
Abstract
Giant, partially thrombosed intracranial aneurysms (GPTIAs) remain among the most technically challenging cerebrovascular lesions to treat, particularly in patients with associated cranial nerve or brainstem compression. Unlike microsurgical clipping with or without decompression, endovascular coiling, parent vessel flow diversion, or parent vessel occlusion, intrasaccular embolization presents a unique opportunity for immediate aneurysm occlusion and reduction of mass effect without requiring long-term antiplatelets or parent vessel compromise. However, to date, no prior intrasaccular devices were available to treat GPTIAs, including the Food and Drug Administration-approved Woven EndoBridge device which could only accommodate aneurysms up to ∼11 mm in width. Here, we present the technical feasibility, safety, and efficacy of minimally invasive endovascular intrasaccular aneurysm embolization for GPTIAs with the novel saccular endovascular aneurysm lattice (SEAL) XL device engineered with a dual-layer mesh design and an expanded size matrix aneurysms up to 20 mm in diameter. Further data from larger prospective case series are needed to validate these promising initial findings.
Keywords
Introduction
Giant, partially thrombosed intracranial aneurysms (GPTIAs) remain among the most technically challenging cerebrovascular lesions to treat. Defined as aneurysms measuring ≥25 mm in diameter and containing chronic intraluminal thrombus, GPTIAs frequently present with mass-effect symptoms such as cranial neuropathies, seizures, or focal deficits, in addition to the risk of rupture. Their complex anatomy, partial thrombosis, and associated perianeurysmal edema make treatment particularly challenging.
Traditional microsurgical clipping with or without thrombectomy and decompression carries a high surgical morbidity, particularly in elderly or medically fragile patients. Endovascular approaches (ranging from intrasaccular coiling to parent vessel flow diversion) can achieve durable occlusion and eventual shrinkage, but raise concern for potentially exacerbating cranial nerve compression and carry high recanalization rates with risk of delayed rupture. Intrasaccular flow-disrupter devices can offer immediate exclusion of the aneurysm from the circulation without permanent implants in the parent vessel and reduce the need for long-term antiplatelets, but are limited by their size, with the Food and Drug Administration (FDA)-approved Woven EndoBridge (WEB) device accommodating only aneurysms up to ∼11 mm in width.
The Saccular Endovascular Aneurysm Lattice (SEAL) by Galaxy Therapeutics is the only endovascular device available in configurations up to 20 mm, expanding the potential for intrasaccular treatments of large and giant aneurysms. Here, we present the first reported use of the world's largest intrasaccular device, the SEAL XL, to treat a giant, partially thrombosed posterior communicating segment internal carotid artery (ICA) aneurysm presenting with complete cranial nerve III palsy.
Case presentation
A 67-year-old woman with Parkinson's disease presented with a 7-month history of progressive right-sided diplopia and eyelid ptosis, culminating in inability to voluntarily open her right eye. Examination revealed a right oculomotor nerve palsy with significant ptosis and severely restricted adduction, upgaze, and downgaze. No other neurological complaints or focal deficits were noted.
Imaging
An initial outpatient magnetic resonance imaging of brain demonstrated a 28 × 23 × 25 mm3 ovoid lesion arising from the right ICA posterior communicating segment, with mixed signal on susceptibility weighted imaging consistent with partial thrombosis (Figure 1). Fluid-attenuated inversion recovery imaging revealed vasogenic edema in the adjacent medial temporal lobe with early signs of uncal herniation (Figure 1). Multiple treatment options were discussed among a multidisciplinary team of interventional neurologists and neurosurgeons and risks/benefits of each were presented to the patient and her family. A collective decision was made to proceed with endovascular intrasaccular embolization with the SEAL XL device.
