
Abstract
Background
Participating in research is widely accepted to have benefits for participants, but there is less evidence about the impact on researchers, clinical staff and organisations involved in the research delivery.
Aim
To explore how participation in a randomised controlled clinical trial impacts on researcher development, professional development of clinical staff, organisational capacity and delivery of clinical services.
Design
Longitudinal qualitative study using interviews undertaken at three timepoints across the period of a clinical trial.
Participants and Setting
Three groups of participants involved in a clinical trial being undertaken at nine centres across India will be invited to participate. This includes: 1) Research staff involved in the design and delivery of the clinical trial; 2) Clinical staff involved in delivering the clinical aspects of the trial; 3) Organisational representatives from the hospital senior management teams at each site.
Materials and Methods
Ethical approval has been granted by University of Leeds Dental Research Ethics Committee and Bharath Institute of Higher Education and Research. Interviews will be undertaken virtually using communication platforms that are commonly used across India (Microsoft Teams and Zoom). Training and technical support will be offered to anyone who is not familiar with the platforms. Participants will be asked for consent for the interviews to be audio-recorded and auto-transcribed. Experienced qualitative researchers will facilitate interviews using a topic guide. Data will be collected at three time points: at the start of the clinical trial, 18 months and 3 years after recruitment commences. Analysis will follow an inductive reflexive thematic approach.
Background
Individuals’ experience of being involved in clinical research has been explored from the perspective of research participants (Lawton et al., 2003; Locock & Smith, 2011) but there is limited research about the experiences of those involved in the delivery of research. Research impact is often described in terms of knowledge production, capacity building, health benefit, informed decision-making and broad socio-economic benefits (Banzi et al., 2011); however, this does not capture the potential benefits to researchers, clinical staff and the organisations involved in delivering the research. Wider benefits may be related to professional and personal development of personnel involved directly or indirectly in delivering the research, organisational and service benefits, capacity building and subsequent improvements to patient care. Nurses involved in research reported to gain experience and knowledge of the whole research process, as well as wider skills such as writing and literature searching skills, team negotiation skills, patience, tolerance, and adaptability (Higgins et al., 2010). There may also be intangible benefits, which are outcomes or effects that are not explicitly measurable and are not solely attributed to the process or project.
Understanding the potential benefits of research allows these benefits to be optimised and measured to further justify the use of finite research resources. Potential domains for professional and personal development for researchers are described in the Researcher Development Framework (Vitae, 2011) and include knowledge and intellectual capabilities, personal effectiveness, research governance and organisation, engagement, influence and impact. While interventions to develop and record researcher skills or behaviours have been described, such as educational activities, outreach visits, audit and feedback (Mazmanian et al., 2013) and research journals (Borg, 2001), few trials have examined how researchers developed through their participation in clinical research.
For the clinical team, participation in research may contribute to professional development by providing new or updated clinical knowledge and skills to improve the quality and safety of practice. Potential areas for individuals’ development in addition to improved clinical knowledge and skills include ongoing competency, improved personal skills, greater job satisfaction, the ability and confidence to drive change and innovation, and better understanding of evidence-based care. Organisational benefits may include a positive learning culture, new ways of working, innovation, enhanced recruitment and retention of staff, greater skill mix, productivity and performance; together these benefits can enhance service development and delivery, and improve patient experience and outcomes.
It is also recognised that research can be challenging due to limited resources, a lack of knowledge and support, and historically, a culture where those contributing to research delivery may have little input into the question and design and inadequate recognition for their contribution (Darbyshire, 2008). Structured discussions with Clinical Nurse Consultants and Nurse Unit Managers using the nominal group technique aimed to identify challenges and benefits to nurses engaging in research (Higgins et al., 2010). A key barrier was that nursing culture prioritises practice and providing patient care is perceived to be core work, whereas research is secondary, resulting limited resources being allocated to delivery of research. Furthermore, there was a need to meet short term goals and benefits from engaging in research were often delayed, or even unrealised where research findings did not lead to change in practice. Research language, a lack of support and resources, and the lengthy research process were also identified as challenges.
