
Abstract
Objective
This study aims to determine the outcomes of nickel allergic patients who underwent a trial of forearm arterial stenting with a nickel-based stent, with follow-up to assess for an allergic reaction. In the absence of adverse effects, patients had their intracranial aneurysm treatment with a nickel-based cerebrovascular device.
Methods
A retrospective analysis was performed on patients who had an allergy to nickel, with an intracranial aneurysm who underwent treatment with a permanently implanted nickel-containing device. Nickel allergy was established by clinical history and dedicated patch testing. Outcomes such as in-stent thrombosis or any intracranial complications were recorded.
Results
Over a 10-year period, there were 18 patients who had a peripheral stent without development of in-stent stenosis, thrombosis or occlusion. One patient developed a cutaneous allergic reaction to the peripheral stent and their intracranial procedure was with a nitinol-free device.
Of 17 patients who underwent intracranial treatment with a nitinol device, there was one patient who developed a postoperative complication of fish-mouthing of the device which has been reported in patients with a nickel contact allergy, but further studies are warranted to establish a causative relationship. Another patient omitted prescribed antiplatelet medication and occluded their stent. The remaining fifteen patients developed no complications with aneurysm occlusion on imaging.
Conclusion
Patients with a nickel allergy who would be eligible for endovascular treatment could benefit from trial peripheral arterial stenting. This provides an alternative approach to avoid unnecessarily eliminating endovascular treatment options with nickel-containing devices from which these patients may potentially still benefit.
Introduction
Nickel allergy is a common occurrence in the population, affecting 17% of females compared to 3% of males. 1 This poses challenges in treating intracranial aneurysms since many aneurysm treatment options contain nickel alloys, such as nitinol, which are favoured due to their shape memory properties.
Nickel allergy has been described in relation to cardiac endovascular devices, with nickel-hypersensitive patients having an increased incidence of in-stent stenosis.2–3 Additionally, neurological injury attributed to nickel-based endovascular devices, such as cerebritis or cerebral oedema, has been suggested.4–7
Conversely, two case series of patients with a documented cutaneous nickel hypersensitivity did not report any adverse outcomes when using the Pipeline embolisation device (Medtronic, Dublin, Ireland).8,9 It has been purported that the nickel release from intracranial devices is negligible and that patients with an allergy may be safely treated with select nickel-containing devices. 10 Current recommendations suggest formal allergen testing and/or consideration of limiting the therapeutic options to nickel-free devices. 11
This study aims to determine the outcomes of nickel allergic patients who underwent a trial of arterial stenting in their forearm with a nickel-based cerebrovascular stent, with follow-up to assess for complications or allergic reaction. In the absence of such adverse effects, patients had their intracranial aneurysms treated with a nickel-based cerebrovascular device.
Materials and methods
Study design and patient selection
Based on a literature search and multiple anecdotal cases in the United Kingdom, it was apparent that patients with a proven nickel allergy were being treated with nickel-containing intracranial devices. This raised ethical concerns within our department with reluctance to offer such treatments without any further assessment or precautions. Therefore, we developed a peripheral arterial stent testing protocol which was offered to patients requiring this form of treatment. This has its own ethical considerations and for this purpose an in-depth discussion and detailed explanation was provided to each patient followed by their written informed consent.
A retrospective analysis was performed on all patients who had a confirmed allergy to nickel on skin patch testing, with an intracranial aneurysm who underwent treatment with a permanently implanted nickel-containing device.
Data collection
A database of all eligible patients for the study was tabulated to record demographic, clinical, and radiological data. Outcomes such as in-stent thrombosis or any intracranial complications related to the nickel device were recorded. All patient data were appropriately anonymised to maintain confidentiality. Data collection took place in a single tertiary level U.K. centre, The Walton Centre for Neurology and Neurosurgery, between July 2014 and July 2024 (10 years).
Allergy testing, pre-procedure protocol and peripheral stenting
Nickel allergy was established by clinical history and dedicated patch testing under the care of an immunologist. Patch testing involved application of the nickel metal allergen to the patient's back or abdomen with subsequent skin inspection for an allergic reaction after 48 h. If patch testing demonstrated an allergy to nickel, patient cases were discussed in a multidisciplinary team setting and if the consensus was that endovascular treatment was amenable for aneurysm treatment, the patients were reviewed by an interventional neuroradiologist in an outpatient clinic. In the outpatient setting, the patch testing results were explained to the patient and the rationale to undertake peripheral arterial stenting, with a documented informal consent undertaken by the interventional neuroradiologist in clinic (formal written consent performed on the day of procedure). The complications of peripheral stenting were explained to the patients, which included cutaneous allergic reaction, forearm haematoma, vessel dissection, stent thrombosis, stent migration and possible stentectomy if compromise of vessel patency. Then the patient was listed for an endovascular radial or ulnar artery stent insertion under local anaesthetic to assess for any clinically significant reaction to medical grade nickel contained in a cerebrovascular stent.
Within our tertiary centre, procurement of laser-cut, braided and flow diverting stents is facilitated via the public health system; National Health Service England. These devices are obtained on consignment from the device manufacturer companies. Following usage of the device, the company is reimbursed the money for the utilised product, with no cost borne by the treated patient.
Prior to the procedure, patients were commenced on a seven-day course of dual antiplatelet therapy consisting of aspirin and clopidogrel. Patients were not administered antihistamines or corticosteroids prior to the procedure. An adequate response to this medication was ensured with VerifyNow (Werfen, Bedford, Massachusetts, USA) point of care platelet testing performed on the day of the procedure. Either the radial or the ulnar artery was selected for stenting, following an interrogation of the vasculature with ultrasound. The most superficial segment of the forearm artery being stented was targeted in case the patient required subsequent surgical retrieval of the stent after a refractory allergic reaction. Under ultrasound guidance, a 5Fr sheath was placed in either the radial or ulnar artery. Once the sheath was in situ, a contrast injection through the sheath was performed to measure the vessel calibre. A Headway 17 microcatheter (Terumo Neuro, Aliso Viejo, California, United States) was introduced via the sheath and the stent was deployed at the targeted location with repeat contrast injection performed following stent deployment (Figure 1).