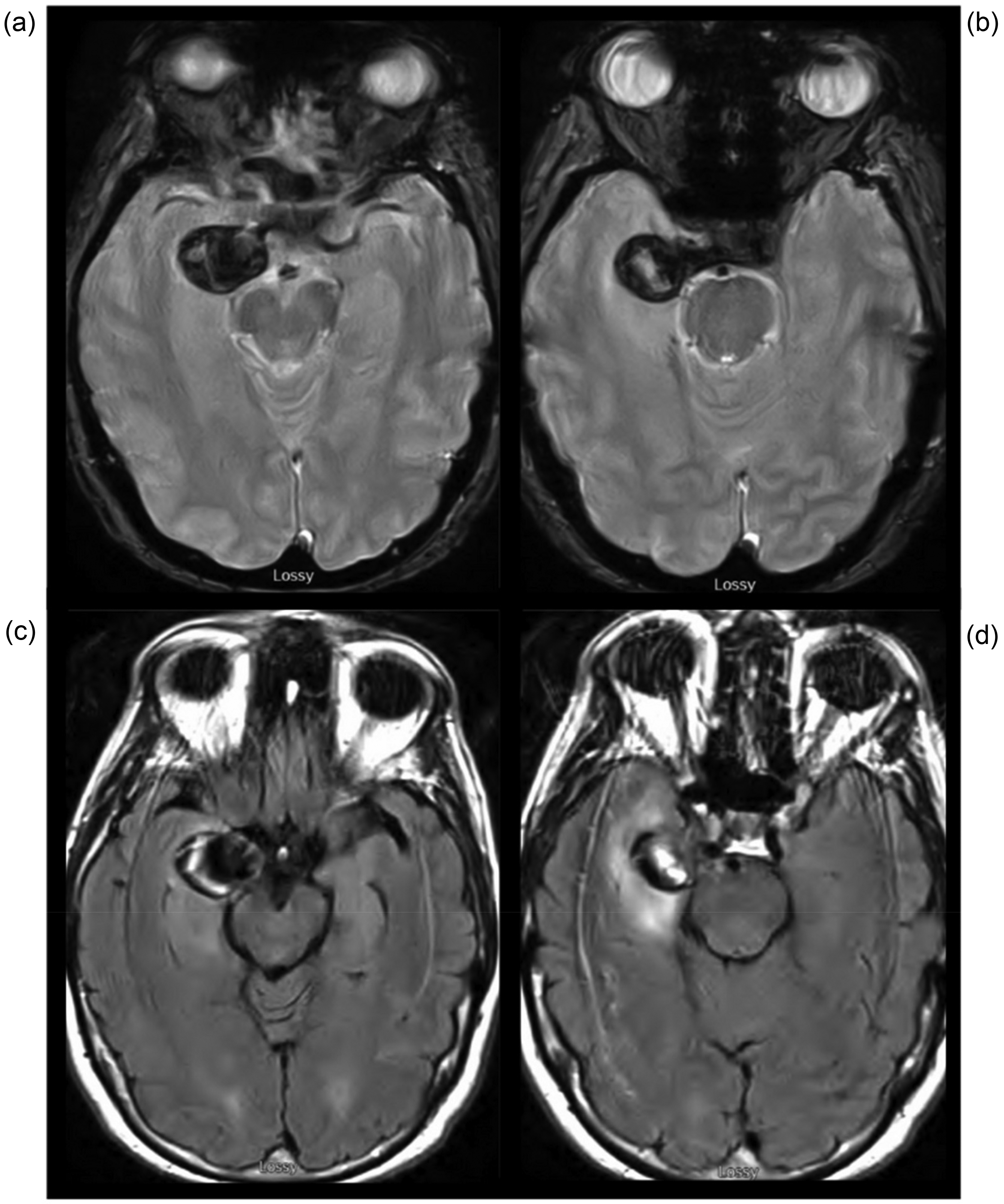
Pre-treatment magnetic resonance imaging (MRI). (a and b) Axial susceptibility weighted imaging reveals a giant right internal carotid artery aneurysm with a central flow void and a peripheral hypointense rim consistent with chronic thrombus. (c and d) Axial fluid-attenuated inversion recovery image demonstrates significant vasogenic edema in the adjacent medial temporal lobe.
Endovascular treatment
The patient was loaded with aspirin 325 mg and clopidogrel 300 mg and intubated for general anesthesia. Initial pre-treatment cerebral angiogram showed a posteriorly directed giant aneurysm in the communicating segment of the right internal carotid artery, with its contrast-opacified non-thrombosed luminal component measuring 15.93 mm in height × 10.74 mm in length with a 4.77 mm neck (see Figure 2).