This qualitative study will explore the experience of research and clinical staff participating in research, to understand the motivators, benefits and challenges. This will be achieved through interviews with researchers and clinical staff involved in a multicentre randomised controlled trial being undertaken in India. The clinical trial aims to evaluate the effectiveness of naso-alveolar moulding in children with a non-syndromic unilateral complete cleft lip and palate. Cleft lip and palate is one of the most common congenital malformations, with an overall incidence of around 1 in 700 newborns (Vanderas, 1987) and it is accompanied by a wide variety of dental and skeletal anomalies. These can have a major long-term impact on the child’s facial aesthetics, function and self-esteem. Cleft care is marred by controversies over the multiplicity of treatment protocols (Mossey & Little, 2009). Naso-alveolar moulding is a non-surgical orthopaedic treatment that aims to facilitate surgery by improving the position of premaxilla, reducing the size of cleft, and reshaping and resizing the nostrils prior to lip surgery. It has shown to be effective for children with unilateral or bilateral cleft and it is usually performed between 1-5 months of age.
Medical and dental research infrastructure and training in India is continuously developing with a focus on addressing healthcare challenges, improving the quality of care and outcomes and providing better patient experience. In the present trial, the clinical teams have been given bespoke training on all clinical areas including naso-alveolar moulding, surgery and speech assessment prior to the commencement of the trial, and ongoing support throughout the trial. Consequently, this trial offers an excellent opportunity to explore how clinical staff and services develop throughout the research period.
Study Justification
This study aims to understand the experience of researchers and clinicians participating in research using a qualitative approach. This is expected to yield insights into the motivation and expectations for participating in research, the benefits and challenges of delivering clinical research and how research delivery can be supported. The findings of this study will be useful to a number of stakeholders such as funders and individuals and organisations involved in developing and delivering research, for example: • Understanding individuals’ motivations and expectations to inform engaging, training and supporting potential researchers • Understanding practical issues facing different groups at different time points and solutions to overcome these issues. • Identifying potential training and support needs for clinicians delivering new interventions or outcome measures • Understanding how to recognise an individual’s contribution to research in a meaningful way. • Identifying methods to capture the potential wider benefits of research to allow greater evaluation of research and justify funding.
Aims and Objectives
This study aims to explore researcher and clinicians’ experience of participating in a multicentre randomised controlled trial to understand the opportunities and challenges presented by research.
The objectives are to explore: 1. Participant beliefs, expectations and knowledge of research prior to commencement of the trial; 2. Opportunities and challenges experienced during the delivery of the trial; 3. Researcher and clinical staff perception of their development over the research period; 4. The perceived impact of trial delivery on organisational capacity and service delivery within the coordinating institute and collaborating centres.
