
Abstract
Attendance for regular antenatal care from early in pregnancy is essential for the health and wellbeing of mother and baby. Delayed antenatal care means that any problems may not be identified early enough and hence may become much more serious and have negative health consequences. A regional health service in urban Australia identified that Pasifika women were typically not attending the available antenatal clinics and asked for assistance in using music to address this problem, since music was a culturally appropriate social determinant of health for this population. A collaboratively funded and co-designed consultative approach was developed with both the health service and the cultural community, with additional project advisors and a music therapist/research assistant employed from within the cultural groups. Following ethics approval, three combined focus group/music creation sessions were implemented in order to understand the needs of the women in relation to antenatal care, and to create and record impromptu music for the clinic waiting rooms, consisting of songs and improvisations. Results were recorded and analysed thematically to understand expressed needs, and the recorded music was processed technically for use in the clinic waiting room. After applying a feasibility assessment, this project can serve as an example of a mutually engaged community approach to addressing health needs and as a model for using music in culturally responsive research. This article focuses on the innovative methodology, and broader findings which will be discussed in subsequent publications. This methodological approach is expected to have further applications to other marginalised cultural groups who may be reluctant to engage with delivery and evaluation of health care services.
Keywords
Background
Introduction
In extending the qualitative tool kit of research approaches for addressing community issues, contemporary approaches to improving health and wellbeing have included utilising the creative arts within a wide range of roles and applications, as outlined by Short and MacRitchie (2023). Within the context of public health, arts-based research initiatives have occurred in many ways. Arts-based practices can be integrated into research engagement and data collection to inform and extend knowledge creation (Byrne et al., 2018) and inform health promotion approaches (Siette et al., 2023). Arts based research can also occur through clinical methods crossing visual and auditory senses to enhance rehabilitation and community needs (Short, 2019; Short et al., 2011, 2013) and via an understanding of the community impact of sound in the form of both noise and music (Short et al., 2010; Short, Ní Chróinín, et al., 2026; Williams & Short, 2022). Social work agencies similarly engage with art and music at multiple levels of positive public health interventions (Hall, 2023).
In fact, arts-based health approaches have been applied worldwide within both prevention/promotion and management/treatment contexts, with findings showing that the arts can affect the social determinants of health, encourage health-promoting behaviours and provide supportive acute and chronic care (Fancourt & Finn, 2019). Together with such a report, Clift and colleagues (2021) caution that robust critique is needed to ensure improved understandings of the efficacy of the arts in public health contexts. Further, arts-based approaches may be appropriate for addressing and engaging with marginalised groups, where access to standard services within the traditional health care context is a challenge (Demant et al., 2024). Co-production of arts-based knowledge to create understandings of lived experience can further inform health research and healthcare processes of marginalised communities (Gillibrand et al., 2023). Arts and cultural activities are known to interact with health and wellbeing, extending beyond the person into social and community contexts to contribute further dimensions which may support health and wellbeing (Zbranca et al., 2022).
Our current study results from a specific approach by one large health service in Sydney, Australia, asking for a research project using the arts (specifically music) to understand and facilitate health promotion with one particular large, marginalised group serviced by the health service. This health service had identified that Pasifika women were typically not, or not sufficiently, attending the available community antenatal clinics. Routinely gathered health statistics indicated higher rates of late antenatal first visits by Pasifika compared to Australian-born women (41% vs 29%, SWSLHD, 2019). Anecdotally from staff reflection and observation, multiple barriers appeared to exist, including the appropriateness of the waiting room at the antenatal clinic. Senior health service representatives asked for assistance in using music to understand and address this problem, since music appeared to be a culturally appropriate social adjunct to health for this population and was likely to provide an in-road into connecting with the women. This project occurred within the context of a longstanding relationship between this health service and the leading university researchers, in line with collaboratively-developed arts and health strategic planning which occurred within existing regional and statewide health policy guidelines (ACI, 2024; SWS Health & Arts Partnership, 2024). After initial collaborative discussions, a project brief was mapped out and funding sourced, as outlined in this unfolding article.
