
Abstract
Background
In recent years, there has been an increasing shift toward more collaborative approaches to research, with greater inclusion of diverse patients and community members in the research process. However, further exploration is needed to understand the factors that contribute to research partners feeling valued within teams. Gaining this insight could help foster supportive environments that empower these individuals to meaningfully contribute their expertise.
Purpose
Our research aims to understand what makes patients and community partners, specifically those who experience barriers to engagement in research, feel valued in the patient-oriented research (POR) process.
Methods
We conducted semi-structured interviews with 37 participants located in communities across British Columbia, Canada. Participants were identified as patients, community members, knowledge users, and researchers engaged in POR. Here, we draw specifically on the insights of 14 participants who identified as patient or community partners. Data were analyzed thematically, and an intersectionality lens was adopted to sensitize the research to the complexities and interactions of diverse and overlapping social locations in research.
Results
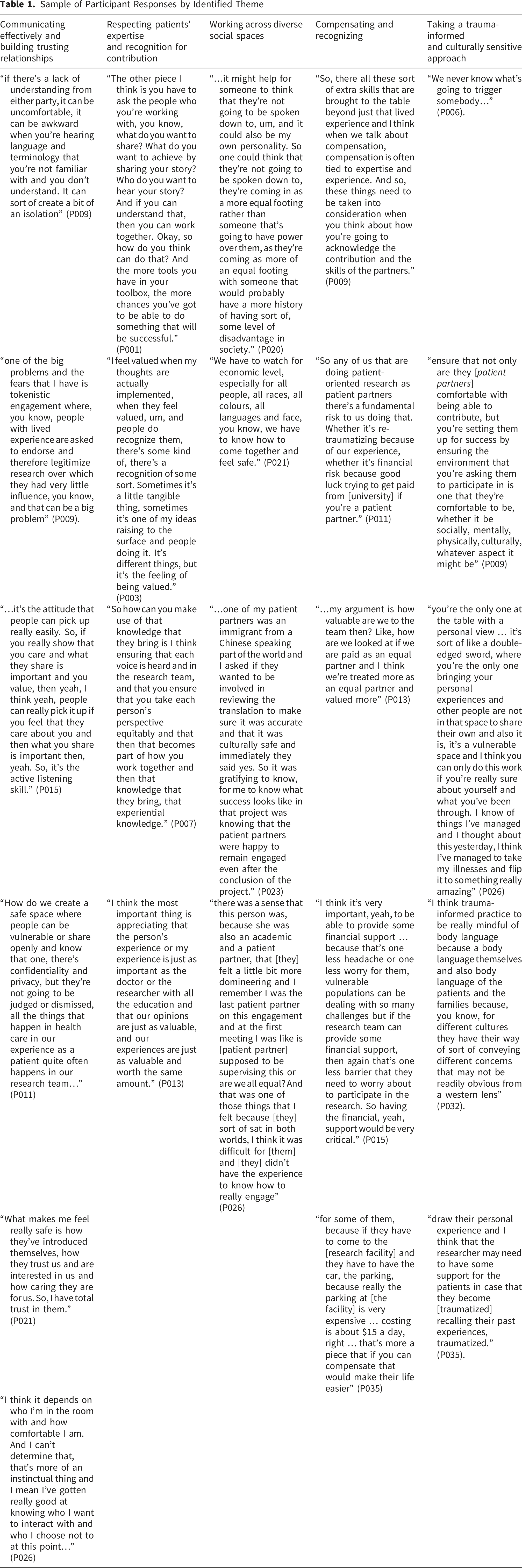
Five themes emerged from our data analysis that focused on factors that make patient partners feel valued. These include: (1) building trusting relationships and communicating effectively, (2) respecting the patient partner’s expertise and recognition for their contributions, (3) working across diverse social spaces, (4) compensating and recognizing, and (5) taking a trauma-informed and culturally sensitive approach.
