
Abstract
Longitudinal personal network studies make unique contributions to understanding how social contexts evolve. These studies have primarily been conducted in structured environments, such as hospitals, schools, workplaces, or large urban populations, where participants are easily reached, and standardized tools can be applied. These conditions differ from those in rural communities, where services are scarce, commuting is a part of daily life, and survey literacy is low. This paper reports on a three-wave personal network panel in a rural Eastern European community, with two additional waves planned. We conducted recruitment through link-tracing, in which participants introduced others from their networks while building on existing ties, which supported trust and continuity. Instruments were adapted in collaboration with community members to ensure cultural fit and minimize burden. Data collection involved repeated face-to-face interviews and locally organized events. Fixed and free-choice name generators, as well as visual elicitation tools, helped respondents to represent their networks across waves. Retention was supported by adapting fieldwork to community rhythms and maintaining researcher presence. The study produced methodological contributions to link-tracing recruitment, participatory adaptation of instruments, interactive elicitation design, and context-adapted retention strategies. These adaptations reduced respondent burden, improved data quality, and sustained participation across waves. Limitations include inherent biases in link-tracing and the intensive resources required for long-term involvement. Even so, the study shows how panel personal network research can be conducted in underserved rural contexts. Beyond its empirical setting, the study advances methodological insight into strengthening the design and sustainability of panel personal network research, which remains underdeveloped in many applied fields. It offers a framework for informing qualitative and mixed-methods research in health and social fields.
Keywords
Introduction
Longitudinal personal network studies have been applied to a wide range of topics, including aging, migration, social support, and life-course transitions (Bidart & Charbonneau, 2011; Cornwell et al., 2014; Fischer & Offer, 2020; Lubbers et al., 2010). These designs enable observation of how social structures evolve and shape outcomes such as health and well-being (Chapman et al., 2022; O’Malley & Christakis, 2011; Shelton et al., 2019). Despite their potential, most longitudinal network studies rely on standardized survey traditions and fixed name generators, typically used in urban or institutional contexts (Jeroense et al., 2025; Perry et al., 2018; van Tilburg, 1998). Such approaches face persistent challenges, from sustaining retention across waves to adapting instruments to diverse cultural settings (Bidart et al., 2018; Cornwell et al., 2021).
Generally, a longitudinal personal network study can be illustrated as follows. A researcher meets with the same study participants at multiple time points (waves), typically months or years apart. At each meeting, respondents are asked to name the people who are important in their lives and to describe those relationships in terms of closeness, frequency of contact, and shared behaviors. Respondents are also invited to indicate whether the people they named know each other (this captures connections among alters, known as alter-alter ties). By comparing these networks across waves, the researcher can observe how ties form and dissolve over time, how the network’s internal structure changes, and how network characteristics are associated with outcomes such as health or behavior change.
In health research, longitudinal personal networks have been employed to examine how social structures impact risk behaviors and health outcomes (Darabos et al., 2025; Hunter et al., 2019; Min et al., 2013; Rice & Halbert, 2017). This work demonstrates the value of repeated measures and also reveals the scarcity of studies conducted in rural communities. Rural contexts pose additional barriers. Limited institutional infrastructures make registry-based sampling difficult. Seasonal migration or commuting for work complicates participation and retention. Low survey literacy and local skepticism toward outside researchers require participatory engagement to build rapport and trust (Hammersley & Atkinson, 2019).
We draw on two theoretical traditions. The first is participatory research. This redefines the role of community members from passive data sources to active co-producers of knowledge (Cornwall & Jewkes, 1995; Israel et al., 1998). In this tradition, validity is related not only to measurement precision but also to relational trust, community acceptance of the research as culturally appropriate, and shared ownership of the research process (Cargo & Mercer, 2008; Jagosh et al., 2012). Applied to longitudinal network studies, this means that the quality and completeness of network data depend not only on the instrument design but also on the quality of the relationship between researchers and the community over time. The second tradition is adaptive methodology. This can be understood as the reflexive modification of research procedures in response to contextual conditions without compromising analytical integrity (Maxwell, 2013). In rural and underserved settings, adaptive approaches are a necessity: the absence of formal registries, low survey literacy, and seasonal mobility mean that no fixed design can be maintained throughout extended fieldwork without significant data loss.
This study was conducted within the framework of a larger European research project, which investigates the role of social structures in shaping cancer-related health behaviors (4P-CAN, 2023; Feliu et al., 2026). While the project provides the substantive backdrop, this paper focuses on the methodological aspects. We present the design and implementation of a multi-wave personal network study in a rural community, adapted through participatory approaches.
Our contribution lies in adapting link-tracing recruitment (Hâncean et al., 2021; Molina et al., 2022), participatory co-creation of data collection tools supported by interactive software, and community-based retention strategies to a rural panel context, as developed in the sections that follow.
Three interconnected research questions underpin our contribution. First, how can longitudinal personal network research be adapted to the methodological constraints of rural, resource-limited settings where standard survey infrastructures are absent or inadequate? Second, which participatory strategies most effectively support recruitment, instrument design, and retention across multiple waves in these settings? Third, what transferable principles emerge from this experience to guide future longitudinal and mixed-methods personal network research in comparable contexts?
This paper is structured as follows. We situate our design within the literature on longitudinal personal network research, describe the rural study setting and methods, and outline the methodological lessons learned. We then reflect on the opportunities and limitations of this approach. In this way, we substantiate transferable lessons for qualitative and mixed-methods researchers working in underserved rural settings.