Addressing the Public Health Needs of Marginalised People
Groups existing external to dominant Western discourses may be described as marginalised (Roguski & McBride-Henry, 2020). Marginalisation may occur within the health care system and includes associated issues of power and voice for vulnerable groups (Baah et al., 2019). For marginalised groups, sub-concepts of intermediacy, differentiation, power, secrecy, reflectiveness, voice, and liminality impact on health service provision (Fasolino & Koci, 2022). Marginalised groups may struggle with access to appropriate health service resources such as mental health care and social respect (Campbell, 2019) and marginalisation is associated with decreasing health status (Robards et al., 2020). Engaging marginalised groups with public health policy development provides real advantages, where building confidence, capacity and a sense of entitlement may enable further participation in health promotion and engagement in healthy practices (de Freitas & Martin, 2015). Many groups may be considered as marginalised, in turn creating issues of access and equity where delays and disengagement with services may lead to poorer health outcomes (Sheikh et al., 2011). Marginalisation due to culture may frequently overlap with ethnicity and race and is affected by patterns of acculturation (Soman & Koci, 2023). Health promotion efforts have often failed with marginalised groups, and novel approaches are necessary (Roguski & McBride-Henry, 2020).These novel approaches include principles of 1) an overarching self-determination, with freedom to direct the focus and manner of health promotion, 2) processes of collective engagement for building trust and a shared vision, and 3) engaging in collective confidence building activities towards increased awareness of health needs, and all within an approach challenging the conventional role of health promotion practitioners (Roguski & McBride-Henry, 2020). In practical terms, gaining the confidence of members of marginalised groups may mean harnessing meaningful cultural practices and artefacts in order to create a suitable atmosphere for open and engaged discussions and interactions, moving past traditional power-based dynamics and encouraging the emergence of new health promotion approaches.
A current marginalised group is the Pasifika community in Australia, and within this Pasifika women who are pregnant have been identified as being marginalised in one large health district of Sydney. According to Australian Pasifika Educators Network (2023), the term Pasifika refers to peoples and communities who are genealogically, spiritually and culturally connected to the lands, the skies and the seas of the Pacific region (including Aotearoa New Zealand), and who have chosen to settle in and call Australia home, although Enari and Haua (2021) point out that consultations are still needed between the Pasifika peoples and the Australian government to determine appropriate terminology for their population census. Understanding and applying the social determinants of health (WHO, 2024) can give insight into the individual health care context, as it is located within an ecological approach to health (AFMC, 2014). In fact, influences of the social and community context of health care are particularly strong for the marginalised Pasifika community, and therefore new ways of engaging and approaching people, especially women for this project, need to be found within the context of specific health promotion initiatives (Mafile’o et al., 2024; Smith, 2005).
Public Health and Pregnancy Care
Early and ongoing pregnancy care for all women has been the gold standard in Australia since the first public child and family clinics were set up in 1914, thereby supporting the health of both mother and baby through the entire perinatal period (NSW Health, 2015). Australia’s universal healthcare system provides free-of-charge care in public hospitals, including for pregnancy and birth, through funding from the federal and state governments. This ensures access to antenatal care and childbirth services for all women, regardless of their financial situation. It is currently recommended that first-time mothers with an uncomplicated pregnancy have 10 antenatal care visits during pregnancy, with 7 visits for subsequent uncomplicated pregnancies (AIHW, 2024), Midwifery-led continuity of care models, which provide continuous support from a known midwife throughout pregnancy, labour, and birth, have been shown to improve maternal and neonatal outcomes, although access to care is not universally available (Pelak et al., 2023; Medway et al., 2025; Brown et al., 2014). Studies show that negative outcomes for mother and baby, including stillbirth, can result from inadequate attendance for antenatal care (Sánchez et al., 2022).
In Australia, Pasifika women are known to have an increased risk of gestational diabetes (Jones et al., 2024), indicating an even more pressing need for antenatal care during pregnancy. Therefore, it is of critical importance that the women receive early and ongoing antenatal care in every pregnancy. However, as noted earlier, local health statistics indicated higher rates of late antenatal first visits by Pasifika women compared to Australian-born women (41% vs 29%, SWSLHD, 2019), leading to extensive discussions with health managers about contemporary and innovative approaches to assist with engagement in health promotion with this marginalised community. Multiple barriers exist, including the appropriateness of the waiting room at the antenatal clinic. The maternal health promotion approach addresses both environmental and structural determinants of health (Neely & Reed, 2023) and arts-based interventions can be applied to antenatal care to achieve positive effects for social and mental wellbeing as well as supportive experiences during pregnancy (Demecs et al., 2011; Sanfilippo et al., 2021; Sezen & Ünsalver, 2019). Scant materials exist about arts-based interventions in the antenatal hospital clinic setting for hard-to-reach and marginalised minority populations, for health promotion and public health benefits. In this context, Gerace et al. (2023) call for a comprehensive, multifaceted approach that addresses the diverse needs and challenges of Pasifika communities across various domains, particularly in providing culturally responsive social services and targeted place-based interventions.
