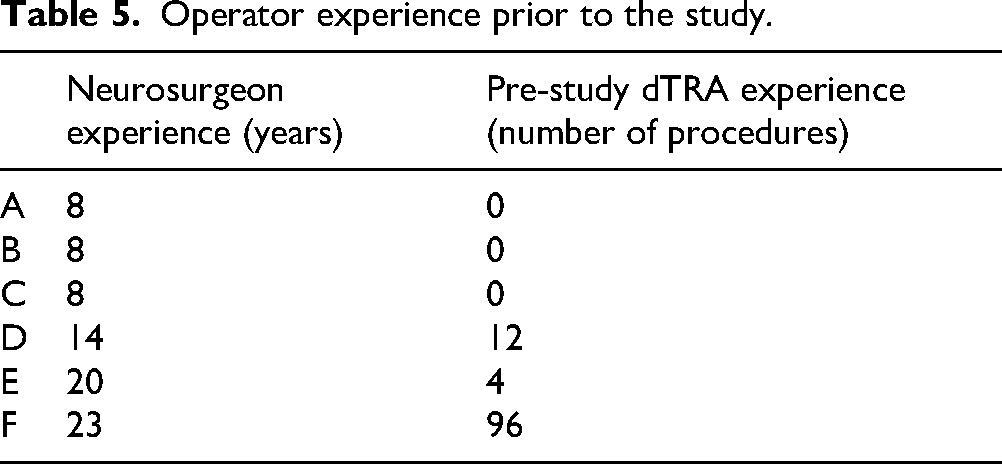
The dTRA is increasingly being adopted because this access lowers the risk of hand ischemia, preserves the proximal radial artery, shortens hemostasis time, and allows a more comfortable arm position for the patient.10,13 In our series, the overall procedural success rate was 82.4% (42/51 cases). Cannulation failed in 5 patients (9.8%), and advanced age was the only significant predictor of failure. The dTRA is technically more demanding than cTRA. 14 Kiemeneij et al. reported an 11% puncture failure rate. 9 Another randomized study showed a high rate of cannulation failure in the dTRA group (30%) compared to the cTRA group (2%; p < 0.001). 13 That study suggested that reasons for this lower success rate were smaller caliber of the distal radial artery in the anatomical snuffbox, greater vessel tortuosity, less stable position of the hand and the operator learning curve. Some studies have examined the relationship between operator experience and procedural outcomes, suggesting that 150 to 200 cases are needed to master dTRA.15,16 Moreover, a large prospective multicenter registry identified having fewer than 100 dTRA cases as a predictor of puncture failure. 17 In our study, 6 neurointerventionalists with heterogeneous experience performed the procedures. The average number of dTRA procedures prior to the study was 18.7 (range, 0–96; Table 5). Nevertheless, both the success and complication rates remained acceptable—even during their early experience. Although we did not use ultrasound guidance either due to operator preference or lack of familiarity, previous cerebral angiography studies indicate that ultrasound improves puncture success and should be considered, especially early in the learning curve. 18
Operator experience prior to the study.
In this study, conversion from dTRA to TFA occurred in 4 patients (7.8%). Acute ischemic stroke and the use of local anesthesia with light sedation were variables that overlapped entirely with our MT cohort and thus represented predictors of crossover, highlighting the technical difficulties of dTRA in urgent MT. Other studies likewise found TFA preferable in cases involving MT, left anterior circulation, elderly patients, or patients with a type III aortic arch. 6 Although pre-procedural CTA was not an independent predictor for procedural success in our analysis, evaluating the access route with CTA can identify tortuous segments, radial artery loops, or severe vasospasm that may necessitate alternative access.
