
Abstract
Introduction
Mechanical thrombectomy (MT) techniques affect procedure lengths and radiation exposure, with both reduced with contact aspiration (CA) compared to combination stentriever-assisted aspiration (SA). Monopoint MT has higher first pass effect (FPE) rates, less technical crossover, and recanalization with fewer passes. Monopoint MT may thus be associated with shorter procedural times and less radiation.
Materials/Methods
Anterior circulation large vessel MT cases across four centers were identified, assigning cases to Monopoint, CA, or SA groups based on the first-line technique employed, excluding cases that could not be assigned to one of these three groups. Clinical variables, technical details, times to first and final pass, fluoroscopy time, dose-area product (DAP), and radiation dose were recorded. Univariable and multivariable analyses were performed to compare procedural times and radiation data among treatment groups.
Results
Seventy-seven Monopoint, 32 CA, 42 SA cases were analyzed. Time to first pass was shortest with Monopoint (p < 0.001), as was time to final pass (p < 0.001). There was no significant difference in fluoroscopy time between Monopoint (17.7 min) and CA (17.6, p = 0.835); both were lower than SA (26.4, p < 0.001). DAP was lowest for Monopoint (18,854 µGy*m2) compared to CA (31,325) and SA (29,483, p < 0.001). Radiation dose was lowest with Monopoint (884 mGy) compared to CA (1095) and SA (1994, p < 0.001).
Conclusion
MT for anterior circulation large vessel occlusions had shorter procedural times and involved less radiation with Monopoint compared to CA and SA. Further investigation is warranted to assess other clinical and technical factors that affect procedure duration, DAP, and radiation dose.
Introduction/Purpose
As endovascular therapy for the treatment of acute ischemic stroke (AIS) has become standard of care, devices and techniques have evolved rapidly.1–17 As mechanical thrombectomy (MT) techniques have advanced, the efficiency with which these procedures can be performed has also increased. The use of different devices may affect such efficiency, which can be measured in both procedural time metrics and radiation data.
Neurointerventional procedures involve exposure to ionizing radiation for the patient, the operating physician, and procedural staff in the angiography suite.18–24 Previous investigations of radiation metrics in the neurointerventional setting have shown trends in which greater exposure and dose are associated with increased procedural complexity and longer fluoroscopy times.18–24 These findings have been confirmed in studies of MT, with higher exposure occurring when an operator has less experience, when more MT passes are required, and in the setting of basilar occlusion as opposed to middle cerebral artery occlusion.18,20–24 Concerted efforts and protocol adjustments can result in reduced radiation exposure and dose. 23 MT techniques can affect radiation, with lower exposure when contact aspiration (CA) is used compared to combination stentriever/aspiration (SA). 22
The Monopoint system (Route 92 Medical, San Mateo, CA) consists of the 8-French Base Camp guide sheath, the HiPoint 88 catheter-extender, and the Tenzing 8 delivery device. Investigations of MT performed with the Monopoint system have demonstrated higher rates of first pass effect (FPE), less need for crossover to alternative techniques, and fewer passes to achieve recanalization.10,11,13,16,17 It is hypothesized that MT with Monopoint will be associated with shorter procedural temporal metrics and lower radiation exposure and dose. This analysis compares such variables among MT procedures performed with the Route 92 0.088″ Monopoint system, CA, with 0.060–0.072″ inner diameter (ID) devices, or SA.