Conclusions
Optimal patient engagement is vital for knowledge generation, with the potential to enrich research projects and their related impacts. Our research highlights factors that should be considered for a productive knowledge exchange in the context of patient-oriented research with patients from diverse communities.
Keywords
Introduction
Among healthcare goals, the identification of methods, tools, and services that address patient needs is an important global priority. However, the achievement of this objective continues to be hindered by the inadequate inclusion of patient and community voices in the research process (Barello et al., 2012). Despite long standing calls for greater inclusion of patient perspectives (Donabedian, 1968), the systematic integration of diverse patient perspectives in health research was, until recently, largely superficial and related to indicators of patient satisfaction (Karam, 2017). Despite more recent interest (Willis, 2022), this lack of perspective continues to perpetuate complex knowledge and practice gaps, along with health disparities, inequities, and poor patient outcomes (Evans et al., 2004; Olson & Windish, 2010; Ross et al., 1995; Wolf et al., 1978; Yellen et al., 2002).
In order to support the creation of knowledge that improves patient and health systems outcomes, patients, families, and caregivers must be meaningfully engaged in research, alongside community-based partners (Al-Abri & Al-Balushi, 2014; Caron-Flinterman et al., 2005; Hamilton et al., 2018; Snow et al., 2018; Tambuyzer et al., 2014). This vital strategy aligns with the broader global movement that promotes patient engagement in research (National Institute for Health and Care Research [NIHR], n. d.; Patient-Centered Outcomes Research Institute [PCORI], n. d.) and emphasizes the need for more democratic and socially responsible research practices (Domecq et al., 2014).
In Canada, the patient-oriented research (POR) initiative was launched in 2011 and signaled the widespread emergence of patient engagement in research, with the intention of supporting healthcare innovation that emphasizes patient priorities and facilitates improvements to health outcomes through integration of the research into policies and practice (Canadian Institutes of Health Research [CIHR], 2019). POR promotes the integration of diverse knowledge systems into health research, including diverse patient voices and experiences. It has been hailed as a mechanism to promote the creation and mobilization of relevant and responsive research that improves health system and patient outcomes, while reducing costs (Allin, 2008; Chalmers & Glasziou, 2009; Devine et al., 2013; Manafo et al., 2018). Despite its many strengths, however, POR has been criticized for failing to adequately engage patients with diverse experiences and perspectives (Bishop et al., 2018; Olson & Windish, 2010; Truog, 2012).
A POR approach requires research teams to adopt collaborative and partnered modes of research, centralize the needs, values, and priorities of patients, build engagement capacity, and integrate diverse perspectives (CIHR, 2024). While the recognition of experiential knowledge remains central to the POR movement, the integration of insights related to equitable health outcomes remains tied to wider societal structures and systems of power. Thus, calls to diversify patient engagement have intensified and include a growing focus on the inclusion of persons with diverse experiences and perspectives, along with the need to promote culturally competent practices that support equity, diversity, and inclusion (Frisch et al., 2020; Michalak et al., 2023).
Creating opportunities to meaningfully engage diverse patients experiencing barriers to engagement, along with adopting appropriate and sensitive methods of inquiry, offers an opportunity to address gaps in knowledge and foster evidence to drive needed health system change (Roche et al., 2020). While many examples of successful engagement have been offered in the literature (Frisch et al., 2020; Michalak et al., 2023; Roche et al., 2020), complex challenges are noted. In particular, POR has been criticized for its tendency to engage homogenous patient groups based on a single category of difference (e.g., women with cancer) while contributing to the ongoing exclusion of hardly reached or marginalized populations (Ocloo & Matthews, 2016). For example, many of the patient partners involved in POR tend to be white, middle-class women, leaving out other valuable voices (Michalak et al., 2023). Underrepresented voices may include populations that experience challenges when accessing healthcare services, including those living with complex and stigmatizing medical conditions, Indigenous and/or racialized people, immigrants and refugees, older adults, and those residing in rural, remote, and northern populations (Allin, 2008; Roche et al., 2020). In Canada, northern communities are commonly geographically distant from larger urban centers and are characterized by unfavorable health outcomes, including a lack of resources and chronic health human resource challenges (Schiff & Møller, 2021).