The utility of BGCs across different neurointerventional procedures has been reported. For instance, previous studies have shown that BGCs offer three main advantages in treating anterior-circulation aneurysms: (a) proximal flow control in the event of unexpected intraprocedural rupture; (b) easier deployment of a compliant balloon across the aneurysm neck; and (c) stabilization of the initial coil, preventing additional protrusion or distal migration when coil loops herniate into the parent vessel.19,20 A systematic review showed that a proximal balloon strategy during CAS was associated with lower odds of new ischemic lesions compared to distal filter and distal balloon on diffusion-weighted magnetic resonance imaging. 21 Non-randomized studies have suggested that BGC use during MT for acute ischemic stroke is associated with superior clinical and angiographic outcomes. 22
Navigating an 8-Fr BGC through dTRA can be challenging. We used a stiff-type, 5-Fr modified Simmons-shaped catheter with long curve length as an inner catheter, and a 0.035-inch half-stiff guidewire. Once this combination reached the target vessel, the sheathless 8-Fr BGC could be advanced successfully in most cases. We employed two 8-Fr BGCs: the OPTIMO, with an inner diameter of 0.087 inch; and the Branchor, with an inner diameter of 0.086 inch. The use of an 8-Fr BGC provides several advantages, including stable proximal support and compatibility with a wide range of devices. Either catheter can accommodate a 6-Fr distal-access catheter for adjunctive coil embolization of cerebral aneurysms and is compatible with a 10-mm carotid stent. All 0.071 inch aspiration catheters fit the 8-Fr OPTIMO, whereas all 0.071 inch devices other than the REACT 71 (outer diameter, 0.0855 inch; Medtronic, Minneapolis, MN, USA) fit the 8-Fr Branchor. According to the manufacturer's instructions, the REACT 71 requires a catheter with an inner diameter of ≥0.087-inch. 23 In our experience, advancing the REACT 71 through an 8-Fr Branchor catheter generates marked resistance, indicating incompatibility.
A meta-analysis showed a significantly lower rate of RAO with dTRA (2.3%) compared to cTRA (4.9%, p = 0.004). 24 In our cohort, distal RAO occurred in 3 patients (8.8 % of those screened by ultrasound). This relatively high rate may reflect exclusive use of large-bore BGCs, prolonged compression time, and catheters originally designed for femoral access. Fortunately, all occlusions were asymptomatic; the puncture site for dTRA is distal to the origin of the deep palmar arch, and collateral flow from the superficial palmar arch generally prevents ischemia. In addition, distal RAO has been reported to be reversible in approximately 60% of cases within 1 to 3 months. 25 Our analysis showed a trend toward smaller radial artery diameter in RAO cases. Onodera et al. reported a significantly smaller diameter of the radial artery in the RAO group, with a cutoff value of 2.4 mm for predicting RAO. 12 Preoperative measurement of radial artery diameter may help predict RAO following the dTRA.
Our experience confirms that neurointerventional procedures via dTRA even using an 8-Fr BGC are feasible when pre-procedural imaging excludes severe tortuosity or distal radial artery diameter is <2 mm. Nevertheless, wider adoption is hampered by the limited familiarity of operators with the procedure, the need to traverse the learning curve, and the absence of catheters and devices specifically engineered for radial access. Dedicated radial BGC systems would likely increase success rates and reduce complications.
Limitations to this investigation included the retrospective single-center design, the lack of a control arm, potential selection bias stemming from the operator choice of access, and incomplete ultrasound follow-up, which may have led to underestimation of the true incidence of RAO. Larger prospective studies are required to confirm our findings.
Conclusion
Our initial experience suggests that neurointerventional procedures via dTRA with a sheathless 8-Fr BGC are safe and feasible, although elderly patients, MT cases, and procedures under local anesthesia with light sedation remain challenging. Preoperative radial artery imaging and careful patient selection may enhance success rates.
Footnotes
Acknowledgments
Ethical approval
The study was approved by the institutional ethics committee of Ohkawara Neurosurgical Hospital (approval no. O2023-004).
Informed consent
Written informed consent was not required due to a waiver granted by the committee. Patients in the study were also given the opportunity to refuse to participate in the study by opting out. This study is based on the current version of the Declaration of Helsinki.
Authors’ contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available upon reasonable request from the corresponding author.