Our Design in Context
Selected Longitudinal Personal Network Studies and Methodological Contributions

Our study extends this literature (Table 1) in several ways. First, most prior work has focused on urban or institutional populations; we conducted a three-wave panel in a rural community, with two additional waves planned. Our rural setting offers a novel testbed for methodological adaptation. Second, we combined methodological tools from the literature, such as fixed- and free-choice name generators (Maya Jariego, 2018; McCarty et al., 2007), with participatory network elicitation supported by interactive software (Birkett et al., 2021). Consequently, we gave our respondents the tools to build larger, more diverse networks. Third, we conducted face-to-face interviews, which allowed for immediate validation and participant feedback. Fourth, while most previous studies recruited participants from surveys or registries, we employed link-tracing recruitment to build trust and enhance retention. Finally, building on previous studies in the field (Cargo & Mercer, 2008; Jagosh et al., 2012; McCarty et al., 2007; Stadel & Stulp, 2022), we collaborated with community members to adapt the instruments, ensuring cultural fit and reducing cognitive burden. How our study was carried out, and the Discussion that follows are organized around the same five areas: recruitment, data collection tools, elicitation, retention, and fieldwork timing.
Study Setting
The study took place in a Romanian rural commune with a population of 4,330 (3,808 aged 18+). The settlement lies in a mountainous area, while its economy is mainly agricultural, with households relying on small farms and seasonal work. Although the region hosts industrial sites, the community reflects a rural periphery. Employment opportunities are limited: some residents are retired or depend on municipal social assistance, whereas those in the labor force are either employed in a small number of local positions or commute to nearby towns or abroad for work.
This community has served both substantive and methodological aims under the larger European project that has sought to enhance primary cancer prevention across Central and Eastern Europe through citizen participation and digitally enabled social innovation. The community is relevant to the social determinants of cancer risk and serves as a challenging test case for longitudinal personal network research in a rural setting. Health care access mirrors national constraints in rural areas. Primary care is available through family doctors and pharmacies, but residents often travel long distances to various towns or cities for specialized services. The country faces persistent inequalities in access to health care between rural and urban populations. Rural areas are marked by shortages of primary care providers and under-resourced facilities (Vlădescu et al., 2016; World Bank Group, 2018; World Health Organization, 2022). These constraints contribute to poorer health outcomes and reinforce skepticism toward external interventions. Recent analyses show that rural residents face significant barriers to accessing timely and continuous care.
Furthermore, adverse working conditions undermine the recruitment and retention of primary care professionals (Brînduşe et al., 2024; Ciotlăuş et al., 2025). Cancer prevention remains particularly underdeveloped: the country records some of the lowest screening participation rates in Europe, with breast cancer screening reaching only around 9% of women in the target age group, compared to an EU average above 60% (Eurostat, 2023; OECD & European Commission, 2025). This context makes rural communities a critical setting for testing methodological adaptations in longitudinal and participatory health research.
Methodologically, this community is a challenging case. Seasonal migration, commuting for work, agricultural calendars, limited digital literacy, and unfamiliarity with formal surveys intensify standard panel challenges (compliance, recall error, attrition, and cultural fit). These conditions necessitate adaptive, participatory strategies to build trust and ensure validity. As a close-knit, small-sized community with constrained health infrastructure and everyday mobility, this locality functioned as a living lab, i.e., a real-life ecosystem in which methods were co-adapted with participants (Malmberg et al., 2017).
Research Design
Preparation of the Fieldwork and Community Entry
We collected personal network data in three waves: September 12–23, 2023 (Wave 1), March 21–April 1, 2024 (Wave 2), and March 20–April 5, 2025 (Wave 3). We adapted the research calendar to local agricultural rhythms. September followed the harvest, while April preceded intensive farming and seasonal migration. A preparatory phase (May–September 2023) preceded Wave 1.
The fieldwork was performed by an interdisciplinary team (five men and four women) from sociology, medicine, and public health. One aim was to establish rapport, adapt the design, and create conditions for longitudinal work. At this stage, the team attended village events (e.g., the annual fair and the local soccer matches) and meetings with local authorities. Additionally, they conducted repeated informal interactions with residents, health professionals, teachers, the media, and other local stakeholders.
Community immersion was employed to foster trust and gain an understanding of local life. Team members stayed in the village, utilized local services, adhered to daily routines, and engaged in community life. Prolonged engagement and persistent observation (Guba & Lincoln, 1989) helped surface norms and shared understandings of health risk and illness. Observing practices in situ supported situated knowledge of how relationships and culture shape risk behaviors (Haraway, 1988). The classic standardized surveys alone cannot capture these realities.
Co-creation was pivotal. The residents were addressed as partners rather than passive respondents, consistent with participatory research traditions. While maintaining the overall research objectives and methodological design, we adapted tools and procedures to incorporate local feedback, enhance data quality, and preserve comparability across waves. Immersion helped identify gatekeepers and influential actors. Their involvement supported rapport-building, facilitated panel recruitment, strengthened retention across waves, and enhanced the study’s legitimacy. The local authorities brokered the first entry and helped us gain legitimacy to stay in the community. At the same time, the local health workers, who were not residents, declined to engage with our research initiative, claiming a lack of time and resources.
The immersion phase had a methodological function. We informally piloted options with local actors and gathered feedback on digital tools. Discussions addressed touchscreen elicitation versus paper forms and flagged barriers (digital literacy, privacy). We therefore selected Network Canvas (Birkett et al., 2021), an open-source, offline, participant-centered platform. Versions 6.0.0 (Wave 1) and 6.5.3 (Waves 2-3) enabled respondents and interviewers to construct and review collected network data in real-time.