Adopting an intersectionality lens and trauma-informed approach to engagement can advance and create spaces for the inclusion of diverse communities, which considers individuals from various cultural and historical backgrounds, as well as their social context (e.g., race, ethnicity, gender, sexuality, age, ability, religion, etc.; Shimmin et al., 2017). Through critical reflection researchers must consider the complex, intersecting, and overlapping factors that impact health and the experience of healthcare. This includes actively challenging and deconstructing dominant discourses in healthcare and research, adopting culturally sensitive and inclusive research practices, and creating safe and welcoming spaces that value diverse knowledge and perspectives (Ellemers et al., 2013).
As engagement with the experiences of diverse patient populations increases, so too must our understanding of how to effectively conduct POR, particularly in light of previously identified negative experiences that are common (Tischler et al., 2010). Our research aims to address this gap by drawing specifically on the insights of patients and community partners to understand what makes patients (and specifically those who experience barriers to engagement in research) feel valued in the research process.
Methods
This work is part of a larger study exploring the engagement of populations that face barriers to engagement in POR. As part of this study, we interviewed diverse stakeholders, including patients, the public, knowledge users, researchers, and not-for-profit organizations engaged in POR with diverse populations (i.e. immigrants, refugees and newcomers, ethnic minorities, housing insecure and low-income individuals, Indigenous community members, older adults, and populations living with complex health conditions, or in rural, remote, and northern communities). We specifically sought to understand experiences of, barriers to, and facilitators of engaging in POR. In this paper, we present the insights shared by community and patient partners who participated in POR teams, highlighting the unique contributions and challenges faced when engaging in collaborative research.
Theoretical Positioning
To gain deep insights about diverse patient experiences and meaningful inclusion in POR, we used a critical, qualitative exploratory method informed by principles of equity and intersectionality whose theoretical underpinning is explicitly oriented towards transformation, building alliances among different groups, and working towards social justice (Collins & Bilge, 2020; Crenshaw, 2017). Grounded in the work of Black feminists, intersectionality adds a distinct analytical lens that challenges researchers to consider the impacts of diverse overlapping and interconnected systems of power (such as sexism, racism, and ableism). These systems give rise to unique experiences of health and wellbeing, including marginalization (Abrams et al., 2020). Further informing our analysis are key principles relating to power, inclusion and representation, social justice and equity, social locations, safety, reflexivity, and diversity of knowledge. Guided by Bauer (2014), we adopted an intersectionality approach which includes: (1) considerations of how complex and intersecting identities impact engagement experiences, (2) engagement with diverse communities of patients and researchers to inform the project, and (3) the adoption of multidimensional and anti-categorical approaches to analyzing data from individuals with diverse identities and social locations (such as gender, practice position, and ethnicity).
Reflexivity and Positionality
To ground our research within collaborative practices, we used an Integrated Knowledge Translation (IKT) approach. Planned from the outset, this approach provides a collaborative research framework that sets out processes for exchanging knowledge, making decisions about methodology and stipulating involvement in the collection, interpretation, and dissemination of data between the researchers and knowledge users (Kothari & Wathen, 2013). Of note, our team was co-led by a patient partner and included leaders from two not-for-profit community agencies that work with communities facing complex health and social care issues. By adopting this approach, our team worked to foster meaningful partnerships by promoting inclusive team activities, conducting frequent meetings, and creating a plan to facilitate and support recommendations. This collaboration helps to facilitate mutually beneficial research studies to address the priorities of knowledge users.
Our research team itself reflected diverse backgrounds, with respect to key demographic (e.g., gender, age, ethnicity, location) and professional (e.g., career stage and roles) characteristics. This enhanced the conceptualization and implementation of the research and provided opportunities for capacity building and mentorship. Of note, the team included researchers from three universities across British Columbia, a patient-partner who led and co-led several research activities, two community knowledge users, and a librarian. Research assistants and trainees from different stages of their education were engaged, including undergraduate, graduate, and post-doctoral trainees from a variety of disciplines, including public health, psychology, nursing, and environmental studies. Team members also represented diverse ethnic and racial identities, with several having minoritized backgrounds.