Music in Culture and Community
The presence of music is ubiquitous across all cultures, fulfilling a wide range of functions including contributions to social organisation, group cohesion, caregiving, meaning-making and communication (Trehub et al., 2015). Professional music therapy uses music to actively support improvements in health, functioning and wellbeing within an evidence-based framework (AMTA, 2026), where typical music therapy approaches promote verbal and musical engagement with community through relevant music activities (Wheeler, 2016). This includes empowered resource-oriented approaches (Rolvsjord, 2015) and community music therapy approaches (Stige et al., 2010). Music and the arts can provide an inroad into many ways of addressing public health issues for health promotion (Bonde, 2019) such as examining the impact of music and noise on lifestyle behaviour for older adults (Short, Ní Chróinín, et al., 2026) and music to reduce anxiety during fertility treatment (Short et al., 2025, 2026). Further, Stige calls for increased understandings of the use of music for public health benefits (Stige, 2018), and Einarsen and colleages (2024) confirm that collaboration between the music therapy and social work disciplines is a good fit. Similarly, a literature review of international research by Lopez de Aguileta and colleagues (2025) showed that music promoted participants’ cohesion, community creation, and transformative actions that align with the values and goals of Social Work, especially around respecting diversity. In terms of cultural diversity, it is well known that Pasifika cultures typically have a strong cultural connection to music, and often strong connections to religious institutions (Mafile’o et al., 2023; Waqa et al., 2023) and hence initial thinking about the use of music for health promotion with Pasifika communities, as in this current project with antenatal care for Pasifika women, is clearly supported by the literature.
In view of this, the current three stage project aimed to: 1. Assemble a team and collaboratively frame the development of an appropriate culturally-based research approach using music to address the identified public health needs 2. Develop a research project, procure funding and prepare for implementation, and 3. Pilot test this innovative research approach for feasibility.
Development of Approach
This project takes a culturally appropriate participatory research approach in line with Consumer and Community Involvement (CCI) and Patient and Public Involvement (PPI) principles (Brammall et al., 2024; Ng et al., 2025). Given that the nature of the research was with Pasifika women, the research was conceptualised and informed by an overall framework known as Fonofale. According to Pulotu-Endemann (2009), Fonofale is a Pasifika cultural model of public health and wellbeing and, as can be seen in Figure 1, uses a Fale (traditional Pasifika house) as an analogy for its multiple dimensions. The fonofale model of health and wellbeing (sourced from Pulotu-Endemann, 2009)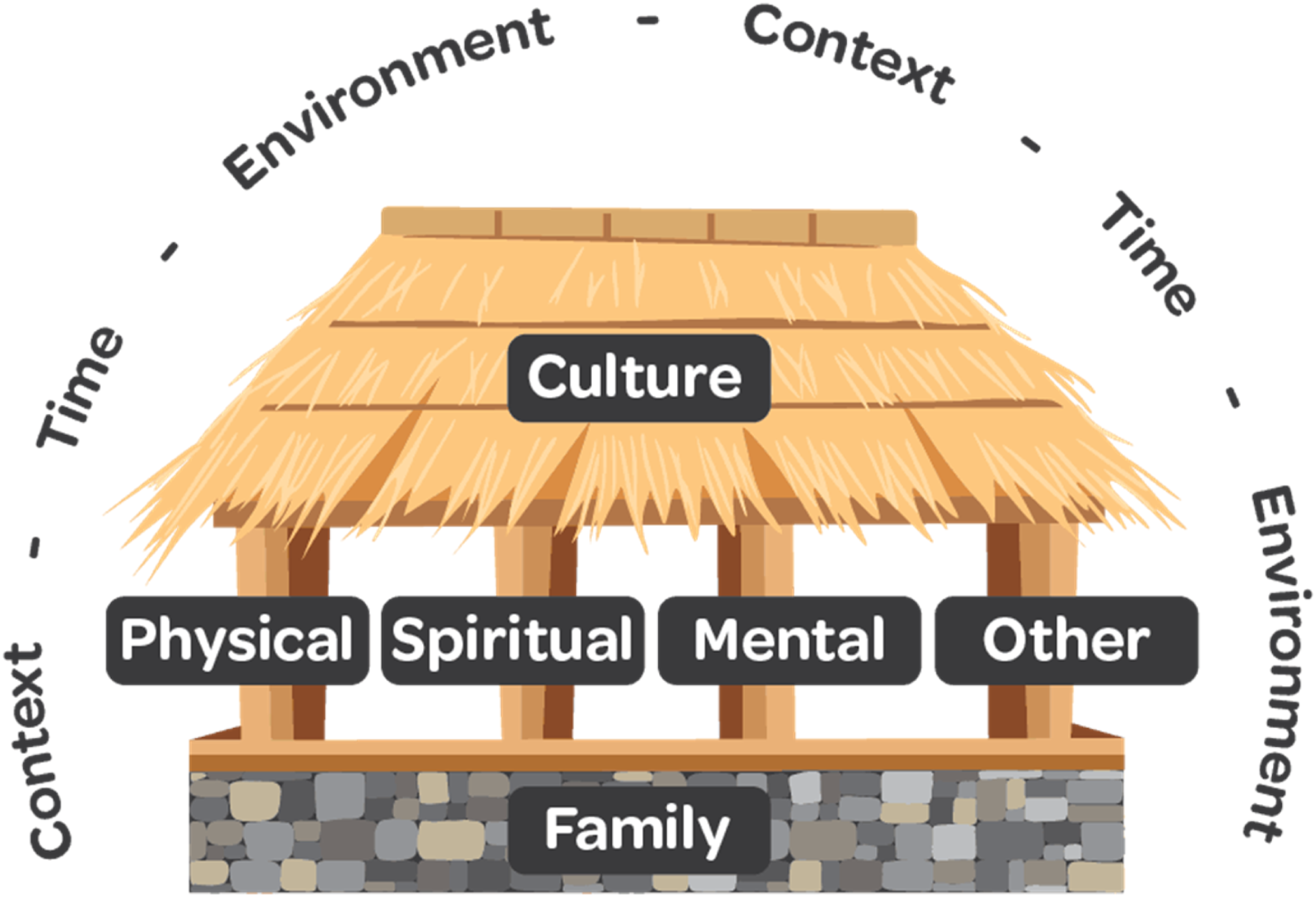