Immersion supported a structured community entry (Schensul et al., 1999). We engaged the community as a partner, incorporating local input into instrument choices and guiding cultural fit. To support this process, we convened a citizens’ jury of nine volunteers (three men and six women) that served as an advisory body. The jury proposed topics for community events, offered feedback on ongoing activities, and advised us on ways of integrating into village life. Although recruited voluntarily, the group comprised active and retired individuals from diverse income levels and educational backgrounds. This heterogeneous profile ensured a diverse mix of perspectives, although it did not fully represent the community as a whole. Engagement with the jury unfolded through individual conversations during data collection and informal group meetings. Members made methodological contributions both on their own initiative and when asked.
In sum, future studies of this kind should actively seek support from the community. In our case, such support came from the mayor’s office and from residents who voluntarily joined the dissemination events we organized locally.
Implementation of the Data Collection Process
We employed personal (or egocentric) network analysis following the seminal work in the field (McCarty, 2002; McCarty et al., 2019). We built on the best practice in the literature (Hâncean et al., 2024; Kim et al., 2015; McCarty et al., 2007; Tracy et al., 2012) and measured personal networks by including a focal respondent (ego), named connections (alters), and the relationships among alters. Alters were elicited using name generators (Campbell & Lee, 1991), while name interpreters measured attributes and the relationships’ features (e.g., closeness, contact frequency, support, and shared behaviors).
Figure 1 presents our panel personal network design. Questionnaires in all waves included (a) socio-demographics (e.g., age, sex, education, occupation, household size); (b) health and lifestyle (e.g., self-rated health, chronic conditions, smoking, alcohol intake, physical activity, diet); (c) cancer-related perceptions and behaviors (e.g., knowledge, attitudes, screening/prevention, information sources); and (d) personal network modules using fixed (W1) and free-choice name generators (W2-3) to elicit alters, their attributes, ego-alter and alter-alter ties, and perceived influence on health behaviors. Details are available in the Supplemental Material (SM) (Hâncean, McCarty et al., 2025). Measuring personal networks at multiple points in time. Note. Personal networks of two study participants (p1 and p7) at three data collection points within a longitudinal mixed-methods design. Nodes represent alters named by the focal participant (ego), with edges denoting ego–alter or alter–alter ties. Color coding captures churn: black denotes alters and ties elicited in the current wave; gray marks alters not yet elicited; orange indicates dissolved (or not elicited) alters or ties; blue reflects restored alters or ties that were previously elicited, then absent, and later re-elicited. Community-level events are organized before and between data collection waves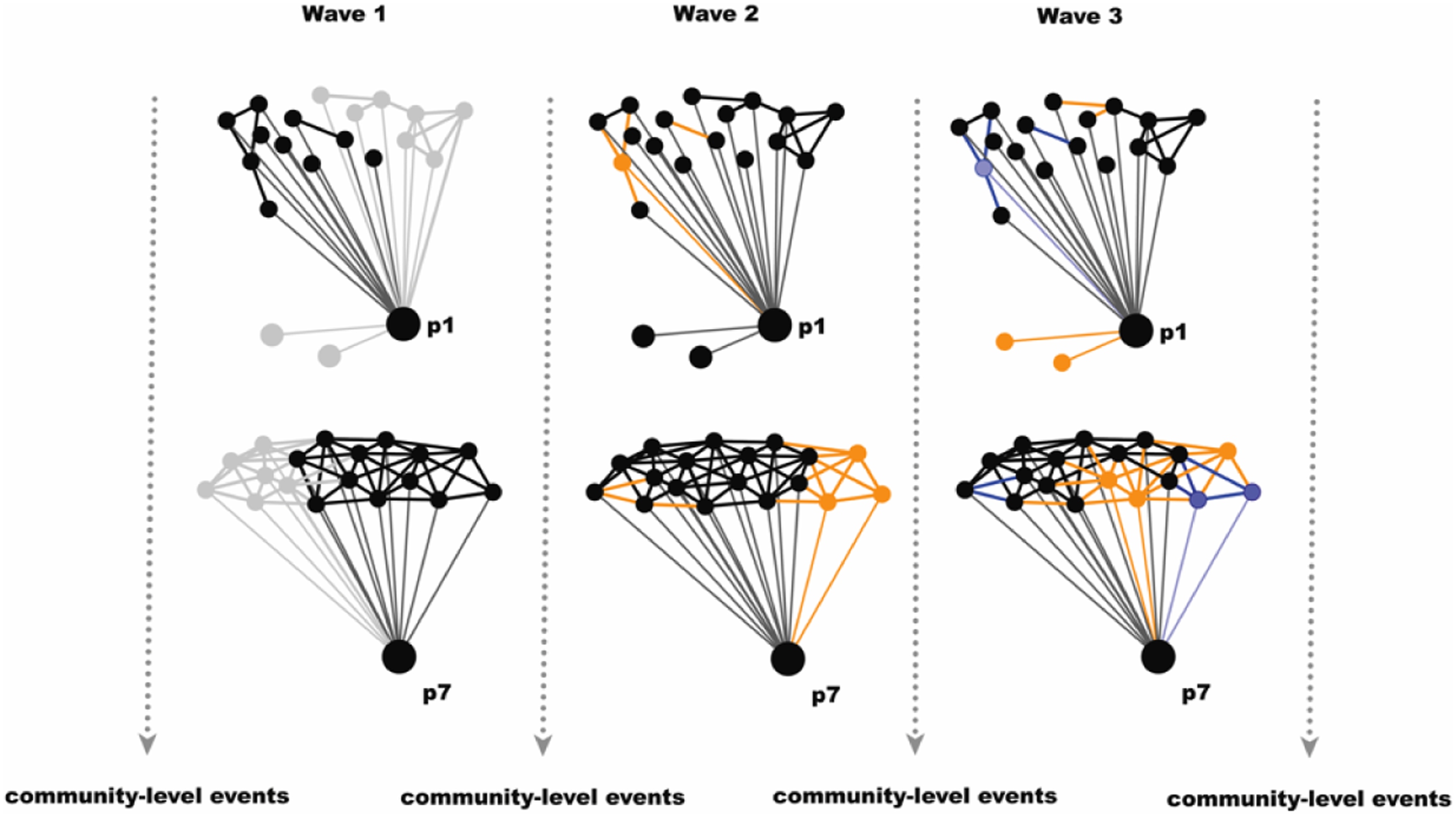
We tracked alters using full names and key socio-demographics to improve identification across waves. Study respondents assisted us in tracking alters across waves. All interviews were conducted face-to-face in neutral, accessible venues (e.g., local lodges, village halls, central community spaces) arranged for comfort and privacy. Real-time visualization in the Network Canvas software supported data quality control and participant feedback during interviews.