Participant recruitment was approached thoughtfully, particularly when potential participants had pre-existing connections with team members, to ensure that participation was voluntary and free from any sense of pressure. Participants received consent forms and interview schedules in advance of data collection and were given a minimum of 24 hours to review all study materials prior to the interview. They were also invited to request any support needs for the interview (e.g., translation services) and could opt to complete the interview in a dyad if there were concerns about potential power imbalances. Throughout all interactions, researchers used inclusive language, including respecting participants’ preferred pronouns and accommodating participants’ language and syntax.
Sample
To recruit our study sample, we utilized purposeful and snowball sampling techniques. Team members utilized their own connections within communities to identify potential participants. Snowball sampling techniques were also employed to garner participation from individuals who have engaged in POR partnerships that were both successful and unsuccessful. The participants for this study were pulled from a larger sample of 37 participants that were part of a larger study. This paper focuses on the 14 participants that were identified as patients or community partners engaged in POR. Participants were recruited from across all geographic areas of British Columbia, Canada, with over 60% living in Vancouver and surrounding areas and 29% in northern and rural British Columbia. Moreover, the 14 participants ranged in age from 38 to 79 years old, with 11 identifying as female, two identifying as male, and one choosing to not disclose their gender. Regarding ethnicity, of those who disclosed theirs, six reported that they were Caucasian, Canadian, or a White settler and four identified themselves as Korean, Chinese, or Indian. 12 participants were interviewed individually and two were interviewed in a dyad. In this paper, we draw directly from the insights of the patient and community partners.
Data Collection and Analysis
Our research was informed by a critical theoretical approach of intersectionality and included an intentional exploration of how interaction of different social locations (e.g., ‘race’/ethnicity, Indigeneity, gender, class, sexuality, geography, age, disability/ability, gender, class, sexuality, migration status, religion) shaped participants’ experiences of partnerships (Bauer, 2014; Bowleg, 2012; Hankivsky, 2022). In our interviews, we sought to curate brave and safe spaces in which participants were able to share their own experiences of POR and social exclusion and discuss their broader engagement within the POR landscape.
To generate in-depth and rich accounts, semi-structured interviews were conducted by experienced qualitative researchers (DB, NC, SM, SD). A preliminary interview schedule was co-created by members of the research team, including patient and community partners (see Appendix A). During the interview, we asked questions aimed at uncovering experiences with, barriers to, and facilitators of engagement in POR, including asking open-ended questions about how their own social locations impacted their experiences of engagement and partnerships. The semi-structured interview approach both supported the in-depth exploration of the focal topic and provided the opportunity to garner broader insights and experiences. Interviews took place via telephone or Zoom and lasted up to 90 minutes. These were digitally recorded and transcribed verbatim. Only the data originating from individuals who identified as patients or community partners were analyzed for this portion of the study.
Thematic analysis was utilized for this study (Braun & Clarke, 2006). Data were first cleaned for accuracy and then de-identified and stored securely in an encrypted and password-protected platform. Data were read closely prior to analysis, allowing for immersion in the data, and then coded using a qualitative software program (NVivo 12). Initial codes were generated independently by a team of researchers (DB, NC, SD, KG, JG, and JF), with each of the transcripts coded at least twice independently. Preliminary themes and interconnections were documented in an analysis table and shared with the research team. Focused discussions were undertaken to support ongoing data analysis and interpretation. The analysis table was updated and then supplemented with illustrative quotes and descriptors. Analysis of sex- and gender-based considerations was undertaken and extended further through intersectionality theorizing. Specifically, we adopted a critical stance toward categorical theorizing, which includes intra-categorical analysis to reflect the complex and overlapping impacts of power and social location (McCall, 2005). Having determined that theoretical saturation had been accomplished, no further participants were recruited (Fusch & Ness, 2015; Sandelowski, 1995).
