
Abstract
Background
Endovascular therapy (EVT) improves functional outcomes and reduces mortality in acute ischemic stroke (AIS) due to basilar artery occlusion (BAO). However, data on hemorrhagic complications and nonneurologic adverse events remain limited. We conducted a systematic review and meta-analysis to assess these outcomes in randomized controlled trials (RCTs) comparing EVT versus best medical management (BMM).
Methods
We searched PubMed, Cochrane Library, and Embase in December 2024 for RCTs comparing EVT and BMM (PROSPERO registry CRD42024617681). Outcomes included any parenchymal hematoma (PH), PH type 1 and 2, subarachnoid hemorrhage (SAH), systemic/extracranial hemorrhage, pneumonia, and heart failure. Pooled risk ratios (RR) with 95% confidence intervals (CI) were calculated using a random-effects model.
Results
Four RCTs, 988 patients (556 EVT, 432 BMM), were included. EVT increased the risk of SAH (RR 5.14; 95% CI [1.35–19.56]; I² = 0.0%) and PH type 2 (RR 5.53; 95% CI [1.47–20.84]; I² = 0.0%) compared to BMM. No significant differences were observed for any PH (RR 1.91; 95% CI [0.92–3.97]; I² = 0.0%), PH type 1 (RR 0.71; 95% CI [0.22–2.29]; I² = 3.4%), systemic/extracranial hemorrhage (RR 1.06; 95% CI [0.71–1.60]; I² = 12.2%), pneumonia (RR 1.00; 95% CI [0.83–1.21]; I² = 0.0%), or heart failure (RR 2.00; 95% CI [0.34–11.92]; I² = 55.4%).
Conclusion
In patients with BAO AIS, EVT is associated with an increased risk of SAH and PH type 2 compared with BMM. There was no significant difference in any PH, PH type 1, systemic/extracranial hemorrhage, pneumonia, and heart failure between groups.
Introduction
Basilar artery occlusion (BAO) is a relatively uncommon cause of acute ischemic stroke (AIS) but is associated with disproportionately severe outcomes. Poor collateral supply of the perforator branches to the brainstem and cerebellum contributes to the catastrophic clinical course, with reported mortality rates ranging from 40% to 80% and significant long-term disability among survivors.1–6
Following the landmark endovascular theraphy (EVT) trials in 2015, EVT became the standard of care in selected patients with large vessel occlusion (LVO) AIS.7–11 Subsequent studies extended EVT indications to include late time windows and larger ischemic cores.12–14 However, these studies focused on anterior circulation AIS, leaving uncertainty regarding the efficacy of EVT for BAO.
Although EVT has been performed in the posterior circulation LVO (PC-LVO) since the early 1980s, 15 the real impact of this intervention remained presumed. The first two trials that compared EVT and best medical management (BMM), “the Basilar Artery International Cooperation Study (BASICS)” and “Acute Basilar Artery Occlusion: Endovascular Intervention vs Standard Medical Treatment (BEST) trial,” failed to provide high-level evidence to support EVT superiority.16,17
More recently, the “Endovascular Treatment for Acute Basilar-Artery Occlusion” (ATTENTION) and “Basilar Artery Occlusion Chinese Endovascular” (BAOCHE) trials demonstrated that EVT significantly improved functional outcomes and lowered compared to BMM.18,19 These findings were further supported by VERITAS, an individual patient level meta-analysis, which confirmed a robust reduction in functional disability and mortality with EVT. 20 While functional and mortality outcomes have been increasingly studied, data on safety endpoints—including intracranial hemorrhage and systemic complications—remain limited. To address this gap, we performed a systematic review and meta-analysis of randomized trials comparing EVT to BMM in BAO AIS, focusing on hemorrhagic and nonneurologic safety outcomes.
Methods
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Statement guidelines and the Cochrane Collaboration Handbook for Systematic Reviews of Interventions guidelines. The protocol was prospectively registered with the International Prospective Register of Systematic Reviews (CRD42024617681).