Materials/Methods
According to an IRB-approved protocol, retrospective analysis was performed of AIS patients treated with MT across four high-volume stroke centers in a regional health system. Querying prospectively maintained treatment records, patients with large vessel occlusion (LVO) of the ICA terminus or M1 segment of the middle cerebral artery were identified. Patient demographics, clinical presentation, angiography suite, procedure date, operator, LVO location, technique, and equipment utilized were noted. Patients were assigned to one of three technical cohorts based on the first-line technique chosen— Monopoint, CA, or SA. MT procedures were performed in six different angiography suites among the four sites. Biplane equipment includes Artis Z, Artis Q, and Icono units from Siemens (Siemens Healthineers, Erlangen, Germany), and Philips Allura units (Philips, Eindhoven, the Netherlands). Fluoroscopy protocols were not changed during the study period. Patients requiring rescue/bailout stenting for atherosclerosis and patients treated with a first-line MT technique not clearly within one of the three above-described cohorts were excluded to limit confounding. Times noted for arterial access, first pass, and final pass were all recorded. Fluoroscopy time, dose-area product (DAP), and radiation dose were all tabulated based on procedure logs generated by angiography equipment at the completion of the procedure. Time to first pass and time to final pass were defined as the duration between arterial access and first pass and final pass, respectively. To compare procedural times, radiation data, and the number of MT passes among treatment groups, paired t-tests were performed. Fisher's exact test was performed to assess crossover to a different technique and rates of FPE and final eTICI 2c/3. Mixed effects linear regression was then performed for multivariable analysis of continuous dependent variables and logistic regression analysis for non-continuous variables, removing any independent variables with p > 0.20 in univariable tests to account for possible residual confounding.