Family – including ancestry – is the foundation (floor) of wellbeing, and cultural values and beliefs provide shelter (roof) for family life. Culture is dynamic and therefore constantly evolving and music, dance and storytelling have a large role in cultural maintenance and healing. Between the roof and the floor are the four pou (posts). These pou not only connect the culture and the family but are also continuous and interactive with each other, where wellbeing is conceived of spiritually, physically, mentally and intersecting with other less easily defined variables. It is also notable that the fale is encapsulated in a cocoon or circle that contains dimensions that have direct or indirect influence on one another, such as the environment, time and context (political, economic, global).
It is significant that this traditional cultural understanding of wellbeing pre-dates the Social Determinants of Health framework and yet shares many similarities outlined in the Alma Ata declaration (1978) and the WHO definition of health as not just the absence of disease. Wilkinson and Marmot (2003) also identify broader contextual aspects such as employment, education, social gradient and the centrality of social support networks as contributing to the health of an individual and a community. Similarly, Macdonald (2005) highlighted the role of environment in developing and sustaining good health and argued that, rather than a deficit-oriented medical model, a strengths-based ‘salutogenic’ approach to health, which is core to Fonofale, is far more effective.
Fonofale encompasses multiple modes and understandings of public health and wellbeing and, in a research context, embraces what is known as talanoa. The talanoa approach is a qualitative, culturally responsive methodology for researching with Pasifika peoples and communities aligning with their communication traditions. It is an in-person gathering (a focus group, or an informal chat between the participant and researcher) where people share their histories, problems, realities, and goals in a safe environment (Mafile’o et al., 2023; Mafile’o et al., 2024; Morrison et al., 2002; Vaioleti, 2006). As relationships serve as the cornerstone of most Pasifika activities, rapport in the research is essential, particularly in an embodied expression of Pasifika values of respect, community, and service (Lakisa et al., 2019; Farrelly and Nabobo‐Baba, 2014). Talanoa’s significance in Australian research highlights the importance of challenging Eurocentric assumptions. Despite its relevance, Pasifika research models and theories are underutilised in Australian music, health and leisure research, making its application here an exciting new development. Music is a core feature of Pasifika culture, and so this innovative participatory methodology was a logical and relational fit for the research, where collaboration and capacity building of participants and same-culture researchers was prioritised and was essential for fostering inclusiveness.