Study Design and Research Team
This will be longitudinal qualitative study undertaken at key timepoints across the period of the clinical trial, expected to be approximately five years. The research paradigm is interpretative, based on an underpinning ontological belief that reality is subjective and constructed by the participant through their experience of it, and an epistemological assumption that researchers will interpret the data through their own lens (Burns et al., 2002). This approach meets the objectives of understanding individual’s experiences of participating in a trial and understanding these experiences to inform future research development, delivery and evaluation. The use of sequential interviews to explore participants’ experiences and beliefs will support a focus on understanding lived experiences across the trial period.
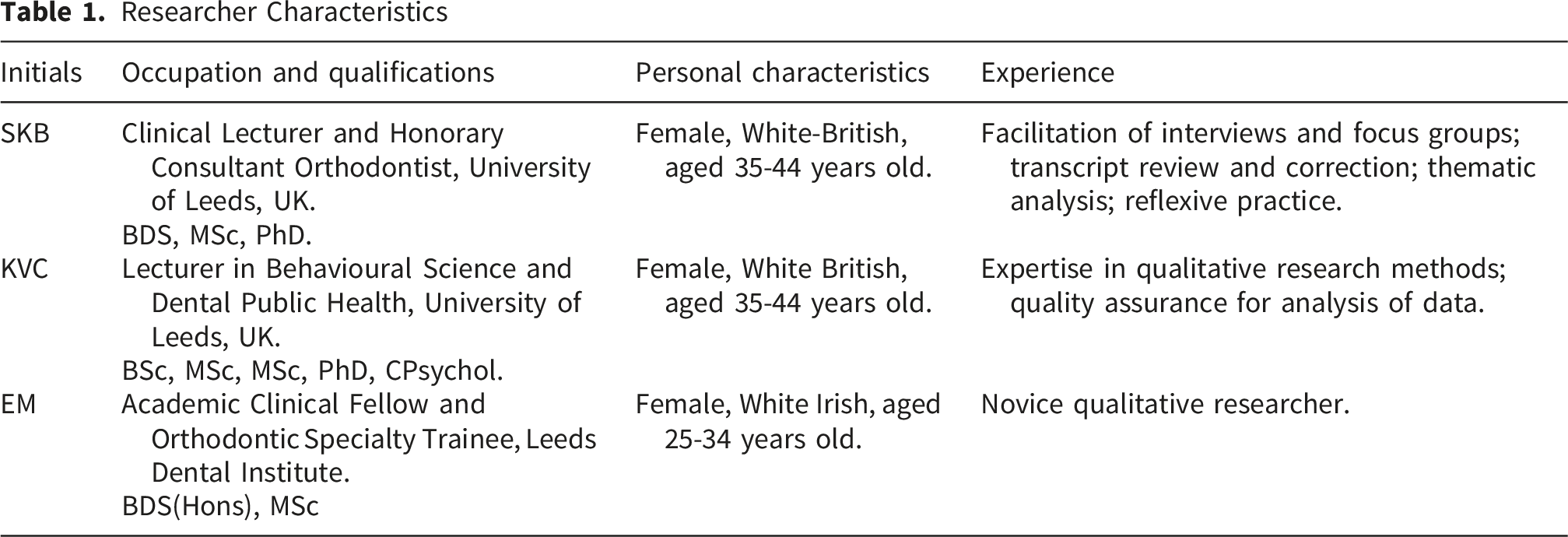
Researcher Characteristics
Setting and Participants
Three groups of people involved in the clinical trial who will be invited to participate in this qualitative study: (1) Research staff who are involved in the design and delivery of the trial including the lead investigators responsible for development of proposal and trial design, site co-ordinators responsible for day-to day delivery and management of trial, staff involved in training and calibration and PhD students who will collect and analyse the data; (2) Clinical staff from the collaborating centres involved in delivering the clinical aspects of the trial includes those providing the naso-alveolar moulding and cleft surgery and the wider clinical care team; (3) Organisational representative from the senior management team who is able to provide information about organisational capacity and service delivery.
The trial involves nine cleft palate centres across India so participants will be recruited from across these sites. All sites have established cleft services, including provision of both surgical and dental treatments for all ages. Use of the intervention (naso-alveolar moulding) currently varies across the cleft services in these nine sites, which will allow examination of the experience of clinicians who are both experienced and new to delivering the intervention. All clinical teams have been given bespoke training on the clinical procedures, including naso-alveolar moulding, cleft surgery and speech assessment, prior to the commencement of the trial to ensure standardisation. All clinical teams will have ongoing support throughout the trial.
Similarly, experience of delivering research varies across the staff participating in the trial. To ensure rigour and quality in the research, training was provided for researchers on key methodological concepts and teams participated in calibration exercises to help standardise methodological processes, for example, data recording. Consequently, the trial offers an excellent opportunity to explore how researchers of all levels develop throughout the research period.
Sampling and Recruitment
Participant Groups and Expected Numbers of Potential Participants
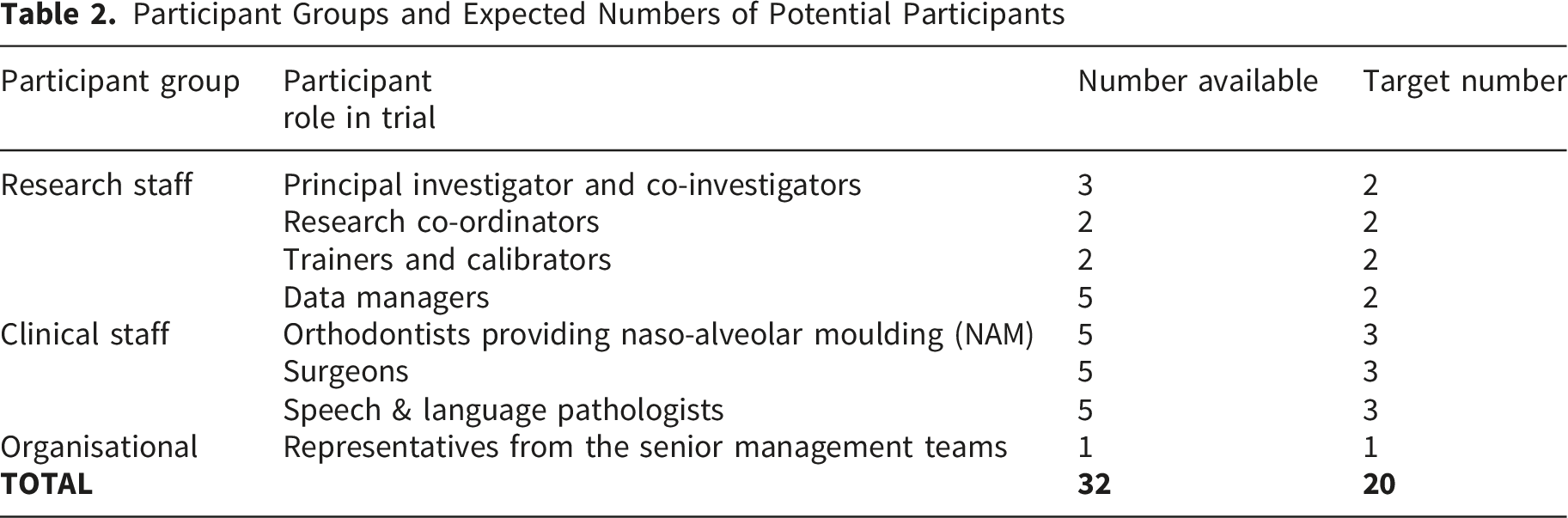
The particular specifics of this study were considered when determining target sample size (Braun & Clarke, 2019a). The research question is relatively focussed, limited identity-based diversity is expected, data collection methods will allow for in-depth exploration of experience and generation of rich data, the sample population is limited, and the analysis aims to answer a relatively specific question. For this reason, a provisional sample size of 20 was agreed with a range of 15-25.