Eligibility criteria
Studies were eligible for inclusion if they met the following criteria: (1) randomized controlled trial (RCT) design; (2) adult patients with BAO-related AIS within 24 h of symptom onset; (3) comparison of EVT versus BMM; (4) reported at least one relevant safety outcome. No restrictions were placed on publication date or patient demographics.
Exclusion criteria included: (1) observational or nonrandomized designs; (2) anterior circulation ischemic strokes; (3) non-English publications; (4) reviews, letters to editors, and conference abstracts; and (5) failure to report any of the outcomes pertinent to this analysis.
Search strategy and data extraction
A comprehensive and systematic search was conducted in the Cochrane Central Register of Controlled Trials, PubMed/MEDLINE, and Embase databases from their inception to the final search date of (“Basilar artery ischemic stroke” OR “basilar artery occlusion” OR “basilar artery thrombosis” OR “vertebrobasilar ischemia” OR “Basilar artery stroke”) AND (“mechanical thrombectomy” OR “thrombectomy” OR “endovascular thrombectomy” OR “mechanical clot retrieval” OR “endovascular clot removal” OR “stent-triever” OR “aspiration”) AND (“best medical management” OR “standard medical care” OR “medical treatment” OR “medical management” OR “conservative management” OR “optimal medical therapy” OR “best medical treatment”). Three authors independently performed the systematic review, with any disagreements resolved through panel discussions among the authors. The study selection process involved an initial screening of titles and abstracts, followed by a full-text evaluation of potentially eligible studies.
Two authors independently extracted data using a double-blinded approach, reviewing primary reports and supplementary materials to systematically capture all relevant information. Any discrepancies were resolved by consensus or, if needed, by consulting other review team members.
Quality assessment
The risk of bias and quality assessment of the included studies was conducted using the Risk of Bias 2 (RoB 2) tool. Outcome data were collected following an intention-to-treat approach. The risk of bias evaluation was independently performed by two authors, with any discrepancies resolved through consensus after a thorough discussion of the differing assessments.
Outcomes, definitions, and subanalyses
The assessed outcomes included: (1) Any Parenchymal hematoma (PH), (2) Parenchymal hematoma type 1 (PH1), (3) Parenchymal hematoma type 2 (PH2), (4) Subarachnoid hemorrhage (SAH), (5) Systemic/Extracranial Hemorrhage, (6) Pneumonia, (7) Heart failure.
Statistical analysis
Endpoints were analyzed using risk ratios (RRs) with 95% confidence intervals (CIs). Heterogeneity was assessed using the Cochrane Q statistic and Higgins and Thompson's I², with the restricted maximum-likelihood estimator. Heterogeneity was classified as significant if greater or equal to 40%. A random-effects model was applied to account for variability in effect sizes across studies. Prespecified subgroup interactions were evaluated using the Q test, assuming no interaction between groups, and reported as p-values. All p-values are two-sided, and no adjustments were made for multiple comparisons. Statistical analyses were conducted using R version 4.3.2 (R Core Team, Vienna, Austria) with the meta package.