We organized community-level events before and between data collection waves. These events addressed cancer social risk factors (Espina et al., 2025) and were open to the entire community, not only to the study participants or the citizens’ jury. Participation was voluntary and free of charge. The events varied in format, content, and audience. Topics proposed by participants and the citizens’ jury included alcohol consumption, nutrition, physical activity, and tobacco use. Activities took the form of an art gallery, workshops, lectures, and seminars for adults and school pupils. Annual health festivals (July 2024 and June 2025) promoted physical activity across all age groups. For example, a walking football competition involved participants aged 6 to 82. Local media reported on the events as part of a broader strategy to promote healthy lifestyles. Healthcare professionals and members of the research team also participated in these events. Beyond their educational function, the events helped maintain visibility, consolidated trust and rapport, supported retention, and generated contextual data on behaviors and participation. We documented event attendance to track how many egos and alters were reached.
We did not provide financial incentives for participation. Instead, we emphasized reciprocity, co-creation, and engagement, offering ethically appropriate forms of non-monetary value, such as free blood tests (at the health festivals) and preventive medical advice, including a hotline for medical second opinions. Given the limited access to medical infrastructure, participants regarded these non-monetary incentives as appropriate and beneficial. However, it is possible that such incentives may have particularly appealed to individuals who were already more health-conscious, potentially limiting participation among those less engaged with preventive health behaviors.
Multi-Layered Data Structure
Our longitudinal design allows for the analysis of network dynamics and the behavioral clustering previously detected by others (Hâncean, Lerner et al., 2025; Mihăilă et al., 2024; Oană et al., 2024). Repeated observation is essential for distinguishing between social selection (homophily) and influence (contagion), and for accounting for contextual confounding. The panel also facilitates opportunities for validation, as some individuals appear as alters across multiple egos or as both alters and egos, allowing cross-checks of reported behaviors and tie characteristics (Figure 2). Multi-layered network data structure integrating link-tracing and personal networks. Note. This figure illustrates the multi-layered structure of the network data, capturing both link-tracing recruitment patterns and embedded personal networks. Black arrows represent the link-tracing network, indicating who nominated whom and who was recruited by whom in the study. Labelled black nodes represent interviewed study participants (egos), while labelled grey nodes represent individuals who were recruited but not interviewed. Each ego’s network is displayed in black, with small black nodes and ties denoting alters and their interconnections. Grey edges indicate ego-alter relationships. This organization reflects a hierarchical structure in which alters are embedded within egos, and egos are embedded within the larger link-tracing network. Orange dashed contours highlight co-dependencies across personal networks. Namely, alters who are simultaneously elicited by more than one ego, or who are themselves study participants.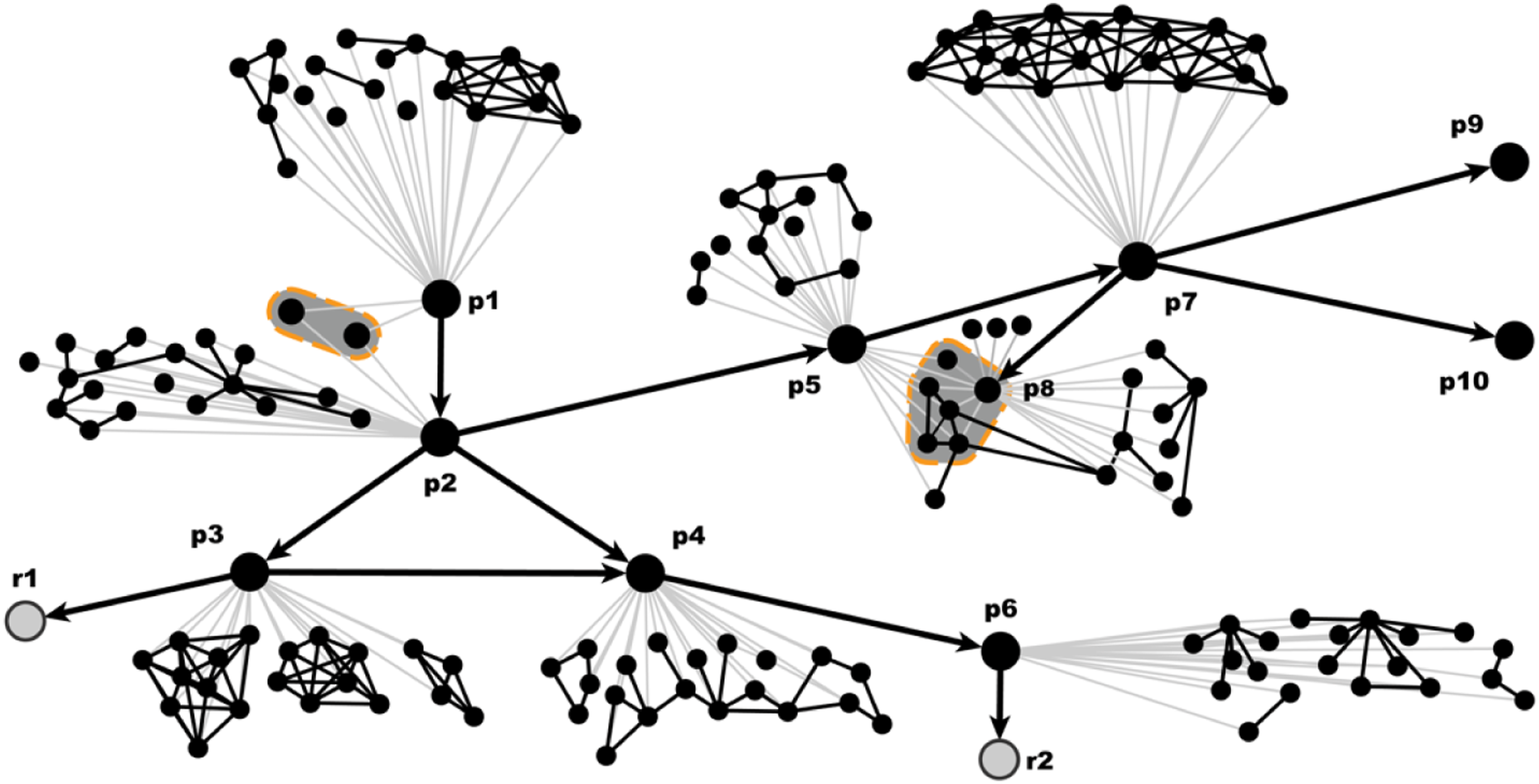