A list of all staff involved in the trial in the coordinating centre and across all collaborating sites is held by the trial coordinator (SC). Potential participants will be sent an invitation email by SC that outlines the study and includes a participant information sheet. Those invited to take part will be reassured that their role in the trial will not be affected if they do not wish to take part in the qualitative study. While it is preferable that participants take part across the full study period, it is recognised that this may not be feasible so participants will be re-invited at each time point. Those who are interested in taking part will be asked to contact Principal Investigator (SKB) directly. Any questions will be answered and then a date will be agreed for data collection. Written consent will be obtained prior to data collection. A log will be kept of participant recruitment including number invited, enrolled and completed, and any reasons for refusal or withdrawal.
Data Collection
Interviews will be undertaken using virtual communication platforms that are commonly used across India (Microsoft Teams and Zoom). Training and technical support will be offered to anyone who is not familiar with these platforms. Participants will be encouraged to keep their camera on where possible to aid interaction. Participants will be asked for consent for the virtual interviews to be audio-recorded and auto-transcribed by the communication platform. The length of the interview will be recorded along with any additonal notes on technical issues.
One or both experienced qualitative researchers (SKB and KVC) will facilitate the interviews. No-one else will be present. The interviews will be conducted in English and although all participants have a high level of English language, steps will be taken to ensure language does not interfere with data collection. Firstly, participants will be sent guidance for the interview and a copy of the topic guide in advance to allow any questions about process to be answered and provide an opportunity for the participants to think about the questions and what they wish to say. Secondly, the facilitator will summarise their understanding of the answers that were given to each question to make sure everything has been understood correctly. In addition, participants will be offered the opportunity to review their transcripts if clarification is needed around meaning or language. Audio-recordings will be reviewed after each session specifcially to allow facilitator debrief and any revisions to the topic guide as needed.
Timepoints
Data will be collected at three time points across the trial period (Figure 1): T0: Prior to the commencement of the clinical trial (prior to start of recruitment) T1: Approximately 18 months after the trial commences T2: Approximately 3 years after recruitment commences Timeline for research

T0 will focus on participants’ beliefs, expectations and knowledge of research while T1-T2 will explore the opportunities and challenges experienced during the delivery of the trial and how researcher and clinical staff development over the research period. Organisational representatives from the collaborating centres will be included to explore the perceived impact of trial delivery on organisational capacity and service delivery.
Materials
Supporting materials for the qualitative study were developed by the principal investigator (SKB) and reviewed by the trial coordinator (SC) to check clarity and acceptability. Materials include: ⁃ Recruitment materials: Invitation email, participant information sheet, consent form ⁃ Data collection materials: Guidance for interview, topic guides
The subjects for discussion in the preliminary topic guides were informed by the Researcher Development Framework (Vitae, 2011) for research staff and the Generic Professional Capabilities Framework (General Medical Council, 2017) for clinical staff. The topic guides for researchers and clinicians for the first interviews are included in the supplemental material. To align with the planned inductive thematic analysis approach, audio-recordings and transcripts will be reviewed prior to the subsequent interview to allow any interesting discussion points arising from the participants to be incorporated into future topic guides.
Data Processing
Audio-recordings will be transcribed using the autotranscription function on each platform. The transcripts will be reviewed with the audio-recording by the researcher to allow correction and check accuracy. Transcripts will be returned to the particpants to be verified. This additional step will be offered to check the accuracy of language.