Results
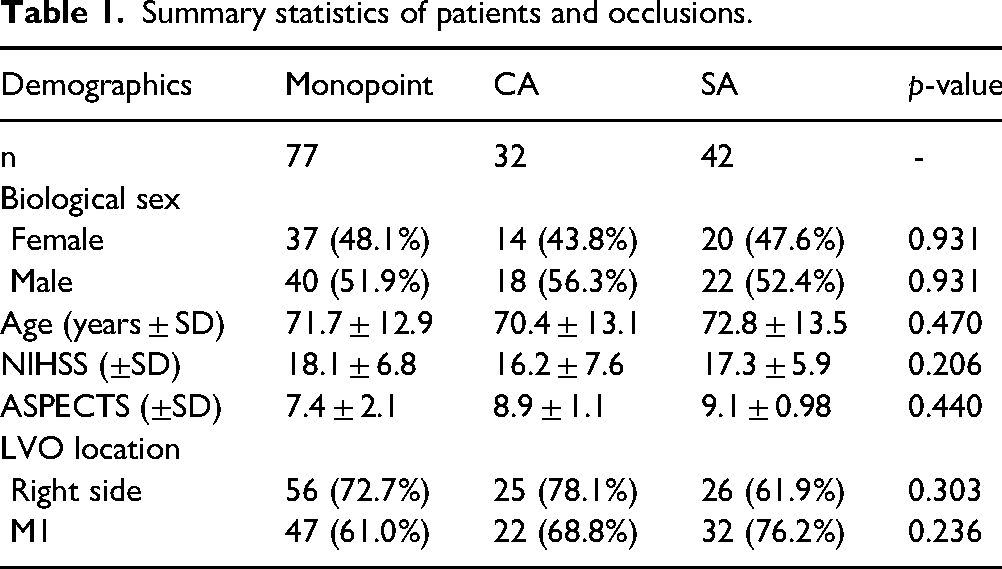
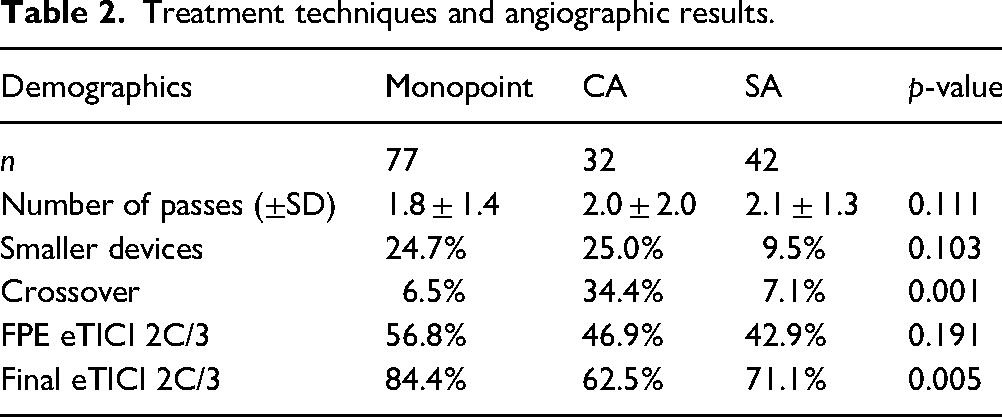
One-hundred fifty-one patients met the inclusion criteria with sufficient data for analysis, as summarized in Table 1. Seventy-seven were identified in the Monopoint group, 32 in CA, and 42 in SA. Technical results are summarized in Table 2. FPE 2c/3 rates were 56.8% in the Monopoint group, 46.9% in CA, and 42.9% in SA (p = 0.191). Final eTICI 2c/3 was achieved in 84.4% of Monopoint cases, compared to 62.5% in CA and 71.1% in SA (p = 0.005). Mean number of passes was 1.8 in the Monopoint group, 2.0 in CA, and 2.1 in SA (p = 0.111). Crossover was less common in the Monopoint group (6.5%) compared to CA (34.4%) or SA (7.1%, p = 0.001). Time to first pass was shortest in the Monopoint group (13.3 ± 7.0 min), compared to the CA group (20.5 ± 9 min) and the SA group (20.4 ± 9.2 min, p < 0.001, Figure 1). Time to final pass was shortest in the Monopoint group (23.8 ± 21.1 min) compared to CA (38.0 ± 32.4 min) and SA (41.8 ± 34.9 min, p < 0.001, Figure 1). There was no significant difference in fluoroscopy time between Monopoint (17.7 min ± 16.5) and CA (17.6 min ± 15.3, p = 0.835), but both had lower fluoroscopy time than SA (26.4 min ± 17.7, p < 0.001, Figure 2). DAP was lowest for Monopoint (18,854 ± 16,113 µGy*m2) compared to CA (31,325 ± 28,912 µGy*m2) and SA (29,483 ± 21,310 µGy*m2, p < 0.001, Figure 2). Radiation dose was lowest in the Monopoint group (884 ± 1039 mGy) compared to CA (1095 ± 1031 mGy) and SA (1994 ± 1583 mGy, p < 0.001, Figure 2). No associations were noted between any of these outcome variables and angiography suite, procedure date, operator, or LVO location (Figures 3 to 5).
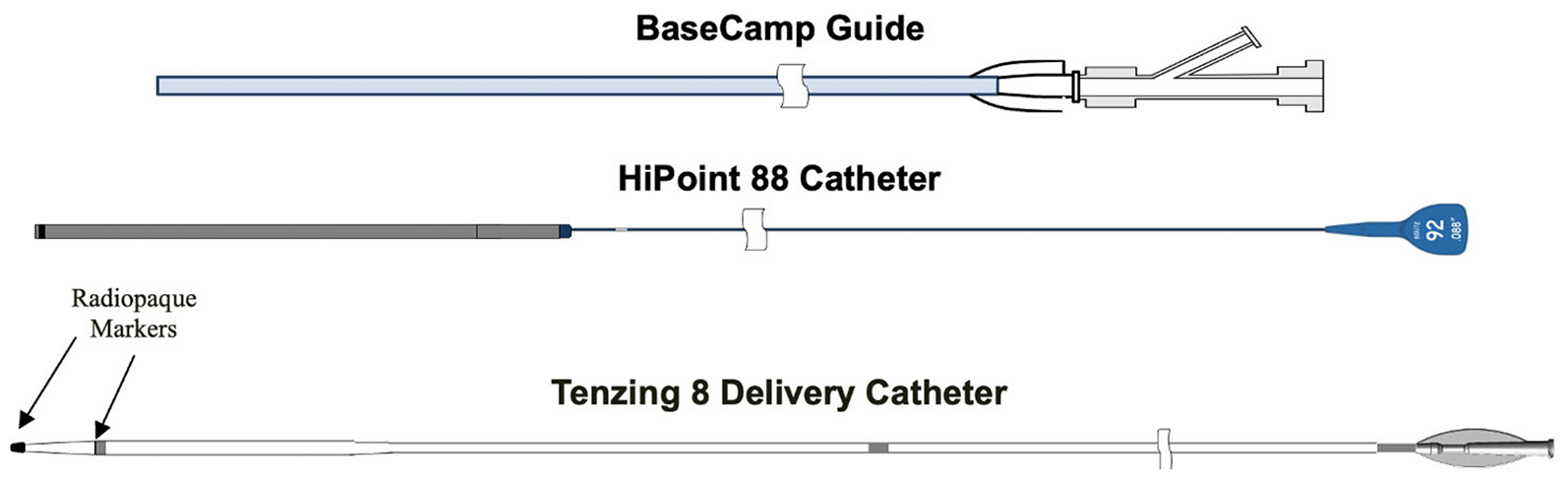
Schematic of the components of the Monopoint system: the Base Camp guide catheter (top), the HiPoint 88 aspiration device (middle), and the Tenzing 8 delivery device (bottom).