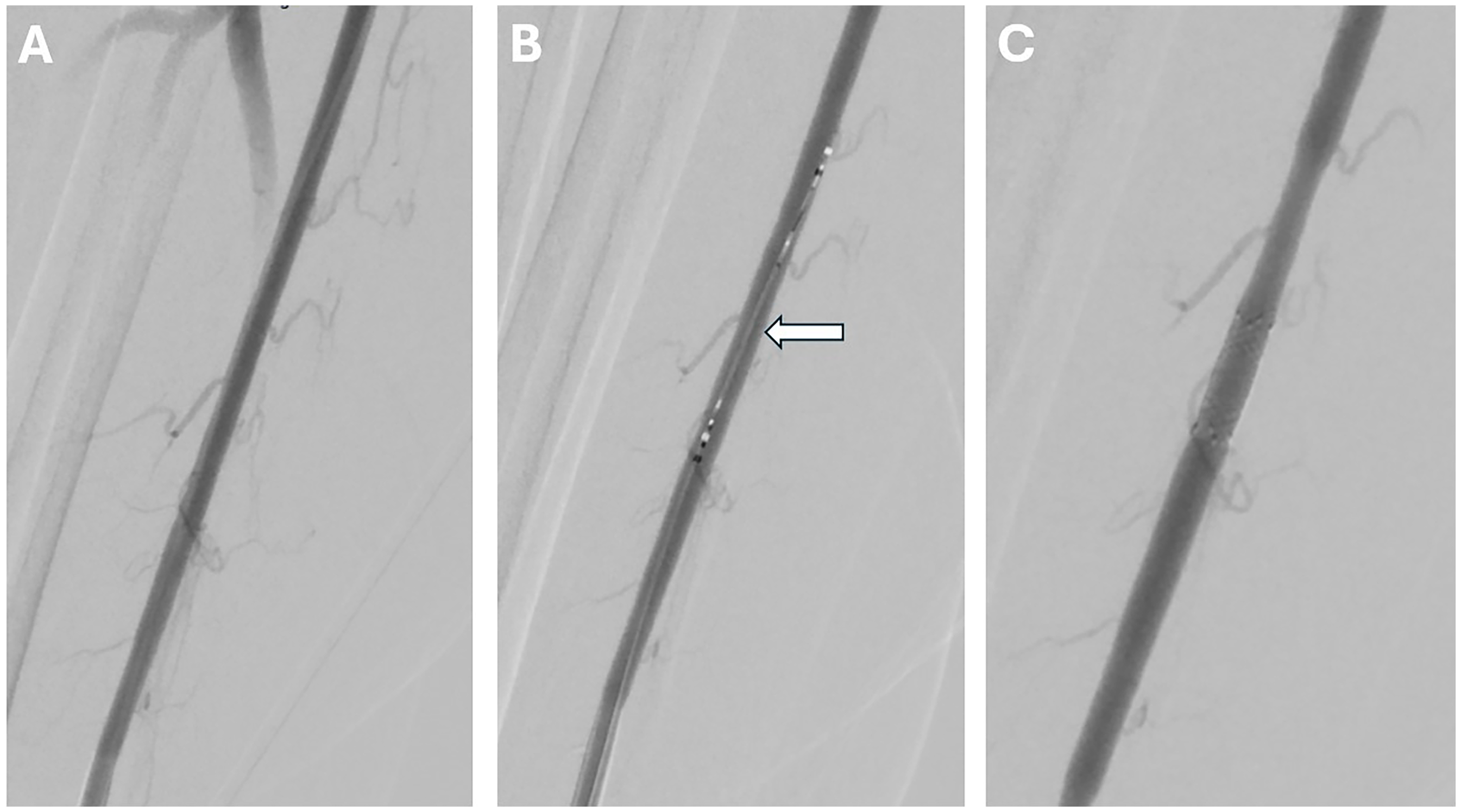
(A) Digital subtraction angiogram of the radial artery through the 5Fr sheath. (B) Headway 17 (MicroVention Terumo, Aliso-Viejo, CA, US) microcatheter within the radial artery with the constrained LVIS EVO (MicroVention Terumo, Aliso-Viejo, CA, US) introduced into the catheter (white arrow). (C) Repeat angiogram of the radial artery with the stent implanted within the vessel.
Post-procedure monitoring
Following the peripheral stent insertion, the patients continued their dual anti-platelet regimen and were closely followed up by the neurovascular service to assess for an allergic reaction. This involved outpatient clinical assessment of the forearm in all patients to assess for any allergic reaction, and an ultrasound typically six weeks after implantation to assess for vessel patency or in-stent thrombosis, although in some patients an ultrasound was not performed. The ultrasound examination included a B-mode and colour Doppler flow assessment of the stent (Figures 2 and 3). If B-mode and colour Doppler flow demonstrated no evidence of stenosis of the stent or increased velocity through the stent construct, it was determined that the stent had remained patent post implantation.