The resulting data display cross-dependencies and a multilevel structure, motivating the use of cross-classified multilevel models and related approaches. The data are amenable to relational hyperevent models available in network science (Lerner et al., 2025; Lerner & Lomi, 2023), as we also recorded participation of egos and alters in community-level events (event data). Additionally, tracking alters across waves allows for comparisons of name-generator designs and of alter retention/change, similar to those implemented by others (Hâncean et al., 2026).
Sampling and Recruitment
As illustrated in Figure 2, we employed a link-tracing sampling approach. After each interview, participants could nominate and recruit new participants who met clear eligibility criteria (18 years or older, at least 6 months’ residence in the rural community, ability to speak and understand the local language, informed consent, and voluntary participation). We contacted nominees with permission only. Up to three contacting attempts were made. Nominees were recorded as “cannot be contacted”, “not available”, “refused”, or “not contacted” for strategic or logistic reasons.
Seeds
Recruitment began with six purposefully selected seeds, varied by sex (four men, two women), age (M = 54.3; range = 34-64), income (three above, three below the national net average), education (five university, one secondary), and employment (one retired, three public sector, one private sector, one self-employed). Seeds were identified during the preparation phase and selected using maximum-variation sampling. We monitored referral chains, documented exclusions and reasons, and tracked demographic variation among referrals to mitigate typical biases in link-tracing (e.g., self-selection, masking, network centrality, availability, and communication biases). Reported reasons for seed refusals included reluctance to discuss medical topics, prior negative experiences with social research, lack of financial incentives, and low trust in external researchers.
Rationale for Size and Timing
Baseline size reflected methodological goals and logistics (budget, field capacity, time). It ensured coverage across demographic strata (age, sex, education, and income) and sufficiently connected recruitment chains for longitudinal and comparative analyses. Wave 2 occurred six months after Wave 1, while Wave 3 occurred twelve months later. The intervals balanced generator design (from fixed to free-choice) and the need to capture structural and compositional change. Waves 2-3 prioritized maintaining the baseline; new recruits filled under-covered strata. Two further waves are planned (September 2025 and March 2026) at six-month intervals.
Field Implementation
Baseline Sample
Wave 1 included 83 participants (M age = 54.3, SD = 15.7, range = 18-80). Sex distribution was balanced (53.0% female and 47.0% male). The largest age group was those aged 65 years or older (33.7%). Education: 42.2% secondary/high school; 34.9% bachelor’s degree. Employment: 54.2% employed/self-employed; 37.3% retired; 4.8% homemakers; 3.6% students. Monthly personal income was most often ≤ EUR 500 (42.1%), i.e., below the national net minimum salary. Most were married (78.3%). Mean household size was 3.3 (SD = 1.5; range = 1-7). Data completeness was high (97.6% complete across five key demographics; two income values were missing). See Table 1S in the SM for details.