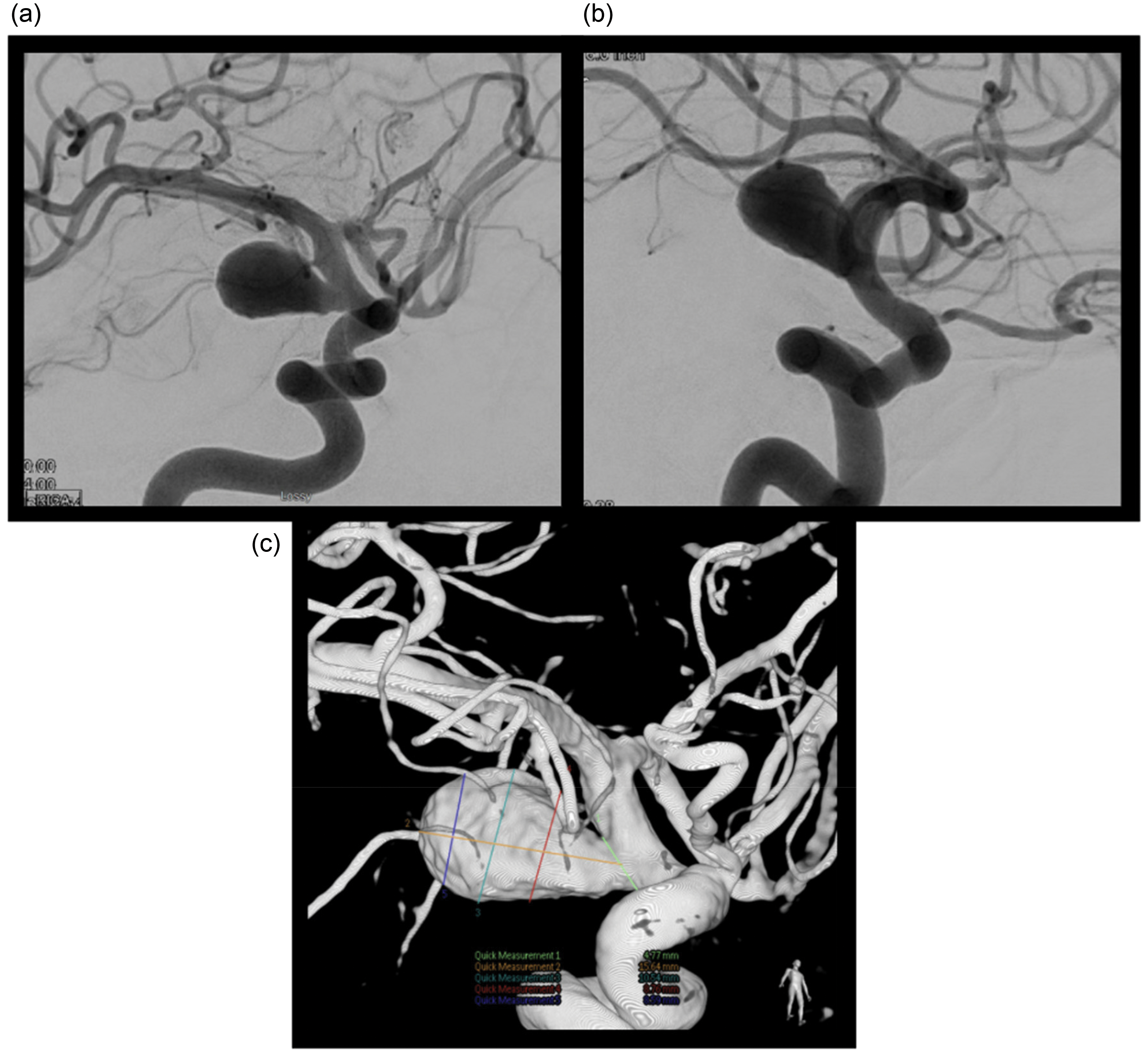
Pre-treatment digital subtraction angiography (DSA). (a) AP and (b) lateral angiographic views show the contrast-filled lumen of the giant aneurysm. (c) Three-dimensional (3D) rotational angiogram delineates the intrasaccular dimensions and aneurysm neck. Note the smaller apparent size compared to the MRI due to the non-opacification of the thrombosed portion. MRI: magnetic resonance imaging.