Results
Search results and patient characteristics
As detailed in Figure 1, our initial search retrieved 165 studies after removing duplicates; 144 studies were excluded after the initial critical examination of the title and abstract. After a full-text review of the remaining publications, four RCTs that assessed EVT efficacy in BAO (BEST, BASICS, ATTENTION, and BAOCHE) were included, comprising 988 patients.16–19
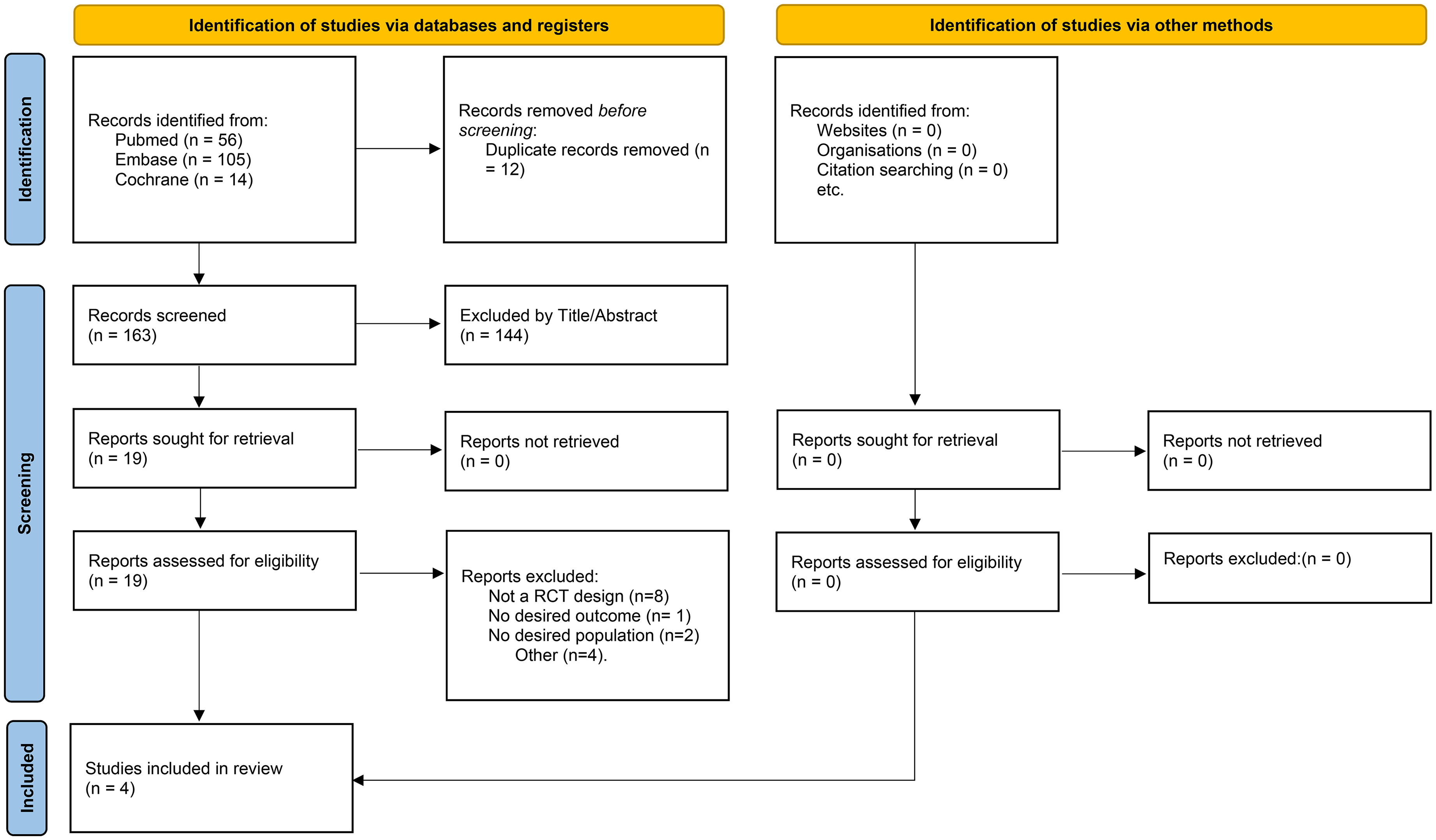
PRISMA flow diagram study screening and selection.
Compiling the four RCTs, we obtained 556 patients assigned to the EVT arm and 432 to the BMM arm to treat BAO. Individual study participants’ baseline characteristics were mostly well-balanced among studies and are displayed in Table 1.
Characteristics of patients at baseline.