Schematic of the Monopoint components assembled for use in endovascular therapy.
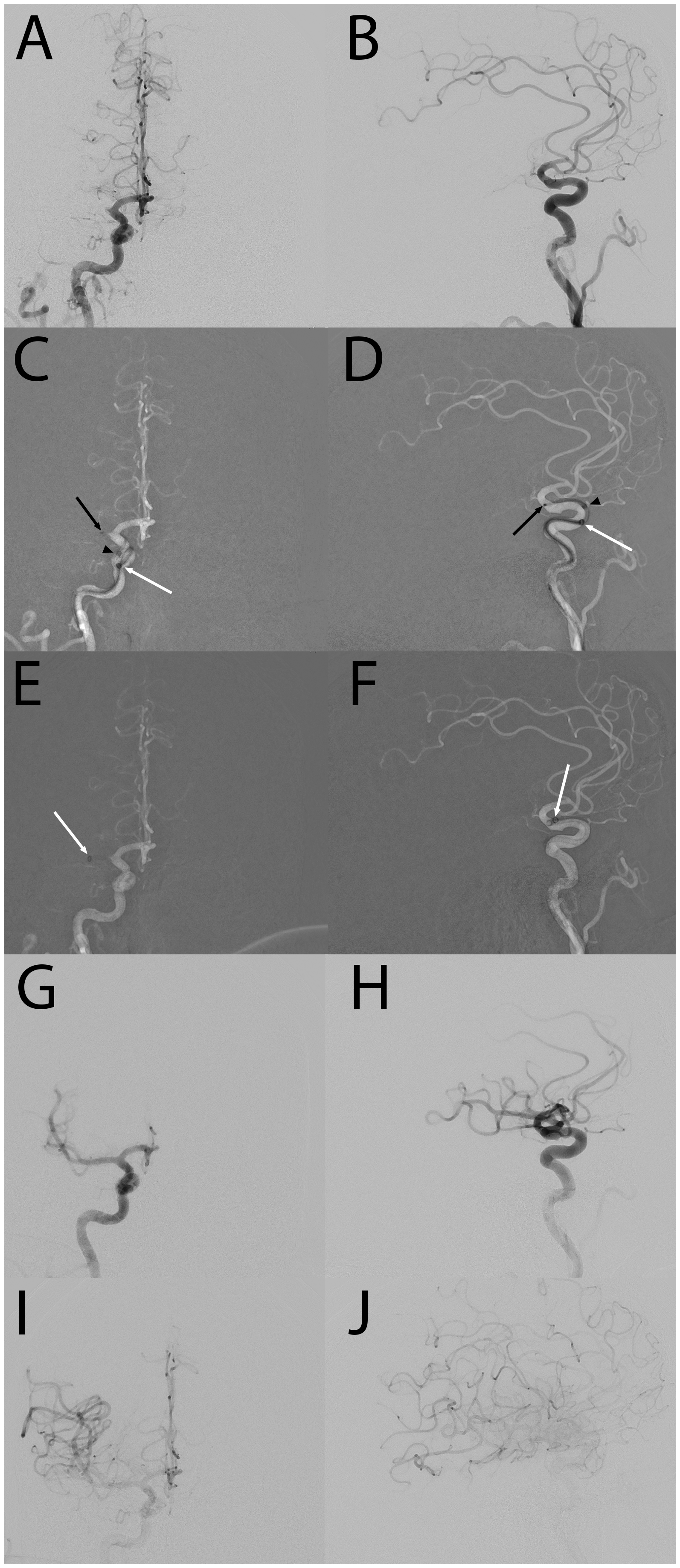
Illustrative case of a man in his 80s with a right M1 occlusion seen on Townes (A) and lateral (B) projections. Roadmap images during aspiration catheter advancement to the clot (C, D) show the Tenzing tip at the clot (black arrow), proximal marker of the Tenzing device (arrowhead), and distal end of the HiPoint aspiration catheter (white arrow). Roadmap images after the Tenzing device was removed (E, F), the distal end of the HiPoint aspiration catheter (white arrow) is seen advancing ingest the clot. Angiography during early (G, H) and late (I, J) arterial phases after thrombectomy demonstrates TICI 3 recanalization.
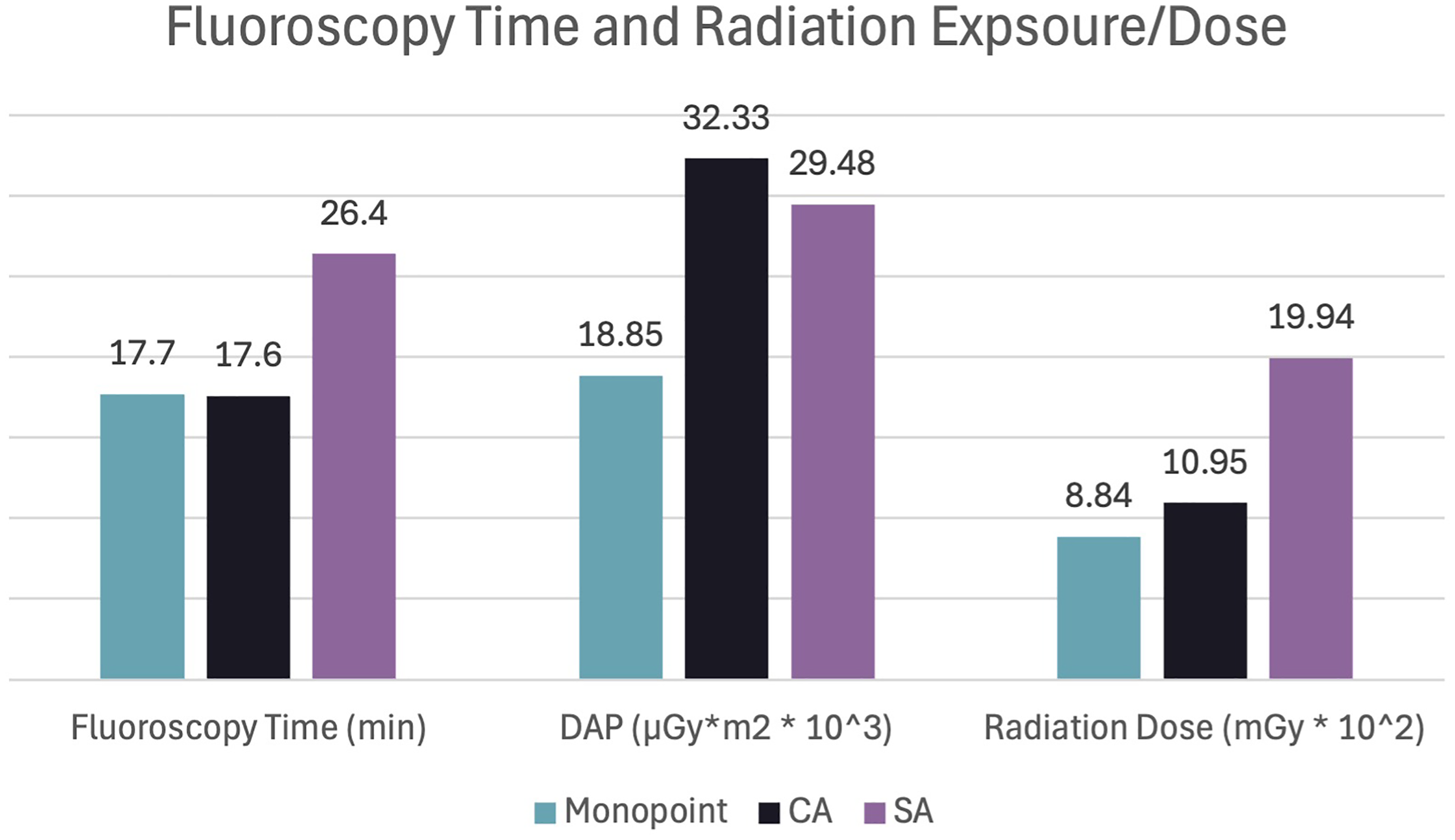
Fluoroscopy time, radiation exposure, and radiation exposure by technique.
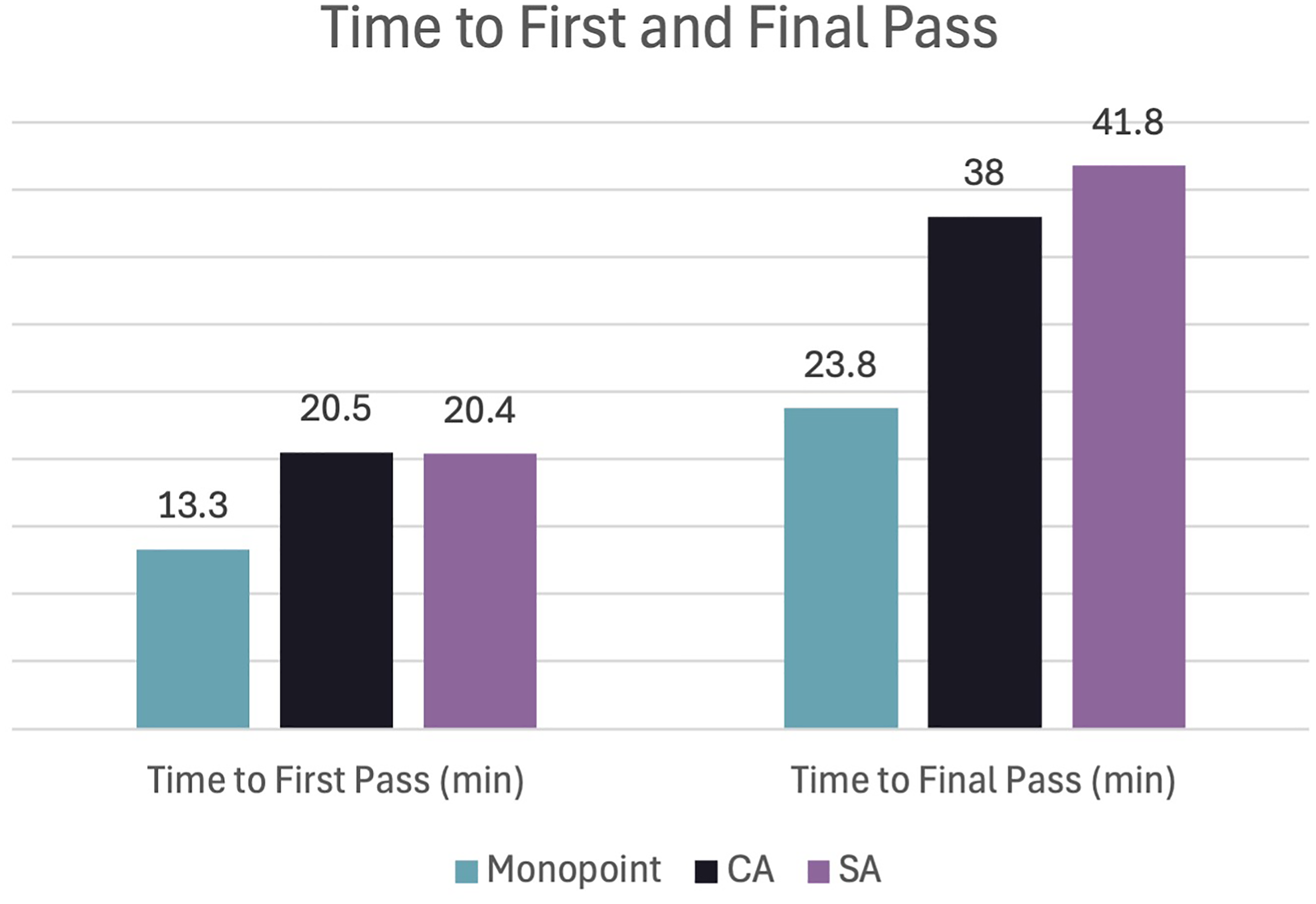
Time to first pass and time to final pass by technique.
Summary statistics of patients and occlusions.
Treatment techniques and angiographic results.