A 6 French Terumo Cook Shuttle, 6 French Terumo Sofia 115 cm intermediate catheter, a Terumo VIA 33 microcatheter, and a Stryker Neurovascular Synchro Support 014 pre-shaped microwire were used to obtain access into the aneurysm. The Synchro microwire was removed with the VIA 3 microcatheter in place just distal to the origin of the aneurysm neck. A SEAL XL 15 mm device was inserted and deployed into the aneurysm using the manufacturer's suggested “PUT” technique (Push forward to deploy partially until device reaches the aneurysmal dome, Unsheath to deploy the rest of the device within the aneurysm sac, and Tweak to adjust as necessary prior to detachment) (see Figure 3).
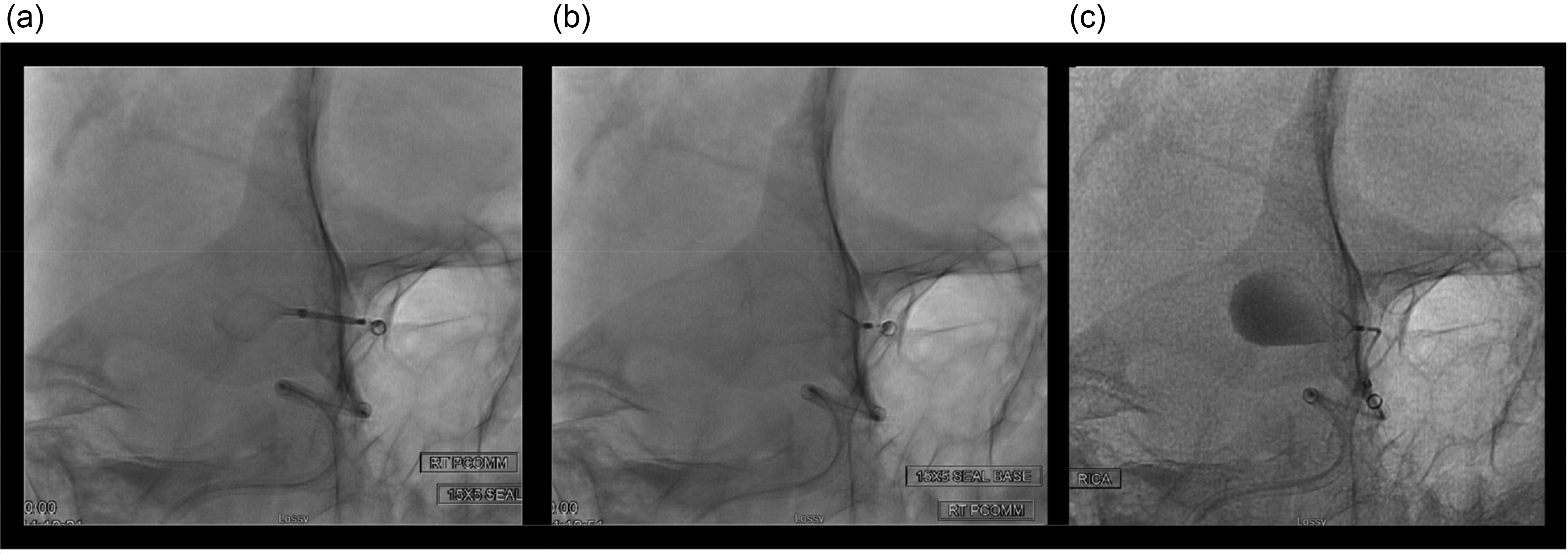
Intra-procedural views of SEAL XL device deployment. Unsubtracted images demonstrate the manufacturer's suggested “PUT” deployment technique. (a) The device is pushed forward from the microcatheter until it reaches the aneurysm dome. (b) The microcatheter is unsheathed to deploy the remainder of the device within the sac. (c) The device position is tweaked as necessary before detachment. SEAL: saccular endovascular aneurysm lattice.