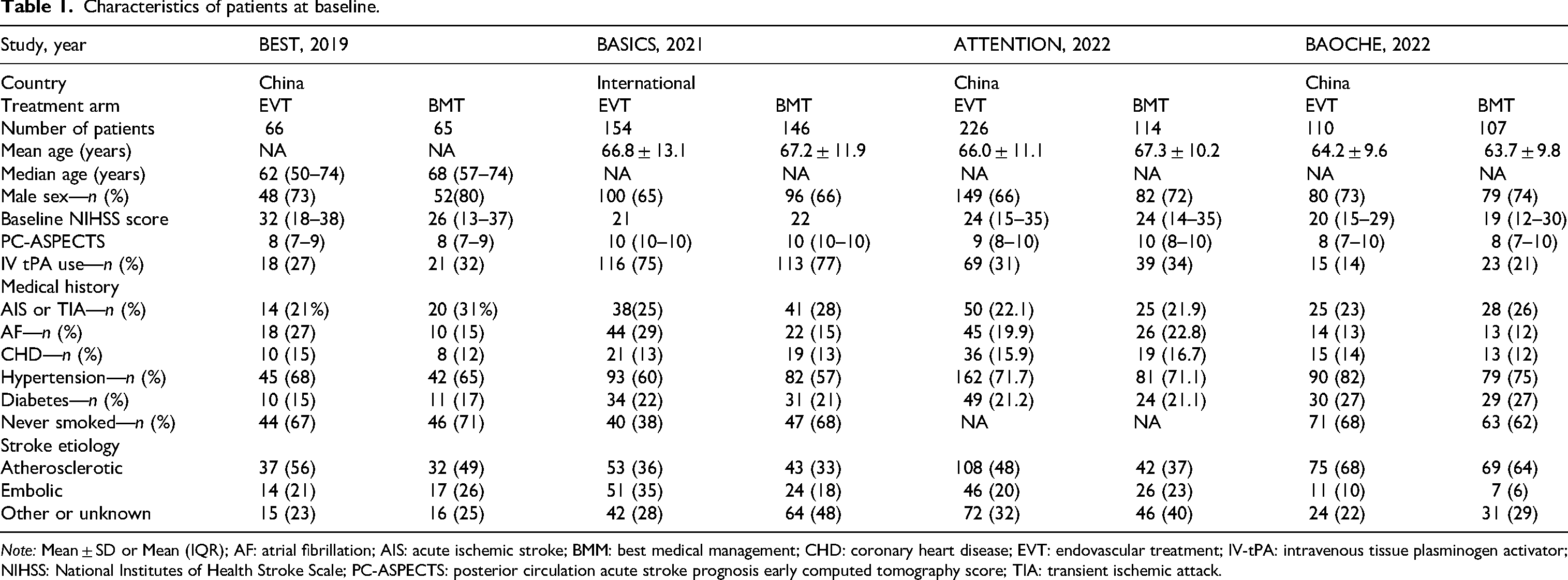
Note: Mean ± SD or Mean (IQR); AF: atrial fibrillation; AIS: acute ischemic stroke; BMM: best medical management; CHD: coronary heart disease; EVT: endovascular treatment; IV-tPA: intravenous tissue plasminogen activator; NIHSS: National Institutes of Health Stroke Scale; PC-ASPECTS: posterior circulation acute stroke prognosis early computed tomography score; TIA: transient ischemic attack.
Pooled analysis of all studies
The meta-analysis results revealed varying outcomes for different complications when comparing endovascular treatment and BMM, as specified in Figure 2. In a meta-analysis of four RCTs, the incidence of any PH did not differ significantly between the two groups (relative risk 1.91; 95% CI [0.92–3.97]; I² = 0.0%). Similarly, the incidence of PH1, analyzed in three RCTs, was not statistically significantly different (relative risk 0.71; 95% CI [0.22–2.29]; I² = 3.4%).