Recruitment Network and Diagnostics
The cumulative link-tracing network comprises 261 unique nodes and 298 unique edges (Figure 3). We interviewed 122 people (46.7% of all unique nominees) and had five refusals (1.9%). We also did not contact 118 individuals (45.2%), a number that declined across waves (W1: 49; W2: 39; W3: 29), because we ceased recruitment once we reached our target and due to logistical constraints. To avoid cluster over-recruitment, referrals were limited to five per participant (Waves 2-3), and a sixth seed was introduced in Wave 2 to broaden coverage. Additional analysis showed age-group homophily in nominations but no significant effects for sex or education. While we acknowledge the biases inherent in link-tracing, our sample reflects the community’s structure within the available parameters, even though our research objectives did not require a representative sample. Table 2S (SM) presents descriptive statistics on participation patterns and recruitment outcomes across waves. Directed link-tracing recruitment network. Note. The image displays the directed network representation of the link-tracing recruitment process across all waves (n = 261 nodes; 298 unique edges). Nodes represent individuals, with colors indicating recruitment outcomes: black = interviewed, mauve = not contacted, blue = not available, teal = cannot be contacted, and orange = refused. Seeds are shown as circles with mauve borders (five interviewed seeds in black and one non-interviewed seed in orange). Arrows indicate recruitment nominations from one individual to another. Arrow color varies by connection type, with black arrows linking two interviewed participants and light-grey arrows linking an interviewed participant to a non-interviewed nominee. The layout is based on the Fruchterman–Reingold algorithm to clarify the cluster structure
Interview Duration and Panel-Conditioning Checks
The mean interview duration decreased from 81.4 minutes (Wave 1) to 43.7 minutes (Wave 2), then increased to 52.2 minutes (Wave 3). The drop from W1 to W2 aligns with the protocol change (from fixed to free-choice generators), whereas the rise from W2 to W3 argues against a simple conditioning explanation (we used the same free-choice name generator in both W2 and W3). At the case level, 73.7% showed reductions of more than 30 minutes from W1 to W2, whereas 64.9% showed increases of more than 10 minutes from W2 to W3. We modified the protocol after W1, as both study participants and the citizens’ jury requested shorter interviews. Further, we found that demographic subgroup patterns were not significant, and the interviewer-continuity effects were small and non-significant across the two intervals. Tables 3S and 4S (SM) provide additional statistics on interview duration by wave and interviewer.
Alter-Elicitation Patterns Across Waves
Summary of Implementation Metrics Across Three Waves

Note. †Recruited this wave = interviewed + not available + refusals + cannot be contacted. Panel retention refers to the proportion of interviewed participants who participated in all three waves. The success rate is enrolled/recruited per wave. Detailed category breakdowns (not contacted, cannot be contacted, etc.) and wave-by-wave unique are provided in Table 2S from the Supplementary Material.
Data Analysis Approach
We combined quantitative and qualitative methods to analyze the raw empirical data. We processed and visualized network data using available packages or algorithms in R (R Core Team, 2024), RStudio (Posit Team, 2024), and visone (Brandes & Wagner, 2004). Also, we analyzed the structural data using standard measures of ego-network composition and structure available in the field (McCarty et al., 2019; Wasserman & Faust, 1994), including size, density, multiplexity, and turnover across waves. To assess change, we examined both absolute differences in network indicators and stability of ties between waves. We detected clusters and estimated assortativity (i.e., the tendency of similar nodes to share ties) using special algorithms (Hâncean, Lerner et al., 2025). Additionally, we paid particular attention to detecting data inconsistencies and cross-validating ego reports, i.e., a challenge in longitudinal network research (Bidart et al., 2018; Fischer & Offer, 2020).
Qualitative data consisted of field notes, interview observations, and documentation of community-level activities. We wrote the field notes and observations at the end of each fieldwork day. Moreover, we performed a Net-Map exercise (Schiffer, 2007) (i.e., a stakeholder network creation by an interview-based mapping toolbox) with public health experts to understand the health-related context that embeds the rural community (Mihăilă et al., 2026). We organized these materials thematically and discussed them in internal research team fieldwork meetings. This contextual analysis informed the interpretation of quantitative results, including the mechanisms underlying observed patterns of stability and change, as well as the potential factors influencing study participation (Charmaz, 2014; Maxwell, 2013). Additionally, the qualitative data helped us better understand how residents conceptualize “a healthy dish”, “the image of a healthy body”, or “under what condition” somebody should go to the doctor.
Examples of Qualitative Inputs to Quantitative Implementation
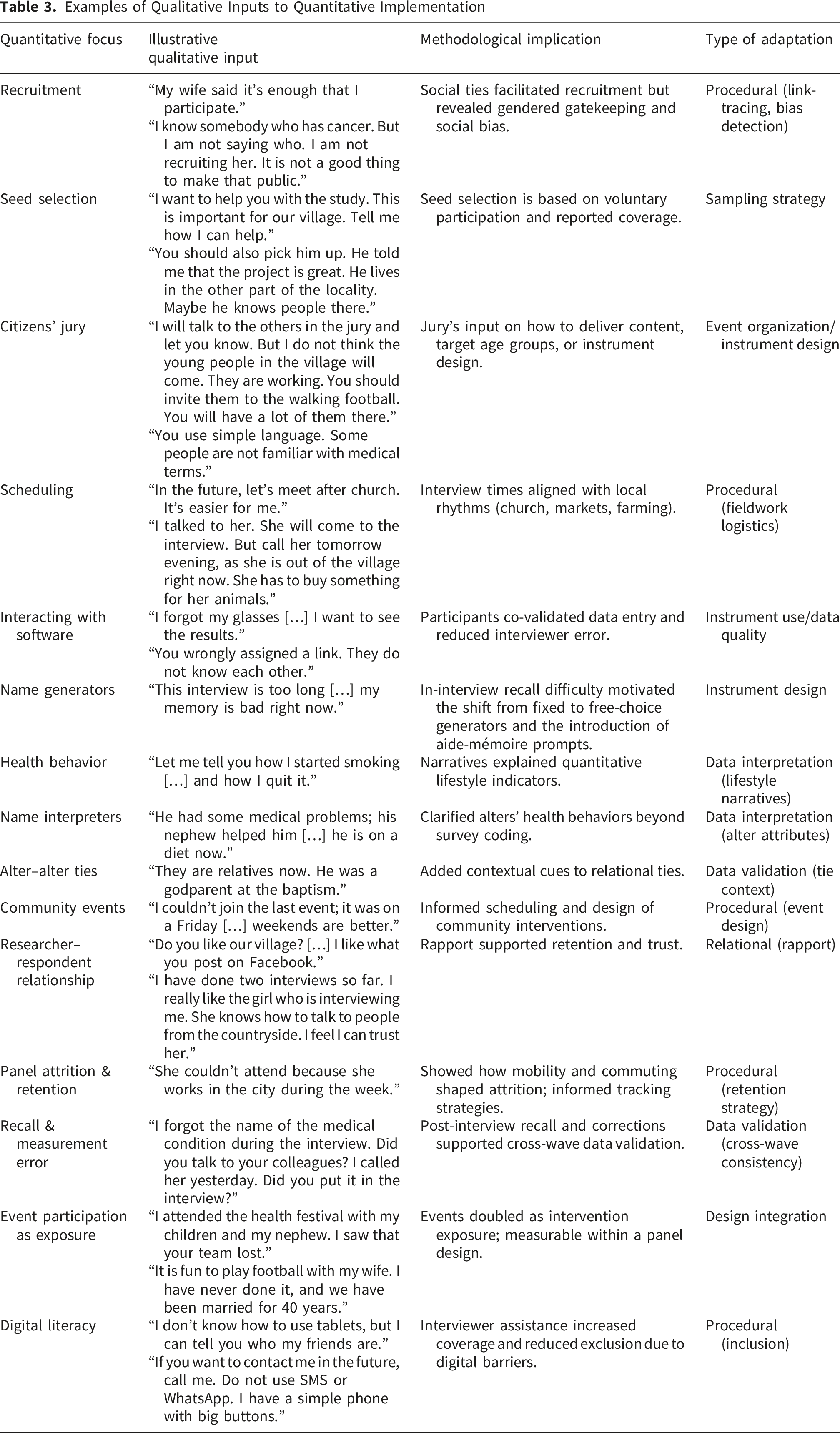