In multivariable analysis, the above-described associations with Monopoint persisted for all outcome variables. Time to first pass was inversely associated with Monopoint (β=−7.86, p < 0.001). Time to recanalization was inversely associated with Monopoint use (β=−12.9, p = 0.002) and technique crossover (β=−19.4, p = 0.002), and it was associated with number of passes (β=13.1, p < 0.001). Fluoroscopy time was associated with the number of MT passes (β=7.22, p < 0.001). DAP was inversely associated with Monopoint cases (β=−15049, p = 0.001) and associated with the number of passes (β=4124, p = 0.017). Similar associations persisted for radiation dose with Monopoint (β=−883.9, p = 0.004) and number of passes (β=440.9, p < 0.001).
Discussion
Neurointerventional procedures involve the use of ionizing radiation. Both stochastic and deterministic effects can be reduced by following the as low as reasonably achievable (ALARA) principle.25,26 Radiation exposure and dose increase with more complex interventions and in procedures with longer fluoroscopy time.18–24 When examining MT procedures specifically, reduced exposure is found with more experienced operators, when fewer MT passes are required, and when treatment is performed for anterior circulation occlusions compared to basilar occlusions.18,20–24 Protocol adjustments can reduce radiation exposure, and MT technique can similarly affect these outcomes, with CA shown to have more favorable exposure results compared to SA.22,23 The current study investigates whether the radiation advantages of CA can be confirmed and improved upon with MT using the Monopoint system compared to CA or SA.
In previous investigations, use of the Monopoint system for MT has been associated with higher rates of FPE, less need for technical crossover, and fewer passes needed to achieve recanalization.10,11,13,17 Technical advantages of the Monopoint system appear to translate into shorter procedure times, with both time to first pass and time to final pass being shorter in the Monopoint group compared to CA and SA. Advantages of Monopoint over CA and SA were also found for radiation exposure, as measured by DAP, and total radiation dose.
Shorter procedures and lower radiation exposure and doses can be found when MT is performed by more experienced operators. 18 This is unlikely to be a confounding factor in the current analysis because all operators at these high-volume centers have far more thrombectomy experience than the thresholds at which these experience-driven benefits are realized. 18 In general, cases in the Monopoint cohort were more recent than those in the CA or SA groups, which could affect fluoroscopic and angiographic algorithms. This could bias radiation findings in favor of the Monopoint technique, although no such association with procedure date and any of the outcome measures in multivariable analyses argues against any such confounding. Alternatively, MT approaches in more recent cases favored more aggressive strategies to achieve final eTICI 2c/3. The higher rates of such recanalization in the Monopoint cohort could be biased by this treatment trend, but such a shift in strategy would also lead to a greater number of passes to recanalize secondary medium and distal occlusions, which would prolong procedure times, fluoroscopy time, and radiation exposure and dose. Again, lack of significant interaction with procedure date in multivariable analyses suggests these treatment trends did not substantially affect results.