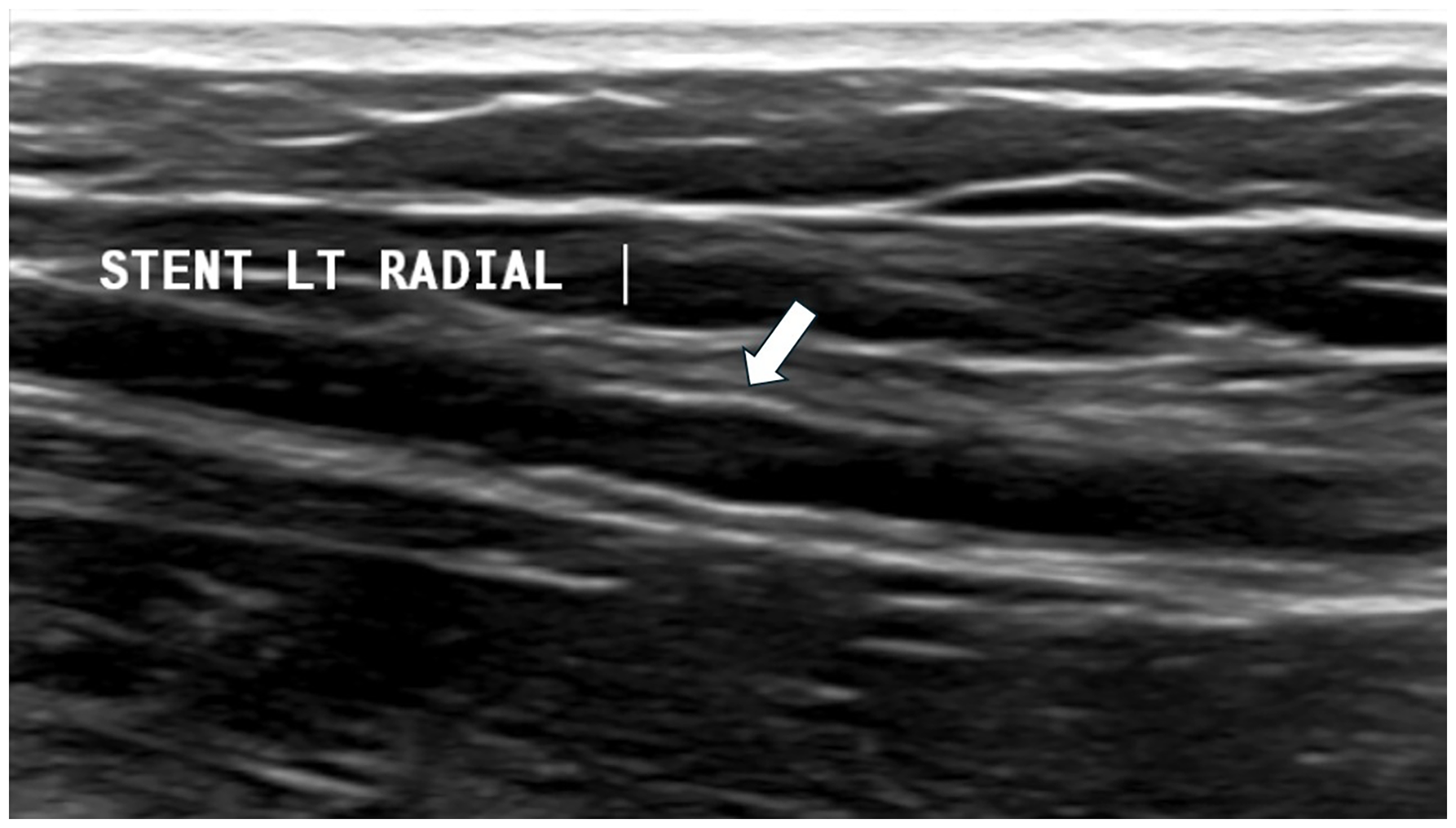
Ultrasound examination of the radial artery demonstrating the implanted stent (white arrow) with no evidence of thrombus formation within the stent construct or stenosis of the stent.
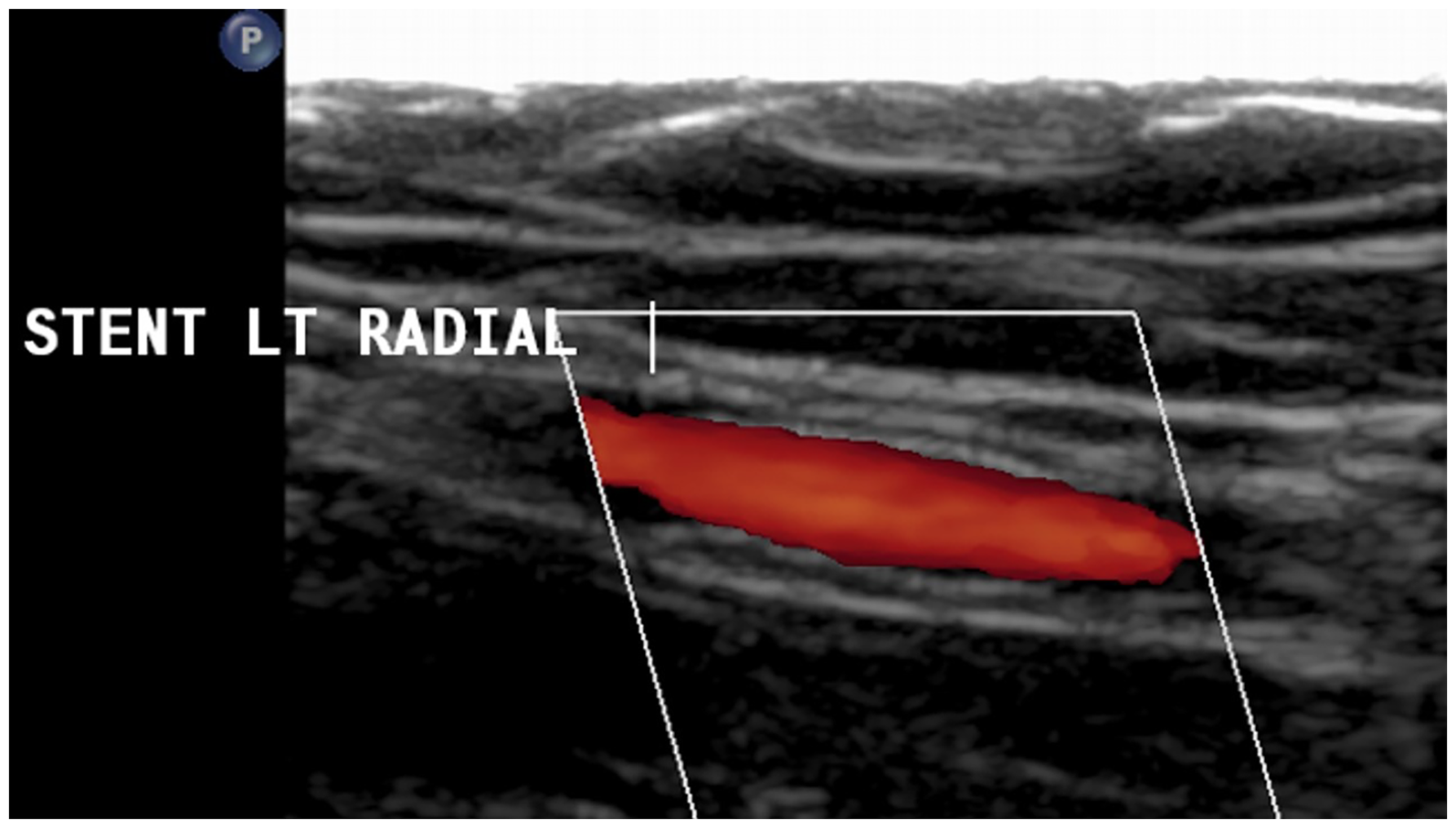
Colour Doppler flow ultrasound examination of the radial artery demonstrates patency of the implanted stent with no obstruction of flow.
Intracranial treatment protocol
If the patient did not report an allergic reaction and the ultrasound study was normal, then the patient was listed for intracranial endovascular treatment for their aneurysm. As patients were already on dual antiplatelet therapy following the peripheral stenting, these medications were continued to the day of the intracranial treatment. The device of choice was either a braided stent, a flow-diverting