Immediate post-deployment angiography demonstrated uniform device expansion and early diffuse contrast stagnation throughout the aneurysm sac (see Figure 4). Unsubtracted views confirmed appropriate device positioning without protrusion into the parent vessel (see Figure 4). A one-time dose of 10 mg dexamethasone was administered intra-operatively followed by a steroid taper over the next 5 days. Aspirin monotherapy was continued for 1 week until the follow-up angiogram.
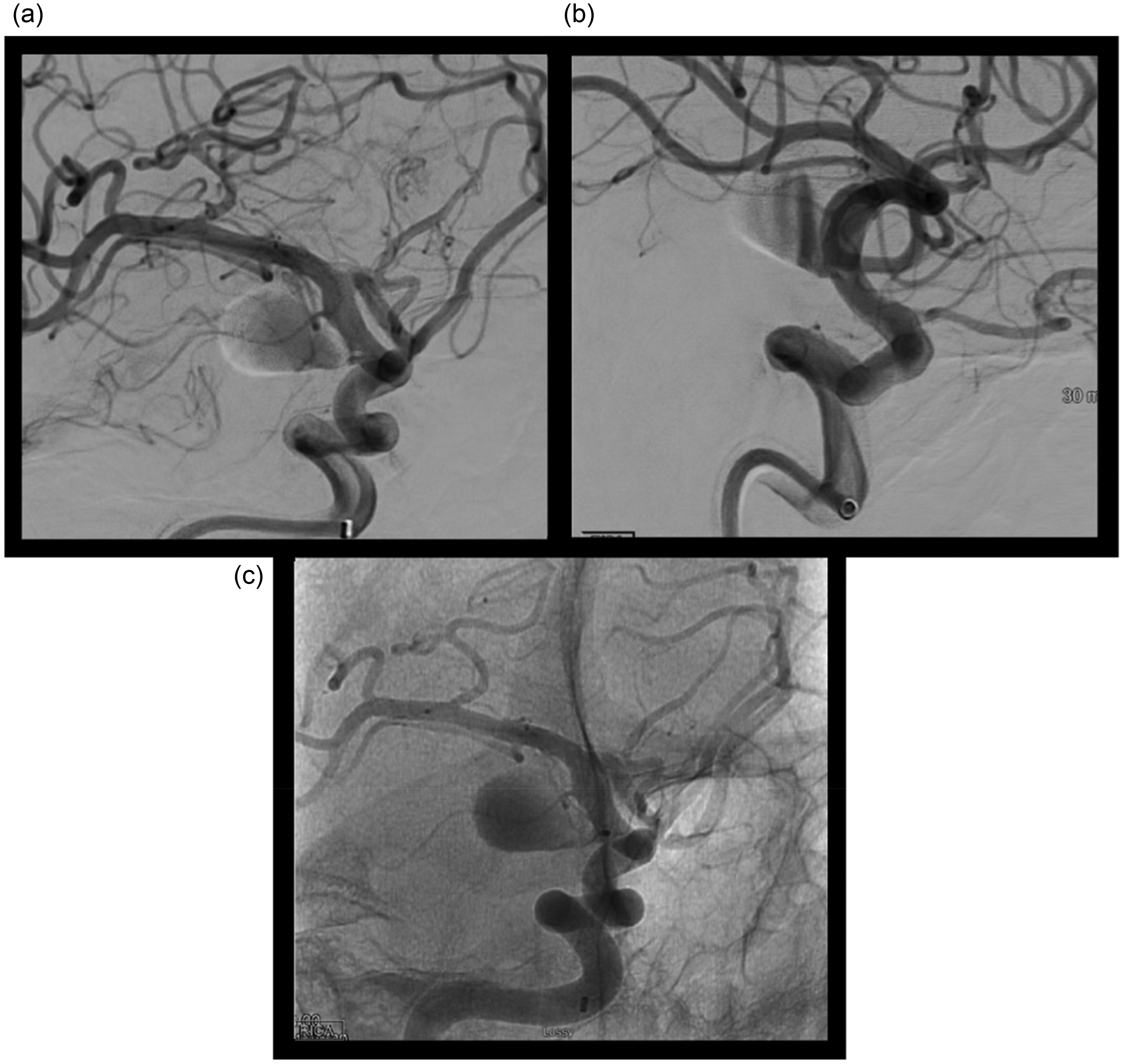
Immediate post-deployment angiography. (a) AP and (b) lateral views show immediate, diffuse contrast stagnation throughout the aneurysm sac, indicating successful flow disruption. (c) An unsubtracted view confirms the proper placement and full expansion of the 15 mm SEAL XL device. SEAL: saccular endovascular aneurysm lattice.