The Chief Investigators brought expertise, experience and leadership from the three disciplines of social work, public health and music therapy. However, as none of the Chief Investigators were from a Pasifika background, it was important to engage in a critically reflexive process. In addition to critically reflexive analysis of data (Chhetry et al., 2024), an acknowledgement of researcher positionality was fundamental. Hall (2023) stresses the importance of assessing motives, detecting biases and correcting ingrained stereotypes through both personal critical reflection and collective checking with members of the pertinent cultural group. To further ensure that the research was engaged and culturally responsive, a collaboratively funded and co-designed consultative approach was developed with both the health service and the cultural community, with additional project advisors and a music therapist/research assistant employed from within the cultural groups. In this project, the non-Pasifika researchers regularly engaged in critically reflexive dialogue with the Pasifika research assistant and the reference group to minimise the influence of a Eurocentric positionality on data collection and analysis. In other studies (such as Stewart-Withers et al., 2017), cultural appropriateness has been exercised in line with the Fonofale/talanoa approach. The current Fonofale/talanoa approach aligns with both participatory action research (Kemmis & McTaggart) and CCI research approaches (Brammall et al., 2024; Ng et al., 2025), seeking to come alongside the community in a mutually satisfactory and respectful manner, in order to assist with identified health issues including public health.
Developing the Project: APHCCRA
This project deliberately used music and music creation with Pasifika communities as a known cultural feature to support increased understanding and engagement of Pasifika women with antenatal care. In developing this project, aims specifically focused on: 1) Using music to collaboratively engage with and increase research understandings of Pasifika community antenatal needs, and 2) Collaboratively producing culturally appropriate music suitable for the hospital antenatal waiting room, inspiring a sense of ownership.
The genesis of the research idea was a question from health staff about how to improve antenatal clinic use by Pasifika women, and whether playing cultural music in the waiting room might facilitate access. Consideration of the cultural and health promotional value of music and related cultural artefacts initiated an innovative music-based methodology. A clear need for the use of music was identified in two different ways. Firstly, culturally specific/relevant music and related cultural behaviours were planned to create social comfort, reduce power differentials and enhance a sense of voice for participants to gather and discuss needs. In line with common cultural practices with this community, this included beginning with a song and prayer, a display of additional cultural artefacts on the research table (flower garlands, shells, conch shell), and the provision of food at the end of the talanoa focus group. Secondly, within the sessions, the provision of musical instruments and group writing materials (a blackboard) assisted with creating music (songs and instrumental) that were suitable for use in the waiting room. Integrating both of these elements into a single integrated entity of a talanoa focus group/music session, this became known as the Arts in Public Health Collaborative Cultural Research Approach (APHCCRA). In order to implement this project, a research assistant (RA) with both music therapy training and experience to support engagement with everyday community members and with personal knowledge and connection to the Pasifika community was required, alongside research leadership from the broader research team to guide and review questions and processes. Implementation of APHCCRA talanoa focus group/music creation sessions by the RA was supported by the non-Pasifika Chief Investigator (CI) who assisted with guiding the RA, plus set-up, notetaking, food delivery and general project management of the sessions.
Challenges were experienced around research ethics approvals due to understanding the community collaborative approach, in light of cultural sensitivities and the power relationships inherent in accessing clinic care. Research ethics approval was received from the SWSLHD HREC [Ref: 2023/STE02393] and Western Sydney University HREC [Ref: RH15783]. All participants gave written informed consent, where it was made clear that both discussions and music making would take place, which would be recorded and the music used for research and public health purposes.
Multiple research team and planning meetings took place in order to create a culturally appropriate context for research data collection, inspired by principles of CCI/PPI and other known research examples (Rose et al., 2023). Considerations included appropriate cultural locations for data collection and the provision of suitable food (lunch) in light of both cultural and healthy eating for pregnancy factors.