stent or a Woven Endo-bridge (WEB) (Terumo Neuro, Aliso Viejo, California, United States) device depending on the aneurysm site and morphology. All cerebral procedures were performed under general anaesthesia and patients were not pre-treated with corticosteroids or antihistamines. The patients treated with stents continued dual antiplatelet therapy for at least six months, whereas those treated with a WEB device were either treated with a single antiplatelet for three months or had their antiplatelets stopped altogether at the discretion of the treating interventional neuroradiologist. An example patient case is provided in Figures 4–6.
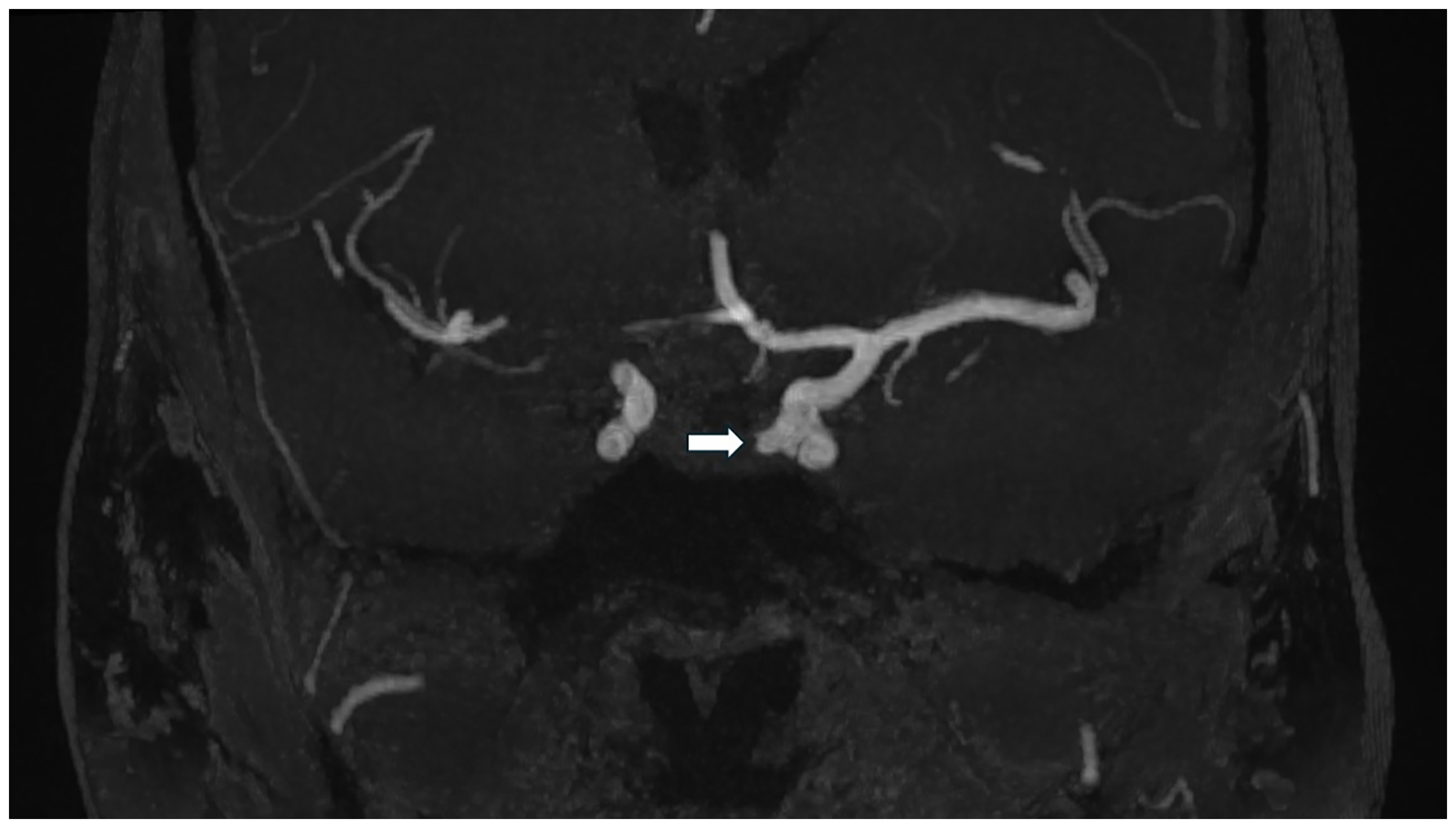
MRI time of flight angiography in a coronal plane demonstrating a lobulated wide necked medially projecting left para-ophthalmic aneurysm (white arrow).