Follow-up
One-week follow-up angiogram revealed stable device position, complete occlusion of the aneurysm (Raymond–Roy Class I), and no stenosis or thrombus in the parent vessel (see Figure 5). The patient tolerated the procedure well without any ischemic or hemorrhagic complications. Her oculomotor nerve palsy remained stable at 1 week, and already started showing signs of partial resolution at a 2-week clinic visit with increased eyelid opening and improving diplopia (see Figure 6).
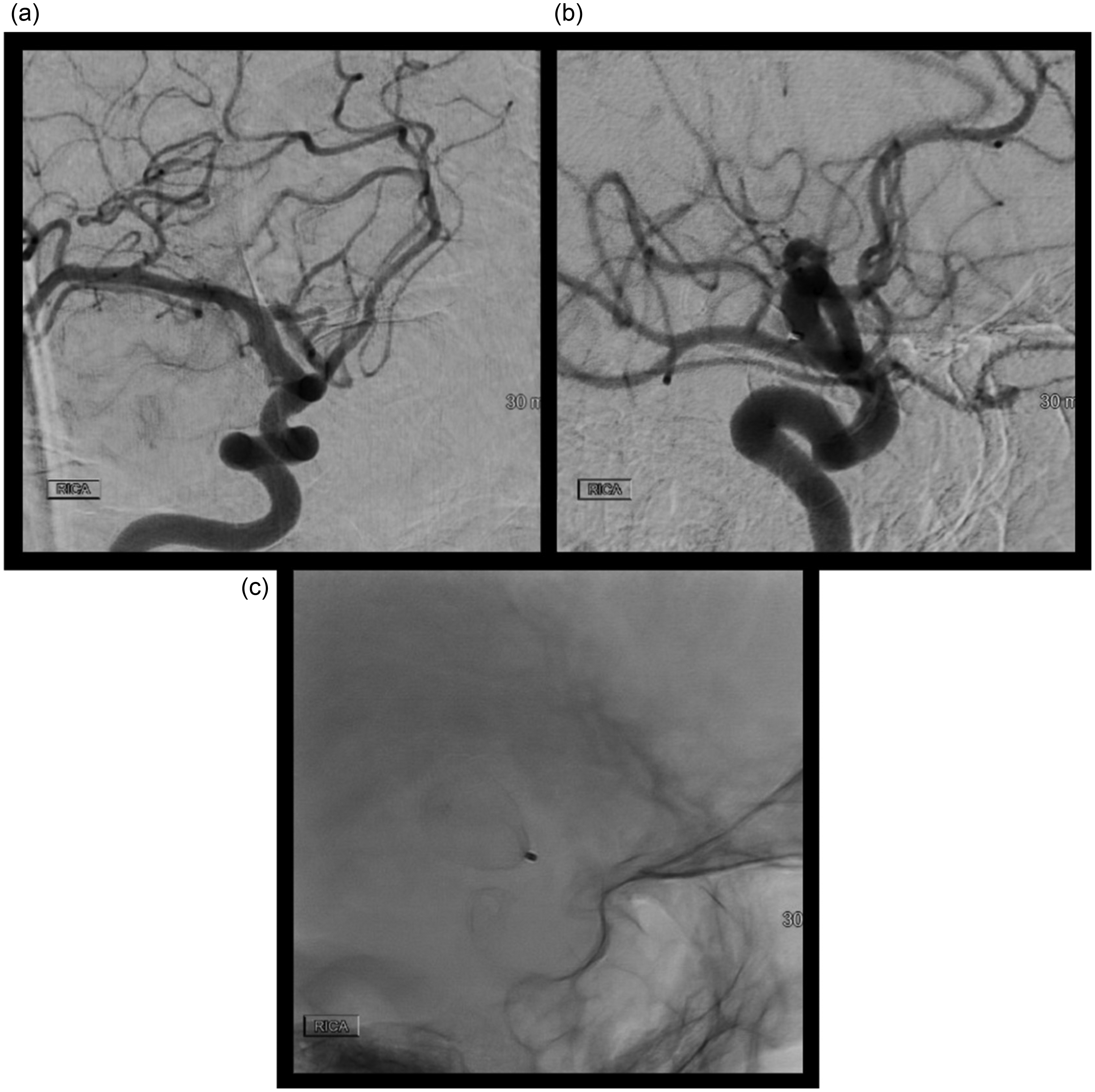
One-week follow-up angiography. (a) AP and (b) lateral views confirm complete aneurysm occlusion (Raymond–Roy Class I) with no stenosis of the parent vessel. (c) An unsubtracted single shot demonstrates a stable device position with no signs of compaction.