Each participant will be assigned a unique identifier that will be used on all documentation and to label audio-recordings and transcripts. Only the Principal Investigator (SKB) will be able to link the unique identifier to personal details.
Participants will be made aware in the intitial invitation email that responding to the prinicpal investigator will mean their name and email address is being transferred to the United Kingdom. Personal information (name and contact details) will be logged in a Microsoft Excel spreadsheet and stored securely. Details will not be shared and will only be stored for the duration of the study. A data sharing agreement between the University of Leeds and BIHER has been established.
Analysis
Analysis will follow an inductive reflexive thematic approach (Braun & Clarke, 2019b), where codes are topics are identified from the data then discussed, refined and interpeted. Intial coding and topic development will be performed by two qualtiative researchers (SKB and EM) independently and in duplicate using nVivo. Refinement of topics and agreement on the final thematic framework will be achieved through discussion with a third analyst (KVC). Anaylsis will be performed in the following steps: 1. Familiaristation with transcripts (SB and EM independently) 2. Coding to describe the meaning of dialogue with devleopment of initial codes (SB and EM independently) 3. Discussion of interpretation of data and refinement of intital codes (SKB and EM together) 4. Development of topics by grouping codes (SKB and EM independently) 5. Discussion of interpretation and refinement of topics (SKB, EM and KVC) 6. Development of themes (SKB and EM together) 7. Discussion of interpretation and refinement of themes (SKB, EM and KVC) 8. Mapping thematic relationships (SKB, EM and KVC) 9. Selection of anonymised illustrative quotes to explain themes (SKB and EM)
Decisions about revisions to the coding and themes will be recorded for transparency and to evidence reasoning for decisions. Throughout data analysis the researchers will reflect on the assumptions underpinning their reading and interpretation of the data. Details of the study’s environment, participants, and procedures will be recorded to enhance the potential for transferability (Ahmed, 2024).
Promoting Quality
Methods to promote researcher reflexivity will be embedded throughout the research. Field notes will be taken during interviews to record any background information, environmental factors, interactions and behaviours that are considered important contextual information for analysis and interpretation (Phillippi & Lauderdale, 2018). Research memos will be used during data collection and analysis to record the researchers’ feelings, ideas and reflection, to record decisions and reasoning, to examine meaning, assumptions and interpretation, and to aid communication between the research team (Birks et al., 2008).
Engaging over an extended period with the participants and practicing self-reflection throughout aims to increase the credibility of the findings (Ahmed, 2024). Data source triangulation (Carter et al., 2014) will be utilised by reviewing information shared by participants and the trial PI, such as personal development plans, researcher training records, hospital activity logs and any evidence of change to clinical practice.
Supplemental Material
Supplemental Material - Exploring the Wider Effects of Participating in a Clinical Trial for Clinical and Research Staff: A Protocol for a Qualitative Study
Supplemental Material for Exploring the Wider Effects of Participating in a Clinical Trial for Clinical and Research Staff: A Protocol for a Qualitative Study by Sophy Barber, Badri Thiruvenkatachari, Jonathan Sandler, Subhiksha Chakkaravarthi, Emily McIlvannaa and Karen Vinall-Collier in International Journal of Qualitative Methods.
Supplemental Material
Supplemental Material - Exploring the Wider Effects of Participating in a Clinical Trial for Clinical and Research Staff: A Protocol for a Qualitative Study
Supplemental Material for Exploring the Wider Effects of Participating in a Clinical Trial for Clinical and Research Staff: A Protocol for a Qualitative Study by Sophy Barber, Badri Thiruvenkatachari, Jonathan Sandler, Subhiksha Chakkaravarthi, Emily McIlvannaa and Karen Vinall-Collier in International Journal of Qualitative Methods.
Footnotes
Ethical Considerations
Ethical approval for the main clinical trial was granted by Sree Balaji Dental and Medical Colleges and Hospitals, Bharath University (BIHER), Chennai (SBDCH/IEC/2023). This is renewed annually and the qualitative study was included in the 2023 application. At the same time, specific approval for this qualitative study was granted by the University of Leeds Dental Research Ethics Committee (DREC ref: 020323/SKB/367) on 14th April 2023. The study will be conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and those consistent with Good Clinical Practice (GCP).
Consent to Participate
Informed consent will be obtained from all participants.
Author Contributions
All authors contributed to the study design. The main text was written by SKB and KVC and it was then reviewed and revised by all authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the DBT/Wellcome Trust India Alliance Fellowship [grant number IA/CPHS/20/1/505255] awarded to Badri Thiruvenkatachari
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors do not have any conflicts of interest to declare.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.