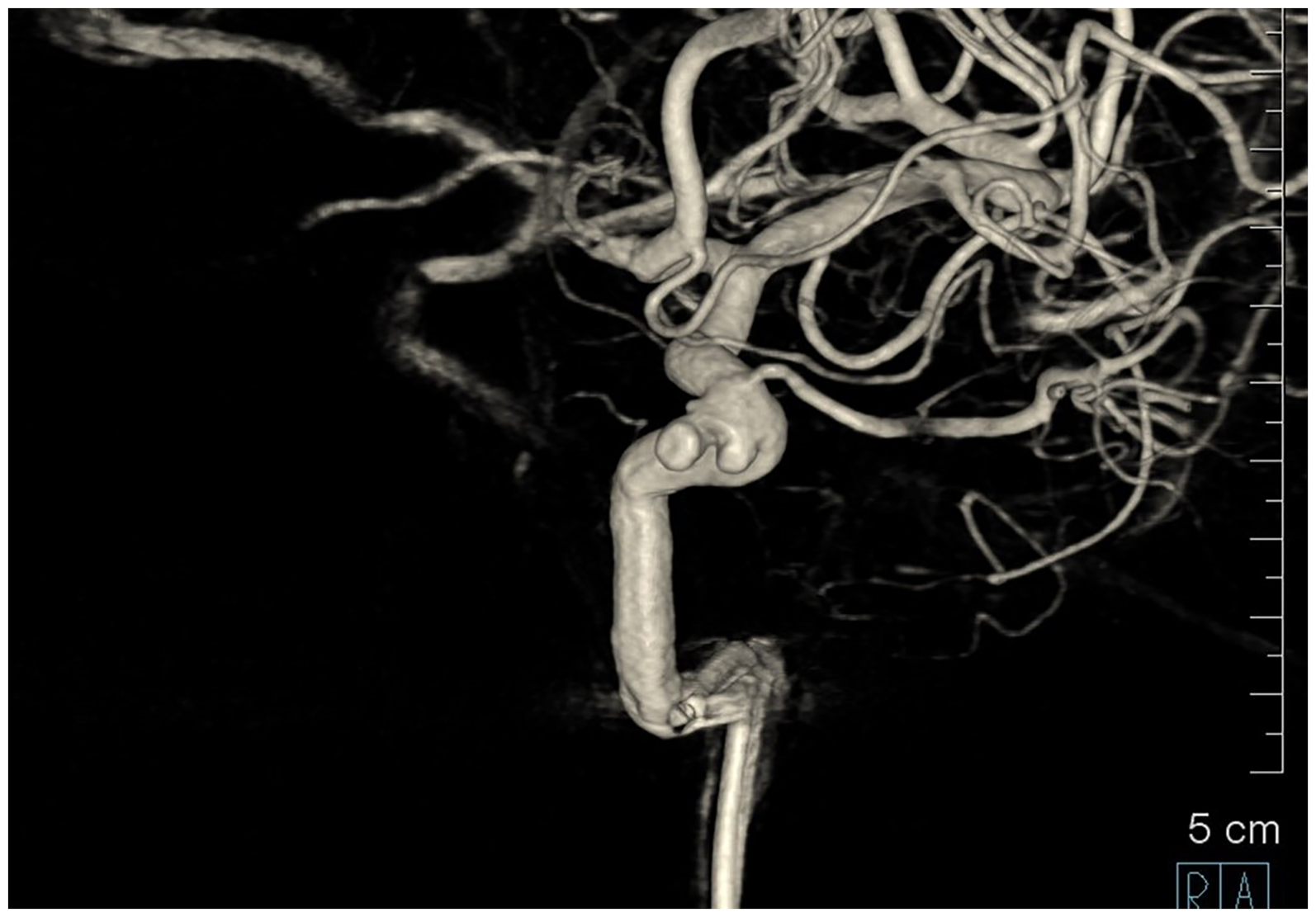
Reconstructed 3D model of left internal carotid artery spin angiography which demonstrates the lobulated wide necked medially projecting left para-ophthalmic aneurysm.