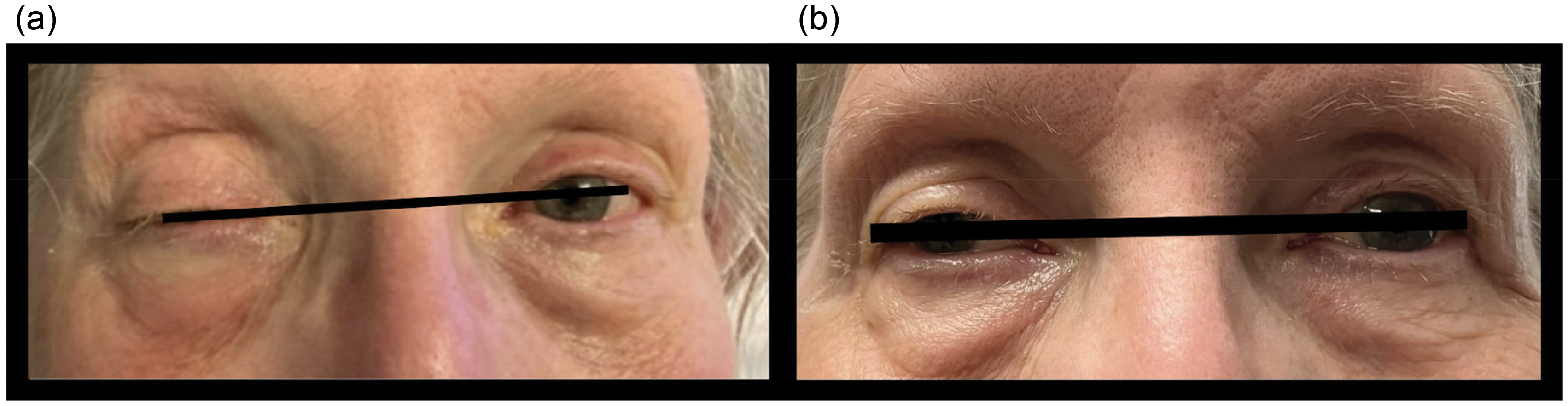
Clinical photographs of patient outcome. (a) At presentation, the patient exhibited severe right-sided ptosis and ophthalmoplegia from a complete oculomotor nerve palsy. (b) At the 2-week follow-up visit, there is marked improvement in eyelid elevation and partial recovery of ocular motility.
Written informed consent was obtained from the patient for her treatment and for the publication of this case report and its accompanying images.
Discussion
The ideal management of GPTIAs with cranial nerve compression requires both durable aneurysm occlusion and rapid alleviation of associated mass effect. 1 This case demonstrates the technical feasibility, safety, and efficacy of endovascular treatment of symptomatic GPTIAs with SEAL XL, the world's largest novel intrasaccular device.