Ethical Considerations
The study underwent harmonized research ethics board review and was approved [H19-01726-A001]. All participants were provided with a letter of introduction, a comprehensive information sheet, and consent form. Participants were encouraged to contact the lead researcher if they had further questions or concerns or wanted further information. Participants were given the option to provide either written or verbal consent, and ongoing verbal consent was confirmed prior to any data collection. In addition, data was de-identified to promote confidentiality. Given the sensitive nature of the research, care was taken to foster safe and inclusive environments. Participants were made aware that they were able to refuse to answer any questions and were provided with a list of accessible support services if needed. Likewise, the demographic survey was designed to allow for identification of various social and demographic characteristics that helped us to define our study sample and ensure that diverse perspectives were included in the research. Participants were encouraged to only answer what was comfortable.
Rigor
To facilitate the credibility of our findings, we engaged in prolonged immersion in the data, providing detailed descriptions and excerpts reflecting diverse patient experiences and voices. Additionally, we continuously involved community and patient partners on the team to reflect on and ground our analysis in the lived experience of the participants. The insights of community and patient partners were instrumental in supporting the analysis of the data and helped sensitize the team to tacit assumptions and more nuanced interpretations.
Findings
Sample of Participant Responses by Identified Theme
Building Trusting Relationships and Communicating Effectively
As a central aspect of the POR experience, participants unanimously identified the importance of building trusting relationships between researchers, fellow patient partners, and knowledge users. When strong and trusting relationships were not formed, participants described that this adversely affected their ability to engage and gave rise to concerns about tokenism, meaning that participants’ involvement was cursory as opposed to meaningful. Participants noted that poor relational practices restricted productive conversations, gave rise to concerns about the credibility of the research, and limited the perceived value of collaboration (described by one participant as “tokenistic”). Central elements of trusting relationships were described by participants through several subthemes.
Comfort and Trust
Among participants, comfort and trust were prominently discussed as being central to a successful research relationship. The need for meaningful and sustained connections, along with trust, was particularly critical among those who navigated multiple complex systems of social exclusion and stigma, including immigrant and refugee, Indigenous, and medically complex communities. Participants described that an embodied sense of comfort and trust within the individual interactions and/or relationship was essential and determined their decision to participate and level of engagement. For some participants, comfort and trust also extended beyond their individual experience and extended to consideration of the broader communities to which they are connected. For example, one community and patient partner commented that they would likely participate in POR initiatives where they believe that a researcher is an ally or steward of the conversations that the participant represents or believes in (P011).
Mutuality
A key factor that emerged regarding value in a relationship is the feeling that a relationship was reciprocal and mutually beneficial, based on collaboration and structured to reflect the importance of patient partners as equal contributors. Some participants shared examples of challenging experiences during their POR roles, particularly expressing that they felt dismissed, unheard, or undervalued. However, some participants also commented that engaging in POR gave rise to new opportunities, including offering new career pathways and ways to work with research teams and associated organizations One patient partner described their increasing engagement in POR a means of going “from being a person with a [disability] with an interest in research, to participating as a research subject, to informing research and becoming a co-investigator on a research project, working for a research organization, and specializing in engagement of people with lived experience” (P009).
Intentional and Sensitive Approaches to Engagement
Many participants explained that intentional and sensitive approaches to engagement were needed in order to foster buy-in, support, and trust. On this point, one patient partner illustrated the importance of protecting relationships and the “researcher being conscious of the sensitivity of the experiences that they are looking to gain access to” (P022). For this participant, comfort and trust was established when researchers ‘showed up’ in the right way, with the knowledge and tools to effectively engage and respect the needs of the community in focus. For some participants, engagement also required deliberate and intentional actions to mitigate and neutralize power imbalances. For example, one patient partner explained that “if there’s a domineering or a power base that’s trying to, that’s just trying maintain control, I will feel it, or I feel it inside, even though, you know it’s not necessarily any words that are said, but it’s a feeling that is projected and again” (P003).