Our study was designed as a longitudinal, mixed-methods community living lab integrating quantitative and qualitative components in a continuous feedback loop. Each survey wave combined structured personal network data collection and quantitative analysis with qualitative elements (e.g., participant observation, interviews, informal discussions, and team reflection). This parallel and iterative structure (Figure 4) allowed the quantitative results to inform the next wave’s fieldwork design, while qualitative insights contextualized patterns observed in the network data. In this way, both strands were mutually reinforcing, ensuring that the evolving instruments and interpretations remained empirically robust, culturally grounded, and sensitive to community dynamics across waves. Integration of quantitative and qualitative components across longitudinal waves in the community living lab. Note. The figure illustrates the iterative design of the study, where quantitative activities (research design, recruitment, events, data collection, analysis, and feedback) and qualitative activities (participant observation, interviews, informal discussions, analysis, and team consensus) informed one another across three waves. This cyclical process reflects the mixed-methods nature of the community living lab, ensuring that each phase was both data-driven and grounded in community experience
Reflexivity and Positionality
The research team entered the study as outsiders to the rural community. Based at urban universities and trained in sociology and public health, we were aware that our institutional affiliations and professional backgrounds positioned us as external experts. This status influenced how participants perceived the project, sometimes generating respect and expectations of expertise and at other times creating a sense of distance. As noted, we used our field notes and learned from our interactions with people in the rural community to ensure that our instruments, procedures, and interventions were adapted and incorporated community perspectives.
Reflexivity was practiced throughout the fieldwork. Notably, we documented how our presence and questioning shaped responses, for example, when participants emphasized health risks they assumed were of interest to “university people”. Being recognized as outsiders (“professors and medical doctors from the city”) required us to deliberately cultivate trust. Strategies included participating in community gatherings, attending church services and local markets, and maintaining a long-term presence across multiple waves. In response to feedback, we adapted the instruments, such as shifting from fixed to free-choice name generators or refining the questions.
Positionality also shaped data interpretation. As outsiders, we may have had limited access to sensitive topics, such as family conflicts, illness, or informal coping practices. However, this distance encouraged participants to explain everyday routines and community norms in greater detail. This contextual information might have been taken for granted by insiders. By explicitly reflecting on these dynamics, we aimed to enhance the credibility, transparency, and transferability of the study (Berger, 2015; Goundar, 2025; Holmes, 2020).
Ethical Considerations
We followed established ethical standards for research involving human participants. All research procedures complied with the Declaration of Helsinki and the European General Data Protection Regulation (GDPR). The study was approved by an ethics committee. All participants provided written informed consent prior to each wave of data collection. The consent process emphasized voluntary participation, the right to withdraw at any time, the confidentiality of personal information, and agreement to the scientific publication of anonymized data for scientific purposes.
We anonymized personally identifiable information after each interview and securely stored data on encrypted drives accessible only to authorized personnel. No raw identifiable data were shared outside the research team, and dissemination was conducted in a format that prevents deductive disclosure. To protect privacy, identifying information about alters was stored separately from survey data and pseudonymized during analysis. We shared only aggregated results with the community. Feedback sessions with study participants and the citizens’ jury were used to return findings in accessible formats (e.g., network animations) and to maintain reciprocity and accountability (Flicker et al., 2007).
Participatory design raised specific ethical issues. Collaborative adaptation of instruments required balancing community input with concerns about data comparability across waves. We employed iterative feedback, transparent communication, and consultation in the decision-making process to address the power asymmetries between researchers and participants. Working in a rural setting also required sensitivity to potential stigma. We discussed health behaviors and cancer risk only during one-on-one sessions, which were organized carefully to avoid singling out individuals or households. Researchers embedded themselves in community life, allowing trust to develop gradually. These measures minimized risks while supporting ethical principles of respect for autonomy, nonmaleficence, and justice (Beauchamp & Childress, 2019). As part of our commitment to transparency and accountability, the research team provided participants with their professional contact details, including institutional email addresses and official social media profiles, to facilitate ongoing communication, address study-related questions, and support trust-building.