Nearly all outcomes had inferior results in the SA cohort compared to Monopoint and CA. Some distinctions between the Monopoint technique and CA warrant examination and could account for the results found between these groups. While fluoroscopy time was comparable between Monopoint and CA, time to first pass was shorter with Monopoint; CA and SA had comparable times to first pass. This may reflect differences in contribution to procedure time while ionizing radiation is not being used. Specifically, this may reflect greater time needed for device preparation with CA and SA compared to Monopoint. Additionally, it could reflect treatment differences in which the Monopoint technique typically involves advancing the Tenzing device only to the angiographic limit of contrast, whereas CA and SA involve crossing the site of occlusion to achieve a more distal position with both a microwire and microcatheter to deliver the aspiration catheter, with or without a stentriever.10,11,13,17 Among interventionalists in this cohort, the self-centering behavior of the Tenzing device allows for safer delivery of devices. Oftentimes roadmap technique is not needed to deliver the aspiration catheter to the clot face, whereas such subtraction techniques were typically used with CA and SA for visualization as devices were advanced beyond the site of occlusion. This lower dose, unsubtracted fluoroscopic technique compared to the subtraction technique likely accounts for the lower radiation exposure with comparable fluoroscopic times.
The current study has several limitations. Its retrospective design is subject to bias, although this is arguably reduced by prospective data collection at each of the sites, as well as analysis of consecutive patients meeting inclusion criteria during the study period. Retrospective classification of the MT technique can also introduce bias, as a prospectively determined technical classification was not considered in the MT decision-making process at the time of treatment during the study period. Some cases during the study period were excluded due to the performance of MT techniques that did not allow categorization into one of the three cohorts. Additionally, patients with atherosclerotic or tandem lesions necessitating more complex or aggressive measures were similarly excluded due to the heterogeneous nature of MT performed in these cases. Finally, this analysis only included MT cases for occlusions of the ICA terminus or M1 segment. Further investigation is warranted for the use of comparable techniques for posterior circulation large vessel occlusions and medium and distal vessel occlusions.
Conclusion
Mechanical thrombectomy for occlusions of the ICA terminus or M1 had shorter procedural times when performed with the Monopoint system compared to CA and SA. Fluoroscopy times were comparable between Monopoint and CA. DAP and radiation dose were lowest in the Monopoint group compared to the two other groups. Further investigation is warranted to assess other clinical and technical factors that affect procedure duration, DAP, and radiation dose.
Footnotes
Ethics statement
All data were deidentified and unlinked to any identifiers. The pseudonymized data of each subject were collated by one author for statistical analysis. The institutional review board of each participating center approved the study and waived the need for patient consent, given the retrospective study design.
Author contributions
Concept and design: FS, MDA, and JK. Analysis and interpretation: MDA and FS. Data collection: all authors. Writing the article: MDA and FS. Critical revision of the article: MDA, FS, and JDE. Final approval of the article: all authors. Statistical analysis: MDA and FS. Overall responsibility: MDA and FS.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FS: Consultant fees, Stryker Neurovascular and Route 92 Medical; Honoraria for lectures, Stryker Neurovascular; Travel, Medtronic; Research Grants: Microvention, Stryker. Stock or Stock Options: Route 92 Medical. JK: None. JDE: Consultant fees, Stryker Neurovascular; Consultant fees, Travel reimbursements, and Stock Options, Route 92 Medical, Co-founder and Chief Medical Officer, Route 92 Medical. WTK: Consultant fees, Stryker Neurovascular; Consultant fees, Travel reimbursements, and Stock Options, Route 92 Medical. RSK: None. BV: None. TAC: None. MDA: Consultant fees, Route 92 Medical. Stock or stock options, Certus Critical Care, Route 92 Medical, Piraeus Medical.