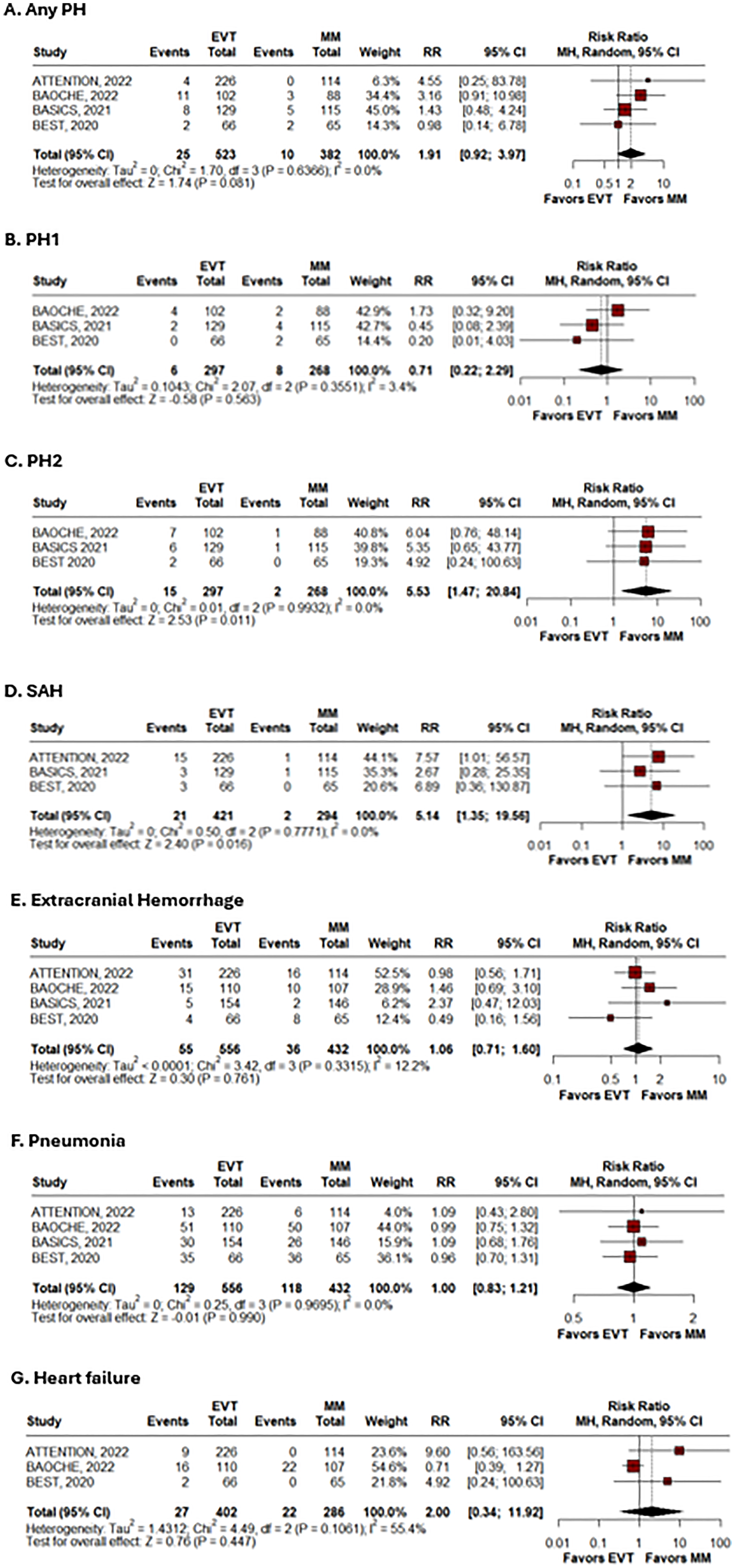
Forest plot comparing the odds of safety outcomes between endovascular treatment and best medical management in basilar artery occlusion. Outcomes include any parenchymal hematoma (A), PH1 (B), PH2 (C), subarachnoid hemorrhage (D), extracranial hemorrhage (E), pneumonia (F), and heart failure (G). Odds ratios with 95% confidence intervals are presented for each outcome.
However, based on three RCTs, PH2 was significantly more frequent in the endovascular treatment group (relative risk 5.53; 95% CI [1.47–20.84]; I² = 0.0%). Moreover, pooling three RCTs, the incidence of SAH was also significantly higher in the endovascular treatment group compared to the BMM group (relative risk 5.14; 95% CI [1.35–19.56]; I² = 0.0%).