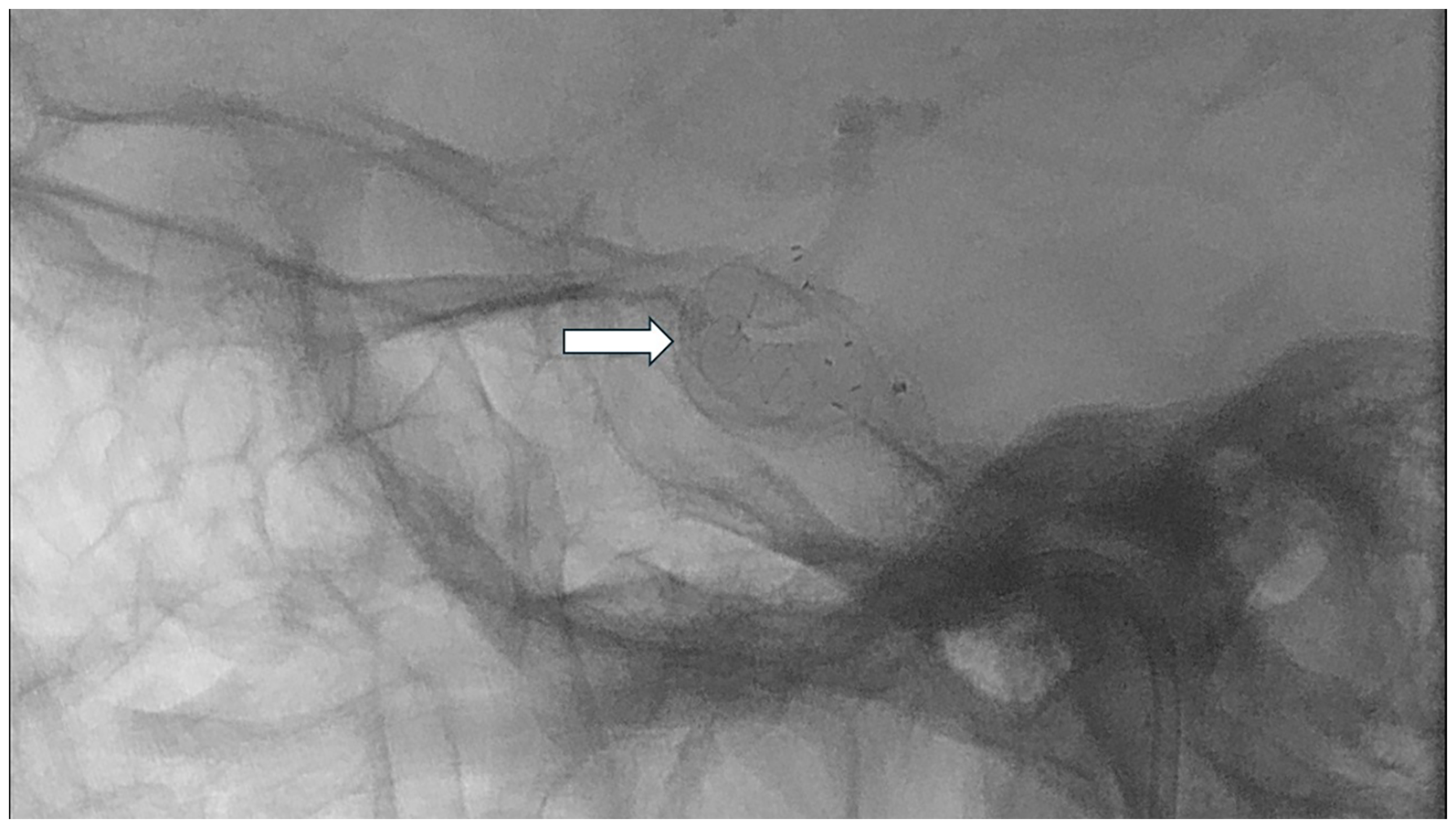
Dynamic rotation spin angiography of the left internal carotid artery following deployment of p64 (Phenox GmbH, Lise-Meitner-Allee 31, 44801 Bochum, Germany) flow diverting stent (white arrow).
Results
Peripheral stent outcomes
Over a 10-year period, there were eighteen patients who met the inclusion criteria for the study. These constitute 2.3% (18/783) of all elective patients treated over this period. Of these 18 patients, there were 12 patients who had a radial stent implanted, and six patients who had an ulnar stent implanted. There were 12 patients who underwent clinical assessment and ultrasound follow-up, with the remaining six patients having the peripheral stent only clinically assessed.
None of the patients developed peripheral limb in-stent stenosis, thrombosis or occlusion. There were two patients who reported development of an erythematous rash of the forearm on the side of stent implantation. In one patient it was felt that the implanted stent was the causative factor since the reaction occurred one day after stent insertion and required antihistamines to resolve. The other patient had a past medical history of eczema and the development of the rash two weeks following stent insertion was attributed to her pre-existing eczema, which self-resolved without corticosteroids/antihistamines.
Intracranial treatment outcomes
Subsequently, 17 patients from the studied cohort have undergone neurovascular intervention for their underlying aneurysms, and one patient scheduled for endovascular treatment of their intracranial aneurysm passed away from a non-neurological pathology prior to undergoing the treatment. Performed endovascular treatment included nine patients treated with a flow diverter, four patients treated with a braided stent, two patients treated with a WEB, one patient treated with a braided stent and WEB device, and one patient with a cutaneous reaction attributed to the peripheral stent who underwent aneurysm coiling alone.
With one exception, none of the patients experienced an intra-procedural related complication. The former developed intra-procedural complete stent occlusion due to the proximal aspect of the stent failing to deploy correctly. This device related complication was successfully managed with a mechanical thrombectomy and intra-arterial thrombolysis.
Follow-up
All treated patients were scheduled to have a baseline magnetic resonance imaging (MRI) study and there afterwards studies at planned intervals. Intracranial follow up imaging was with MRI, intravenous digital subtraction angiography (DSA) and/or standard arterial DSA, ranging between six and 18 months from the date of the intracranial procedure. Intravenous DSA was used as an alternative to arterial DSA in patients who were not coiled (i.e. stent or WEB alone). This was not used in patients who were coiled due to the resultant artefacts which makes adequate image interpretation on intravenous DSA difficult or impossible.