Mitigating Conflict
For other patient partners, the ability to manage and mitigate conflict was seen as a critical factor in building, establishing, and sustaining effective POR relationships. Many examples of conflict and conflict resolution within POR teams were shared during the research, including situations where expectations between partners were mismatched. One participant identified the ability to resolve conflicts and negotiate resolutions as a good indicator that a project is “going well” (P015).
When discussing the importance of trusting relationships, participants often pointed to a related theme of effective communication. When asked about their prior experiences with POR, participants frequently described how communication acted as a central lever of power, meaning that communication (or lack of thereof) was a tool for determining (or limiting) access, inclusion, and value within the team. With respect to the importance of communication, participants identified a number of barriers and tools that impact the POR experience, including:
Use of Jargon
The use of jargon or other inaccessible technical language was consistently identified as a barrier to engagement, with participants explaining that this often left them feeling excluded and limited their ability to contribute to the discussion. Participants further expressed that effective communication, particularly when it comes to understanding and using technical jargon, requires significant effort and development on their part (who must learn the terminology), as well as the broader research team (who must learn to accommodate those with diverse abilities and first languages). These issues were particularly relevant when teams were addressing more technical elements of the research, including reviewing research protocols, reports, or manuscripts. One critical strategy that was identified as a means to address this communication gap was the use of inclusive, sensitive, and plain language, hailed as a means of ensuring that everyone can understand the material and participate actively within the research activities.
Active Listening
Among participants, active listening skills were perceived as a key component in fostering effective and valuable communication, whereby team members responded in a way that created spaces of inclusion and co-learning. By supporting active listening within the team environment, patient partners felt able to contribute fully, which in turn helped them feel ‘genuinely heard’ and that what they were sharing was of value. Regularly reviewing and assessing communication, and in particular the use of active listening and the avoidance of derogatory terminology, was seen as an essential means of facilitating meaningful partnership spaces and avoiding superficial and tokenistic exchanges.
Open Communication
Participant feedback demonstrated that open communication is a central means of fostering safety for patients and community members engaged in POR. Participants recognized that consistent clarification around expectations, in particular confidentiality, along with steps to explicitly value their experiential knowledge, were important relational practices that created feelings of safety and trust. Similarly, engaging patient partners and community partners early and continuously throughout the research process, was seen as a necessary part of open communication. For immigrant, refugee, and newcomer populations with diverse first languages, participants recognized the importance of facilitating access to translators or translated materials as a mechanism to minimize barriers. Doing so allowed for the inclusion of contextual and experiential insights within the decision-making process. Actively engaging, listening, and considering patient partners during team activities, including meetings, and being inclusive during the planning phases prior to meetings, facilitated engagement and led to positive POR experiences. However, some participants noted that they were often excluded from communication around planning, leaving them feeling as if their time and contributions were secondary to others.
Respecting Patient’s Expertise and Recognition for Contributions
Community and patient partners expressed desire for greater recognition of their contributions, in particular noting that their contributions were a legitimate form of knowledge and expertise. For many participants, their engagement was perceived as offering important social and economic benefits, including making the research more socially responsible and impactful. One patient partner noted that the publicly funded nature of research gives rise to an onus and expectation that the research being conducted “will impact the people it’s intended to assist” (P009).
Underpinning participants’ expectations of engagement was a desire to be treated equally within the team environment. This included having their contributions and time valued in the same way as it is for researchers and other knowledge users. One participant commented that their experience is “just as important as the doctor or the researcher with all the education” and that participants’ opinions and experiences are “just as valuable and worth the same amount” (P013). Participants noted that while researchers may have greater expertise in relation to research methodology and the technical aspects of the work, the experience of community and patient partners could provide further context to the focal topic and support more impactful outcomes and policy. This was seen as particularly important when conducting research with equity-deserving populations that have experienced significant barriers and marginalization. In particular, participants engaging in POR with immigrant, refugee, and newcomer populations and Indigenous communities noted the need for researchers to have well established expertise and experience, understand and unmask underlying racism and structural disparities, and appreciate the uniqueness of the population or community. Of note, some newcomer participants expressed profound caution around engagement activities, noting fears related to cultural, social, or political viewpoints of research. For example, one participant expressed explicit concerns related to research during the COVID-19 pandemic, recalling fear for the safety and wellbeing of their families within their home country if traced back.