Regarding nonneurologic outcomes, extracranial hemorrhage showed no significant difference between the two groups in four RCTs (relative risk 1.06; 95% CI [0.71–1.60]; I² = 12.2%). Pneumonia rates were similar between the groups in the meta-analysis of four RCTs (relative risk 1.00; 95% CI [0.83–1.21]; I² = 0.0%). Lastly, the incidence of heart failure was not statistically different between the groups, based on three RCTs (relative risk 2.00; 95% CI [0.34–11.92]; I² = 55.4%).
Quality assessment
From the four studies analyzed, only one presented “some concerns” for risk of bias according to the ROB 2 assessment, 17 mainly due to concerns about the “deviations from intended interventions” (ROB 2 domain 2). The other three studies presented a low risk of bias.15,17,18 Individual study appraisal of all domains is shown in Figure 3.
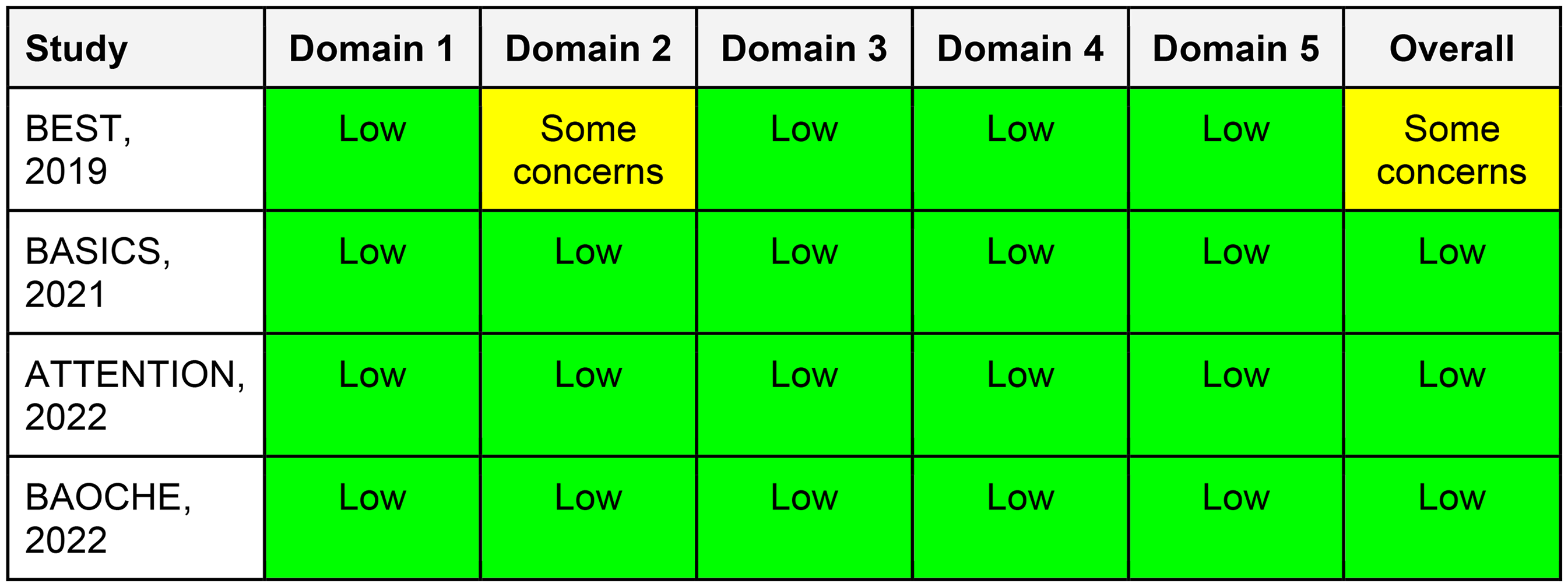
Risk of bias 2 (ROB 2) assessment of individual studies. Domain 1: Randomization process; Domain 2: Deviations from intended interventions; Domain 3: Missing outcome data; Domain 4: Outcome measurement; Domain 5: Selection of the reported result.