Follow-up imaging for 15 patients demonstrated good flow through the stented vessels and complete aneurysm occlusion/near complete aneurysm occlusion. Two patients had complications after the intracranial procedure identified on follow-up imaging. One patient underwent endovascular treatment of a left anterior cerebral artery aneurysm, with a hypoplastic right A1 segment. The aneurysm was at the junction between the left A1 segment and the bilateral A2 segments. The patient was planned for braided stent assisted coiling of the left A1/A2 aneurysm with a LVIS EVO (Terumo Neuro, Aliso Viejo, California, United States) stent. The braided stent was deployed from the ipsilateral left A2 segment to the dominant A1 segment of the ACA across the aneurysm neck, with a jailed microcatheter for coiling of the aneurysm. Following discharge, the patient presented with bilateral anterior circulation arteries stroke with complete stent occlusion on computed tomography (CT) angiography. Subsequently, it was reported that the patient had been omitting doses of the dual antiplatelet medications prescribed which likely resulted in stent occlusion.
The other patient developed a right sided weakness one day following the intracranial procedure which resolved with Tirofiban infusion and an induced high mean arterial pressure, to a range of 100–110 mmHg for a period of 24 h. CT angiography at the time demonstrated normal flow through the flow diverted vessel. Subsequently, one week following the intracranial flow diversion, the patient developed a right upper limb weakness and mild expressive dysphasia which was again managed with repeated induced high mean arterial pressure. An MRI study at the time demonstrated a focal narrowing in the proximal aspect of the flow diverting stent and a small left pontine area of infarction. The patient had a prolonged inpatient stay with resolution of the expressive dysphasia and residual mild right upper weakness on discharge. Subsequent MRI demonstrates a stable stenosis in the proximal aspect of the flow diverting stent and complete aneurysm occlusion.
A complete breakdown of the patient demographics including the type of peripheral stent, intracranial device, complications and follow-up, is presented in Table 1.
Patient demographics including the type of peripheral stent, intracranial device, complications and follow-up.
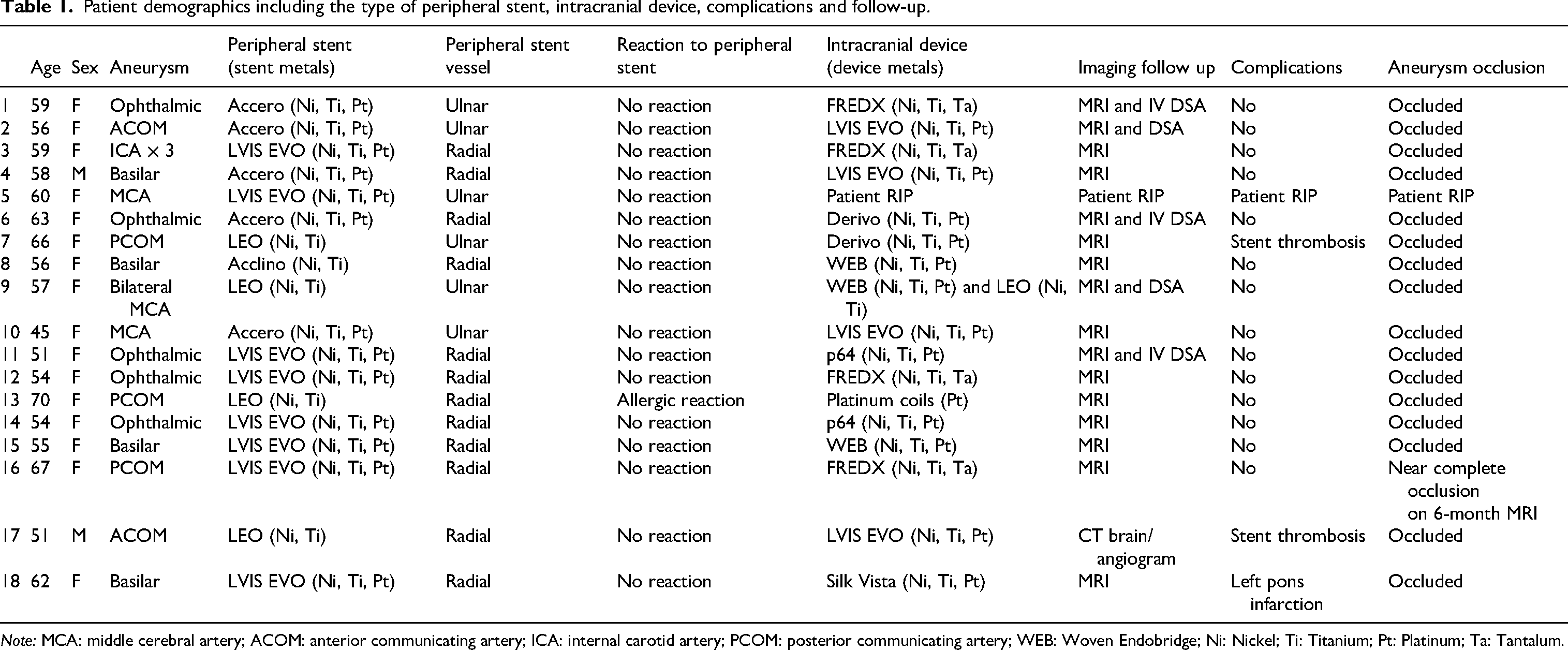
Note: MCA: middle cerebral artery; ACOM: anterior communicating artery; ICA: internal carotid artery; PCOM: posterior communicating artery; WEB: Woven Endobridge; Ni: Nickel; Ti: Titanium; Pt: Platinum; Ta: Tantalum.
Discussion
Nickel allergic patients present a challenge to neurointerventionalists and their desired choice of aneurysm treatment device. This technique of testing a nickel-based stent at non-critical sites in those patients who have been confirmed to have a nickel allergy provides a means of predicting any significant allergic reaction to a stent. This then informs the choice of treatment options for cerebral aneurysms in these patients. Those with an allergic reaction attributed to a forearm arterial stent can then be considered for safer treatment, such as coiling alone or clipping.