Historically, the treatment of GPTIAs has been limited to microsurgical clipping with or without decompression, and has been associated with high periprocedural mortality. 2 Endovascular coiling has been attempted with technical success in aneurysmal occlusion, but has often failed to reduce the associated mass effect and demonstrates high rates of recanalization and coil compaction. 3 Parent vessel sacrifice, an extreme option for aneurysmal exclusion, is only feasible for a select minority of patients who can tolerate the procedure without having a large disabling ischemic stroke. 3
Flow diversion in the parent vessel has emerged as a superior endovascular alternative, demonstrating higher rates of durable occlusion and eventual aneurysm shrinkage. 4 However, for symptomatic patients with cranial nerve and brainstem compression, the protracted aneurysm remodeling timeline, risk of delayed post-procedural hemorrhage, and necessity for long-term dual antiplatelet therapy remain significant drawbacks.5,6
Intrasaccular devices offer a fundamentally different therapeutic profile, allowing for immediate flow disruption within the aneurysm sac. However, existing devices have been limited in size, with the FDA-approved WEB accommodating only aneurysms up to ∼11 mm in width. 7 The SEAL XL device, engineered with a dual-layer mesh design and an expanded size matrix aneurysms up to 20 mm in diameter, is currently under investigation for addressing this gap in the treatment of GPTIAs.8,9
When considered within the spectrum of intrasaccular flow-disruption devices, the SEAL system demonstrates both shared principles and distinct engineering advances. The WEB system, first developed in 2010, is a three-dimensional braided mesh designed for volumetric aneurysm filling. Its lateral compression-based stability necessitates complex sizing adjustments to accommodate predictable elongation, and its maximum diameter of ∼11 mm limits use in large or giant lesions. 10 The Contour Neurovascular System employs a shallow, cup-like, dual-layer mesh optimized for neck reconstruction while leaving most of the sac unoccupied, thereby simplifying sizing but restricting applicability to smaller, proximal morphologies. 11 The Artisse device incorporates a flexible flared-basket or spheroidal configuration with an atraumatic tip, improving conformability and dome safety, though similarly limited to smaller aneurysms. 12 In contrast, the SEAL platform introduces structural specialization through two configurations: a shorter “Base” optimized for shallow or irregular aneurysms, and a taller “Arc” incorporating an anchoring loop for deeper aneurysmal sacs. Both utilize a dual-layer mesh reinforced with a platinum core, extending the available size matrix up to 20 mm. These features enable SEAL to address a broader range of aneurysm anatomies, including large and giant lesions, while maintaining an intrasaccular-only treatment paradigm. 8
In the presented case, the intrasaccular SEAL XL device achieved immediate and complete occlusion on follow-up angiography without parent vessel compromise. Notably, the patient demonstrated early cranial nerve improvement despite theoretical concerns that intrasaccular thrombosis could exacerbate mass effect in partially thrombosed aneurysms. 13 The swift improvement suggests that the immediate elimination of arterial pulsatility against the oculomotor nerve may be a dominant mechanism for early recovery, a phenomenon that has been previously reported following endovascular treatments. 14
This proof-of-concept case demonstrates the technical feasibility, safety, and efficacy of minimally invasive endovascular intrasaccular aneurysm embolization for GPTIAs with the novel SEAL XL device. Further data from larger prospective case series are needed to validate these promising initial findings.
Footnotes
Ethical approval
This case report was conducted in accordance with ethical standards. Institutional review board approval was not required as the report contains no personal identifying information beyond what is necessary for the case presentation, and the treatment was performed as part of standard clinical care.
Informed consent
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images.
Author contributions
Amit Chaudhari and Rashed Kamal were the primary authors responsible for the writing of the manuscript. Amit Chaudhari, Eugene Lin, and Darwin G Ramirez-Abreu were directly involved in the clinical care of the patient. Zachary M Rosenstein assisted with the revisions of the manuscript. Eugene Lin, David J Altschul, Brian T. Jankowitz, and Boris Pabón provided senior review and revisions of the manuscript. Osama O Zaidat provided overall project supervision. All authors have read and approved the final manuscript for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study are available within the article.