Six combined talanoa focus group plus music making sessions (each 90 minutes long) were planned with these six group sessions addressing different groups within the Pasifika diaspora: Samoan, Māori, Fijian, Cook Islanders, Tongan and a Mixed group. The desired data focused on participants’ understanding and experience of antenatal care and health clinics, and their cultural connection to music. Due to recruitment challenges only three of the planned six talanoa groups went ahead. Data collection was planned to include both written forms and recordings within the talanoa focus group/music creation session; and as the project unfolded a further on-campus recording studio session occurred. All data was collated and entered, and audio materials were transcribed and analysed thematically; music files were reviewed and subjected to sound engineering processing. ( Figures 2 and 3) Cultural artefacts, musical instruments and recording resources Music creation within the project

Pilot Testing and Feasibility of APHCCRA
The implementation of APHCCRA is now reviewed in line with the pilot testing and feasibility approach of Lawson, where a consideration of process, resources, management, and scientific/pilot implementation aspects of a study are all seen as contributing to broad feasibility understandings (Lawson et al., 2022). As a public health focused approach to feasibility, the authors agreed that Lawson’s work was appropriate as a framework for analysis in this study.
Pilot Implementation
Participants were recruited via circulated flyers, word-of-mouth and from existing social groups. As noted, a total of three (not six) talanoa focus group/music creation sessions were run across two weeks, with a total of nine attendees from Samoan, Cook Islander, and Maori cultural backgrounds, and these participants also stated that they had insights into many other Pasifika cultures. Participants were from 25-34 and 35-44 age groups and were in first, second and third trimesters of their pregnancy. Only one participant was a primipara (first pregnancy) and she had been attending antenatal clinics, and all but one participant said that they had been feeling very well during their current pregnancy. The groups met in community-based locations (rather than health services) and questions were posed about what would make it more likely for pregnant Pasifika women to attend antenatal clinics, and whether original Pasifika music played in waiting rooms might be a facilitator of access. Recorded group data were transcribed, with associated thematic analysis (Braun & Clarke, 2021) applied. Common themes were identified in the data through an initial layer of coding followed by critically reflexive dialogue between the researchers to agree on broader themes. For the purposes of this article, thoughts on the methodology have been included but other findings on outcomes are intended for a separate article. In line with ethical practice, no names were mentioned in any recordings or transcripts due to using badges with numbers instead of names. Musical recordings were reviewed and processed, and the university staff sound engineer suggested a further recording in studio, to control and enhance sound quality, which was then undertaken.
Challenges occurred with recruitment and getting the groups together. For example, finding a critical mass of pregnant women who were available to gather in one place, fitting with school times, work commitments and antenatal visits was difficult. For this low socio-economic group, asking them to take time off work potentially affected their financial situation, plus if it were a second pregnancy they likely also had childcare responsibilities.
Although recruitment numbers were small, engagement of participants in discussion and music making was enthusiastic within the talanoa focus group/music creation sessions, and participants were encouraged to speak about not only their own experiences during pregnancy but also those of other women known to them within their community, thereby representing further distilled knowledge about community needs. Speaking in first person and using terms such as cousin, sister, my neighbour, someone I know, the participants provided input without referring to any specific names.
Reflecting on the value of this project for the women in her community, one participant said: “That’s why I loved the initiative to have nice, soothing music be played while you’re in the waiting area. Because without people actually knowing, music has frequencies that, you know, it gets you on different energy levels. And so for me, I’m like, without music, I can’t give birth. I can’t be without it. I rely on it. Yeah, so it would be great to have that set ambience in the waiting room. Get the mother relaxed before she goes into her antenatal appointment… Sometimes you’ll get the midwife that will just skim through it and just get you out.”
Participants were not afraid to speak out for their communities about the inadequacies of the current health system, demonstrating a sense of their own power to represent their community and express the voice/s of these marginalised women, with another participant saying: “And you, and you, you can feel that it’s just like, you’re just another mother. And so if they [staff] could be trained in more of the, the way of making every single appointment, and I know it’s hard, but making every single appointment more personalized. Um, and just for, and also like letting the mothers know, like, that it’s
Limitations of this study included small group and participant numbers within this qualitative research approach. Additional constraints linked to this were the timing of implementation of the project towards the end of the university year which then ran close to extended pre-Christmas activities. Ethics approvals also excluded additional Pasifika community members who expressed interest in attending (for example, those who had recently given birth or were elders/leaders in the community). The original plan for the research was for data to be collected – and music created -with currently pregnant women. As the research progressed and the possibility of speaking with women who had recently given birth emerged, there was insufficient time to receive ethics approval for amendment before the completion of the project. Such an exclusion was a limiting factor and ran contrary to the Fonofale and talanoa principles underpinning this project, and in future the inclusion criteria need to be broadened to all community members who feel invested in this issue, as an outworking of collaborative inclusive practice. Ideally, to be consistent with this culturally responsive method, there could have been an additional step in collaborating around the data analysis, especially consulting on the themes generated through the process. Limited time and the deadline for funding expenditure provided a barrier for engaging in this way, and will be considered for future projects.