Discussion
Adapting longitudinal research to rural contexts requires rethinking recruitment, instrument design, and retention beyond traditional approaches. We offer five methodological insights from our experience that can be organized in a provisional transferable framework. First, we used link-tracing to embed enrollment in existing relational structures, to reinforce trust and support retention (Heckathorn, 1997; Metz et al., 2022). Second, adjusting the instruments to feedback reduced cognitive burden, improved collaboration, and ensured that participants acted as co-designers (Tremblay et al., 2020). Third, software-supported elicitation improved feasibility. Using Network Canvas reduced data-entry errors and enabled real-time interaction. The visual interface facilitated comprehension even in a low-digital literacy context, while offline functionality ensured continuity despite poor internet connectivity (Hogan et al., 2016). Fourth, we sustained retention through relational recruitment, prolonged community presence, citizen engagement, and interviewer continuity across waves (Lugtig, 2014). Fifth, we adapted data collection timing to local rhythms (agricultural cycles, weekly markets, and church services), thereby increasing participation and reducing the number of refusals.
These insights may have several methodological implications. First, relational recruitment strategies, such as link-tracing, are well-suited for contexts where formal registries are weak or inaccessible. Second, participatory co-design of instruments can enhance engagement and cultural fit, but it requires striking a balance between flexibility and cross-wave comparability. Third, digital tools that integrate visualization and interaction can facilitate network elicitation, even in low-literacy settings, provided adequate interviewer support is available. Fourth, methodological rigor in longitudinal network studies must be balanced against field adaptability: participatory and flexible approaches may reduce standardization but facilitate ethical reciprocity and data quality.
Our work is subject to several sources of bias and other inherent limitations. Our research objectives did not require working with a representative sample, but several factors shape how the data should be interpreted. Because we recruited through link-tracing (participants nominated others from their networks), the sample approximates the structure of those existing relationships and likely underrepresents more isolated individuals. The non-monetary incentives that we offered may also have appealed more to residents who were already health-conscious. Some participants may have chosen not to mention or recommend certain people from their networks (a masking effect), which limited who could be reached for recruitment. Variation in respondent availability and in the communication channels used to reach nominees may have introduced further residual biases despite the monitoring procedures described in Methods. Participatory adaptations enhance cultural fit while reducing strict standardization, which, in turn, may limit comparability across waves. Reliance on digital tools, even with interviewer assistance, may exclude those with very low digital literacy or education. Our visible presence in the village helped establish trust but may also have influenced how participants represented their networks, particularly in terms of health behaviors (e.g., desirability effects). Finally, relational and participatory strategies require intensive resources, which may be difficult to replicate in large-scale or multi-site studies.
Despite these constraints, we illustrate how longitudinal personal network designs can be adapted beyond urban survey traditions. The combination of link-tracing recruitment, participatory instrument adaptation, software-enabled elicitation, and community-based retention strategies offers insights for a transferable methodological framework. These practices may guide future mixed-methods health research in small communities where weak infrastructure and limited digital and survey literacy pose obstacles.
Supplemental Material
Supplemental Material - Adapting Longitudinal Personal Network Research Through Participation: Reflections From a Rural Study
Supplemental Material for Adapting Longitudinal Personal Network Research Through Participation: Reflections From a Rural Study by Marian-Gabriel Hâncean, Christopher McCarty, José Luis Molina, Marius Geantă, Jürgen Lerner, Bianca-Elena Mihăilă, Iulian Oană and Cosmina Cioroboiu in International Journal of Qualitative Methods.
Footnotes
Acknowledgments
We gratefully acknowledge the residents of Lereşti for their participation, trust, and collaboration throughout this study. Special thanks are extended to the members of the local authorities, study participants, and local citizens’ jury, whose input and feedback were crucial in adapting the research design to the community context. We also thank Ph.D. Maria-Cristina Ghiță, Bogdan-Adrian Vidraşcu, Maria-Alexandra Roşu, Andreea Ștefania Moise, and Antonin Tron-Lozai for their assistance with this study. Finally, we are grateful to our colleagues from the Center for Innovation in Medicine, the University of Bucharest (Department of Sociology), and the 4P-CAN consortium for their methodological insights and constructive discussions that supported the development of this work.
Ethical Considerations
We followed established ethical standards for research involving human participants. All research procedures complied with the Declaration of Helsinki and the European General Data Protection Regulation (GDPR). The study was approved by the Ethics Committee of the Center for Innovation in Medicine (EC-INOMED Decision No. D001/09-06-2023, No. D001/19-01-2024, and No. D002/03-02-2025).
Consent to Participate
All participants provided written informed consent prior to each wave of data collection. The consent process emphasized voluntary participation, the right to withdraw at any time, the confidentiality of personal information, and agreement to the scientific publication of the anonymized data.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: M.-G.H., M.G., B.-E.M., C.C. and I.O. were supported by the 4P-CAN project, HORIZON-MISS-2022-CANCER-01, project ID 101104432, programme HORIZON; J.L. was supported by Deutsche Forschungsgemeinschaft (DFG 555455503). The funding sources had no involvement in the study design, in the collection, analysis, and interpretation of data, in writing the paper, and in the decision to submit the article for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset analyzed in the current study and the R code (as Supplementary Material) are made openly available in the Zenodo data repository as Hâncean, McCarty et al., 2025. The supplementary material includes the code and the data used in this paper. The personal network data contain sensitive information about individuals and their social relations. For reasons of confidentiality and to prevent deductive disclosure (especially given the size of the community), raw data cannot be shared publicly.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.