Discussion
In this systematic review and meta-analysis of four RCT studies, we compared the safety outcomes of AIS patients with BAO treated with EVT versus BMM. Our main findings were: (1) patients who underwent EVT were at a significantly higher risk of SAH and parenchymal hematoma type 2 compared to patients who had BMM, and (2) there were no significant differences between groups in: any parenchymal hematoma, parenchymal hematoma type 1, pneumonia, systemic/extracranial hemorrhage and heart failure.
For many years, the benefit of EVT in BAO was presumed rather than demonstrated. The VERITAS collaboration—an individual patient level meta-analysis pooling data from the BEST, BASICS, ATTENTION, and BAOCHE trials—provided robust evidence supporting EVT for BAO AIS.15–18 The study found that EVT significantly improved outcomes in patients with vertebrobasilar artery occlusion with moderate to severe symptoms, with a 2.5-fold increased likelihood of achieving a favorable functional outcome (mRS 0–3 at 90 days). EVT resulted in significant reductions in overall disability (adjusted cOR 2.09 [1.61–2.71]; p < .0001) and mortality (aOR 0.60 [0.45–0.80]; p < .0001) at 90 days across multiple subgroups, despite a higher risk of symptomatic intracranial hemorrhage (SICH) (aOR 11.98, 95% CI [2.82–50.81]; p < .0001). 20 However, the benefit of EVT for patients presenting with mild stroke severity (NIHSS <10) and extensive infarcts on neuroimaging remains poorly explored. Additionally, a secondary safety outcomes analysis pooling data from these four RCTs,16–19 which were not included in previous meta-analyses, warranted further investigation.
Previous studies on post-EVT SAH have yielded mixed results, with some indicating SAH as an independent risk factor for poor outcomes. In contrast, others suggest it may be clinically benign.21–24 However, much of the existing literature is based on data from high-volume academic centers and clinical trials, which may not reflect routine clinical practice. 25 An analysis of a U.S. national database of 99,219 EVT patients found that 6.2% (6174) experienced SAH. Moreover, SAH was independently associated with higher in-hospital mortality (21.5% vs 10.6%, adjusted OR 2.53, 95% CI [2.23–2.87], p < .001) and lower odds of routine discharge with self-care (18.2% vs 28.0%, aOR 0.58, 95% CI [0.52–0.65], p < .001). Factors associated with increased odds of SAH included distal/medium vessel occlusion, coagulopathy, angioplasty or stenting, concurrent intraparenchymal hemorrhage, and female sex. 26
We observed a higher frequency of SAH in EVT patients group (RR 5.14, 95% CI [1.35–19.56]; p = .016), but this radiological finding did not correlate with an increase in mortality or worse functional independence at 90 days (mRS 0–3). 20 This association could suggest that many of these radiological SAHs may be clinically benign, aligning more with contrast extravasation than with true hemorrhagic complications. A previous study that analyzed post EVT dual-energy CT in anterior circulation found 49.2% of cases presenting isolated contrast extravasation, but SAH cases were not associated with worse functional outcomes nor with mortality. 27 Thereafter, this observation is reassuring for clinical practice, as it suggests that EVT-related SAH found in the RCTs does not necessarily translate into worse prognosis.