Trial peripheral stenting in a forearm artery was proposed given the rich collateralised vascular supply of the hand through the radial and ulnar arteries, with associated supplemental arteries. 12 The cohort of 18 patients in this series who had a peripheral stent inserted showed no evidence of in-stent stenosis, thrombosis or occlusion. Of these, a sub-cohort of 17 patients underwent endovascular cerebral aneurysm treatment with a wide variety of nitinol containing devices ranging from braided stents to flow divertors to WEB device, and no definite complications were attributed to a patient's nickel allergy. A single patient with a reaction attributed to the forearm arterial stent was treated without the use of nickel-containing devices.
Nickel is commonly used in conjunction with other metals as an alloy to produce a wide range of medical devices and implants. 2 Nickel bonding with titanium in an intermetallic phase (50% nickel, 50% titanium) provide a very stable chemical bond. A nickel–titanium alloy has been widely used in the manufacture of minimally invasive implants, including orthopaedic prostheses and dental instruments. The alloy provides excellent biocompatibility, corrosion resistance, super-lubrication, and shape memory effects, which are all tenants warranted in the development of intracranial endovascular devices. As a result of these properties, medical grade nickel metal differs from the nickel metal found in jewellery and other commercially available devices. 13
Release of the nickel ions from the device surface into the blood stream has been proposed to elicit the allergic reaction. The eluted nickel ions have been proposed to induce in-stent stenosis by accelerating neointimal hyperplasia, theorised in coronary artery stenting. 14 In coronary intervention, diminished stent patency may warrant stent revision, stent removal or autologous grafting. Such interventions may not be feasible in patients when managing their cerebrovascular pathologies. 15 However, a previously reported in-vitro study has revealed a negligible nickel release from several commonly used intracranial stents after 30 days of incubation in human plasma-like medium. 10 However, such an in vitro study has its limitations and cannot substitute for a patient's natural physiology and complex immune system.
Baranoski et al. reported a series of seven patients, four of whom had documented nickel allergies, who underwent endovascular treatment for a variety of vascular lesions. They reported no periprocedural complications and complete occlusion of the offending lesions on follow-up imaging. 16 Tonetti et al. reported two patients with cutaneous nickel allergies who underwent successful treatment with nickel-containing flow diverting stents, with no evidence of in-stent stenosis on follow-up imaging. 8 Additionally, Wallace et al. reports a series of 20 patients with metal allergies who underwent flow diverting stent treatment, and did not develop any allergic reactions. 9 While these small series describe no adverse reactions or complications with a similar experience to our own series, there are other concerning reports with undesirable outcomes.
Park et al. reported two cases of patients undergoing stent assisted coiling for unruptured aneurysms with an Enterprise VRD 2 nitinol stent (Codman, Raynham, Massachusetts, USA) who developed delayed non-ischaemic oedematous white matter lesions which resolved with corticosteroids pulse therapy. 5 There has been a similar case presented in the literature by Ulus et al., who reported a middle cerebral artery aneurysm undergoing stent assisted coiling with a ‘Y’ stenting technique, who subsequently developed reversible ischaemic parenchymal lesions. However, in this case no corticosteroids were used, and the patient's symptoms gradually improved with subsequent imaging showing complete resolution of the lesions. 6 Shotar et al. reported two similar cases of non-ischaemic cerebral enhancing lesions although the likelihood of these lesions being secondary to nickel was considered low, given their vascular distribution, but rather felt to reflect granulomatous lesions secondary to foreign body emboli. Symptoms related to nickel hypersensitivity ranged from seizures or focal neurological deficits, but all patients had complete resolution of the cerebral lesions and gradual symptom improvement, with or without systemic corticosteroids. 7
Kocer et al. reported a statistically significant association between flow diverter fish mouthing in patients with a history of contact allergy to imitation jewellery and a small aneurysmal size. However, they reported non-statistically significant association between flow diverter fish mouthing and a positive patch test. 17 In our cohort of patients, there was only one patient who experienced fish-mouthing of the proximal aspect of the Silk Vista (Balt, Montmorency, France) flow diverting stent with development of a small pontine infarction secondary to likely occlusion of a small perforating artery from the basilar artery. The association of nickel allergy and fish-mouthing of the stent in this patient remains a possibility, however further large-scale trials of nickel hypersensitive patients who have undergone flow diversion are warranted to establish a causative relationship.
In some centres, neurointerventionalists would not consider a nickel hypersensitive patient for implantation with a nitinol device and rather perform a bare coiling or refer the patient for microsurgical clipping. Although, in the context of bare aneurysm coiling without an intraluminal device, aneurysm recurrence remains a possibility. Our study highlights an alternative method of managing nickel allergic patients with a nitinol device by first assessing for a reaction at a non-critical peripheral vessel. This method should be considered by neurointerventionalists when considering treatment options for such patients.
Limitations of our study include its retrospective nature and small patient cohort. There was no standardised follow-up time post implantation of the peripheral stent and the follow-up for some patients was limited to clinical examination alone, rather than including an ultrasound examination of the stent. This may have resulted in incomplete assessment of the underlying peripheral limb stent.
Conclusion
Neurointerventionalists faced with patients self-reporting a history of nickel allergy should at the very least perform cutaneous patch-testing before ruling out an endovascular therapeutic option. Those patients with a confirmed nickel allergy who would otherwise be eligible for endovascular treatment could benefit from trial peripheral arterial stenting. This provides an alternative approach to help avoid unnecessarily eliminating certain endovascular treatment options with nickel-containing devices from which these patients may potentially still benefit. This way the optimal therapeutic choices for each patient can be made. Future work in this field should include large-scale and prospective studies to substantiate the observations made in cases series and allow confident decision making by the neurointerventionalists in the patients’ best interest.
Footnotes
Acknowledgements
The authors acknowledge the staff in the Department of Neuroradiology of The Walton Centre for their support and assistance in this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.