Feasibility
The feasibility of this study is reviewed in line with Lawson’s four broad areas for consideration: Process, Resources, Management and Scientific (Lawson et al., 2022) which has been applied to music and health projects (for example, Short & Palaniappan, 2026). Whilst the scientific area of feasibility has already been addressed in discussions of the pilot study (above), process, resources and management are now further explored.
Process
The broad research team that was gathered to guide this project was involved at all levels of the project planning, leading to a culturally appropriate study addressing contemporary issues in public health related to promoting antenatal care in the marginalised group of Pasifika women. Music was successfully woven into the talanoa focus group context for culturally responsiveness engagement in group discussions. Music was also utilised for forming an engaged outcome of recorded music files, which could in turn be used for health promotion within a public health focus by playing this music in the antenatal clinic waiting room. Creation of this music was self-directed by the participants attending the talanoa focus groups within an empowered process, with facilitating suggestions and support from the RA and CI (who were both trained Music Therapists bound by professional code of ethical conduct). Final decision-making rested with the women themselves. In line with ethics approvals, everyone was informed directly about what was happening in this project and a post-participation token payment occurred with gift cards. Most wanted to be involved to help their community. There was currently no recorded music being used in waiting rooms, and participants suggested that they could start a trend – and that there could be music from other cultural groups. Shared ownership resided in the recording and the agreed use of their music to help others.
Observation of non-verbal body language suggested that participants were relaxed in the context of the group, and that they engaged enthusiastically in the song creation/music making in each of the sessions. Participants were observed to be comfortable and sufficiently skilled with playing guitar, singing, playing other instruments and the even creating sounds from a conch shell. Given the stated purpose of the music creation part of the project, participating women spontaneously searched for common or similar words across Pasifika cultures – using their personal knowledge and internet searching via their phones – such as use of the words “pepi” (baby) and “moe” (sleep), as an emergent lullaby was developed and created for recording. The Cambridge English Dictionary (2025) defines as a lullaby as “a vocal piece of music specifically designed to lull a child to sleep by using a repeated formula”. The participants chose this form of music as it is used culturally during pregnancy and infancy for calming purposes The soothing nature of lullabies, encompassing low pitch, slower tempos and reduced energy, has been demonstrated to provide self-regulation of arousal levels for mothers and may assist with maternal depression and anxiety (Cirelli et al., 2020).
Although the initial plan was for six talanoa focus group/music creation sessions, in fact three sessions were run, all with mixed Pasifika cultural groups. This occurred mostly due to specific Pacific Islander community recruitment challenges, which occurred in terms of time, location and availability of participants and research assistant. Some participants were willing to attend an additional on-campus recording studio session to re-record some of the music, showing their commitment of time to this project and its value for their community.
Resources
This project has access to excellent advice and guidance as a resource, from conceptualisation thought implementation to results and interpretation of this entire project. The RA was clearly briefed on the purposes and aims of the current project, and the way that this could be integrated. She was a trained and registered music therapist and therefore used to engaging purposefully with people through music; was from a Pasifika culture and therefore had connections and shared cultural understandings. Links to relevant religious facilities where the Pasifika community typically gathered was also invaluable for booking of suitable spaces to implement the project, and an appropriately sized room supported talanoa focus group, musical instruments, recording and post-study refreshments (lunch). In one instance, a final music recording happened after lunch and prior to the participants leaving. This integration of activities and functions led to a conducive data collection context, in line with the Fonofale and talanoa principles of this project relating to the strength of cultural practices such as sharing food, music and stories.
Relevant musical instruments were easily available as resources for this project, based on CI linkage to the music therapy department within the university, and likewise dedicated state-of-the-art recording studios and expert sound engineer services were available as needed through the music department of the university, for successful implementation of this project. Having funding available for lunch (sandwiches, fruit, water) was invaluable as a culturally appropriate activity and a health support for the pregnant women, forming an informal “thankyou” for their attendance. The availability of gift cards as a further token of appreciation for attendance within the research project was also of financial help and recognised the socio-economic needs of this marginalised community.