We also found that the EVT treatment arm for BAO was associated with a significantly higher risk of developing PH2 (RR 5.53, 95% CI [1.47–20.87]; p = .011), which is linked to poor outcomes, presumably due to mass effect and herniation. A retrospective multicenter study identified the number of passes during mechanical thrombectomy as a predictor of postprocedural PH and PH2 in high ischemic core AIS in the anterior circulation, likely due to local vessel injury and blood–brain barrier disruption. However, this association was not observed in patients without extensive infarction at baseline.28–30
Although data on risk factors for PH and its influence on outcomes in patients with posterior circulation AIS are limited, the pathophysiological mechanisms underlying PH have been previously described. These involve disruption of the blood–brain barrier, cytotoxic injury, and preexisting cerebral small vessel disease in older patients. Such processes can lead to mass effect, potentially compromising adjacent healthy parenchyma and subsequently impairing functional recovery. 31 In this context, a more nuanced understanding of the increased risk of intracranial bleeding may be gained through stratified analyses of blood–brain barrier disruption factors, such as the number of passes and the EVT technique used (aspiration, stent retriever, or a combination of both). 32
Our study did not show significant differences between treatment groups for other types of intracranial bleeding: any PH (RR 1.91, 95% CI [0.92–3.97]; p = .081) and PH1 (RR 0.71, 95% CI [0.22–2.29]; p = .563). Prior meta-analyses have focused on SICH as a clinically meaningful endpoint. Our study extends these findings by examining radiological subtypes, and, although not all PH are clinically symptomatic, their detection often influences clinical management decisions. 33
From a clinical management standpoint, PH2 frequently prompts escalation of neurocritical care, initiation of intracranial pressure-directed therapies, or withholding of anticoagulation/antiplatelet treatment.33,34 Identifying PH2 as the radiological correlate of SICH helps refine post-EVT monitoring and informs risk–benefit discussions with patients and families. Furthermore, even after accounting for PH2 risk factors, the variance in SICH occurrence remains largely unexplained and unpredictable, 35 and asymptomatic bleedings were associated with poorer functional outcomes and higher mortality in anterior circulation AIS, suggesting that any intracranial hemorrhage should be considered as an additional EVT safety measure regardless of symptomatology. 36 Herein, our study extends the clinical relevance of prior SICH-focused analyses by providing a more granular understanding of which hemorrhage subtypes matter most in BAO EVT, but prognosis data for each hemorrhage subtype in posterior circulation EVT remains limited.
Following acute interventions, such as intravenous thrombolysis and endovascular therapy, systemic complications are common in patients with BAO AIS in the intensive care department. However, studies on these complications are limited and rarely included in systematic reviews or meta-analyses. This study aimed to fill that gap but found no significant differences in outcomes between treatment groups for heart failure (relative risk 2.00, 95% CI [0.34–11.92]; p = .447), pneumonia (relative risk 1.00, 95% CI [0.83–1.21]; p = .99), and extracranial hemorrhage (relative risk 1.06, 95% CI [0.71–1.60]; p = .761). Although these findings may not impact eligibility for endovascular treatment, they enhance the evidence base by addressing clinical outcomes routinely managed in neurocritical care settings, suggesting that EVT does not increase these complications.
To the best of our knowledge, this is the first meta-analysis to examine the secondary safety outcomes of EVT versus BMM in BAO AIS patients, focusing on the etiology of intracranial bleeding and systemic complications. The included studies involved both stent-retriever and aspiration techniques, supporting the generalizability of our findings.
Our study has limitations. Firstly, the lack of individual-level patient data precluded subgroup analyses based on BAO etiology, ischemic core size, number of EVT passes, age, precise intravenous thrombolysis type used, clot removal technique (aspiration vs stent-retriever), post procedure blood pressure parameters, recanalization score, and arterial access site (radial vs femoral artery). Second, several potentially relevant complications—such as subdural or intraventricular hemorrhage, malignant brain edema, acute respiratory failure, acute renal insufficiency, and cardiac ischemia—could not be analyzed due to limited reporting or event rarity. Finally, the increased frequency of SAH in EVT group should be interpreted with caution, as none of the included RCTs uniformly employed dual-energy CT or equivalent confirmatory modalities to differentiate blood from contrast extravasation. Thus, part of the observed SAH signal may reflect contrast staining related to blood–brain barrier disruption rather than true hemorrhage.
Conclusion
In conclusion, this meta-analysis adds to the growing body of evidence supporting EVT for BAO AIS by focusing on safety outcomes. EVT was associated with significantly higher risks of SAH and parenchymal hemorrhage type 2 but showed no significant differences in any parenchymal hemorrhage or type 1, extracranial hemorrhage, pneumonia, and heart failure. Overall, EVT is safe and highly beneficial, but the increased risk of SAH and PH2 should be considered in treatment planning and consent discussions.
Footnotes
ORCID iDs
Ethics statement
Ethics approval was not required for this case report per institutional guidelines.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosures
The authors have no personal, financial, or institutional interest in any of the drugs, materials, or devices described in this article.