Management
Project management unfolded under the guidance of the CI and the entire research team. All ethics requirements were met in a timely manner as was data collection, although some delays were experienced over data processing and analysis which related to individual circumstances and availability.
Preparations for embedding the music into the clinic waiting room setting are still in process and will require additional technical help, and consideration of resources for implementation into the clinical situation. On reflection, the project could have benefitted from additional time for distribution and recruitment, and consideration of further locations where pregnant Pasifika women may gather would be helpful in future studies. In terms of planning for this project, separating out the language groups was not shown to be an effective strategy, because in the end people were likely to have multiple connections across different groups.This multiplicity became evident as participants demonstrated their knowledge of different Pasifika languages when they collaboratively searched for words with similarities in developing a lullaby song. Using already established social groups, whether they were same or mixed language groups was what eventually enabled recruitment for this project.
Discussion
This project created an innovative methodology combining qualitative and arts-based music approaches to address a contemporary public health and health promotion challenge with marginalised Pasifika women, in order to understand and work towards increased engagement with antenatal care to improve the health of both mother and baby. Framed within a CCI/PPI and a culturally sensitive fonofale/talanoa approach, this project used participation in music-making to collaboratively engage with and increase research understandings of Pasifika community antenatal needs. Consistent with the research methodology, the project collaboratively produced culturally appropriate music suitable for the hospital antenatal waiting room, inspiring a sense of ownership within the public health clinic context.
Implementation of the collaboratively developed APHCCRA project demonstrated feasibility in piloting this approach, and the combination of both talanoa focus group and music creation outcomes within a single session was effective in producing results relevant to the intent and questions addressed in this regional public health and health promotion initiative. Not only did the participating women speak freely and openly, and excellent data was collected about the needs of the Pasifika community in relation to barriers and enablers for antenatal clinic attendance, but it was also clear that participants valued the opportunity to create music together which could be used to assist others within the community to feel more comfortable in the antenatal clinic waiting room. Some participants suggested that music from many other marginalised groups beyond Pasifika cultures could also be included, addressing the needs of even more women within this culturally diverse region.
Challenges existed around the sound quality of music creation with a regular group setting where the talanoa focus group and music creation were combined. Further consideration may need to be given to a planned rather that emergent use of the on-campus recording studio for future projects, and perhaps can be planned into a further protocol as a two-stage process. Likewise, the inclusion of additional community representatives such as women who have recently given birth or other community representatives may contribute to deeper and more well-rounded community understandings. Nevertheless, this project demonstrated that such a combined qualitative arts-based approach is in fact possible, since the participants did engage with this research process and music was created. The fact that both the RA and CI were music therapists and trained to engage well using music with general community members was of value to this project. At the same time the CI and Co-investigator had extensive additional experience as health services researchers. This project assisted a marginalised community derive a sense of ownership within the health system and its processes and informs health managers within the regional health system. It serves as an example of a mutually engaged community approach as a methodology for exploring and addressing health needs, and is expected to have further applications to other marginalised cultural groups who may be reluctant to engage with health care services.
Conclusions
We created and implemented the new APHCCRA methodology in order to research and address a particular public health need in contemporary society, where marginalised communities must be engaged in order to enhance access and equity to health care, with this in turn benefitting future generations and enhancing wellness and wellbeing in the community public health context. This feasibility pilot project may also apply in future iterations of projects addressing Pasifika community health needs beyond antenatal care, and projects addressing other hard-to-reach communities such as Aboriginal and Torres Strait Islander and humanitarian entrant groups, where music can act as a positive facilitator of public health promotion for engagement in health and wellbeing activities.
Footnotes
Acknowledgements
Thanks to the participating women for their enthusiasm and insights. Project team: Dr Alison Short, Dr Neil Hall, Prof Josephine Chow, Jacqueline Ramirez, David Kelly, Kathryn Farrell, Sydney-Rella Pihema (RA). Advisory group: A/Prof Freya MacMillan, Prof Virginia Schmied, A/Professor Litea Meo-Sewabu. Technical advisor: Mitchell Hart.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Western Sydney Creative Collaborate Fund ($13,800 AUD).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.