During the interviews, participants also shared their desire to contribute as ‘whole’ individuals, recognizing their varied life experiences beyond their lived experience of a health issue. Some participants shared that they were experienced in other professional areas, which allowed them to have skills that could be utilized for additional pieces of the research project (e.g., community connections, interviewing skills, etc.). Many of the participants expressed that these varied experiences and skills were not widely recognized, valued, or utilized in their previous experience with POR.
When asked about strategies that may support participants to feel valued within a POR team, community and patient partners explained that teams should be willing to embrace their contributions and integrate these within the research. In particular, participants felt that researchers should consider their input regarding the topics and research questions they find interesting and important, rather than being a ‘token’ that furthers the curiosity of the researcher. Thus, participants expressed a desire that research studies should be tailored to, or include, the interests of the patient partner or the community more broadly.
Finally, participants noted that seeing something come out of a research project was an important way in which they came to feel valued. One community partner, who supports research teams in research with multiple marginalized populations, noted that there was a need to intentionally document how the contributions of those with lived experience impacted the work. For this participant, an opportunity existed to “create the narrative that her research brought forward and to use it not only to tell our story, but to hopefully have it as a very accessible manual for others” (P022). Other participants noted that seeing the outputs of the research, through knowledge mobilization, reinforced the value of the work and their contributions and made meaningful impact within their communities.
Working Across Diverse Social Spaces
When asked about how their own social locations intersected and influenced their experience of POR, some of the participants described how they often spanned multiple roles and social locations defined by gender, ethnicity, research capacity, and world view. For some, this means simultaneously occupying positions of advantage and disadvantage. Participants described how these complex positionalities, boundaries, and liminal spaces gave rise to unique challenges and opportunities. For example, one community partner described the duality of being disadvantaged in some ways, while also having the privilege of a Canadian graduate-level education, commenting that “it’s important for people to be aware that all of us have these different identities that give us some privileges and some disadvantages, so it’s important to be aware of this complexity” (P015). By engaging in research in this way, some of the participants reflected that they were navigating two distinct worlds, as well as bringing similar ‘intersections’ that may be experienced by the populations targeted by the research.
Compensating and Recognizing
Compensation and recognition emerged strongly during the interviews and was widely discussed by those with experience as a community or patient partner in POR. While participants noted that compensation and recognition can take many forms, monetary compensation was seen as a primary need in POR involving diverse populations that face barriers to engagement. Participants recognized that conversations around monetary compensation can be challenging, particularly when considering how much should be paid, who should receive compensation, and its prioritization in research budgets. Compensation was seen as a central aspect of feeling valued, closely tied to feelings of equity. Participants noted that while other team members typically participate in a formal and paid role (e.g., primary investigator, research assistant, policymaker, etc.), community and patient partners may be seen as “informal” participants and thus not be paid for their time. Participants felt that they should receive appropriate and timely compensation for their involvement over the duration of their engagement, and that this can help neutralize power imbalances and legitimize their contributions.
Although compensation was viewed as a basic component of participation, many recognized that the costs to participants (including those for attendance, childcare, and transportation) far exceed the financial compensation received. Not offering appropriate compensation to community and patient partners who, unlike researchers and healthcare professionals, are not in a salaried or hourly position, was seen as a key factor that both limited their input and created risk.
Of the 14 participants, 12 described, in some manner, the connection between lack of compensation and the risk that their voices may not truly be valued in the research process. One community and patient partner commented that there is a “fundamental risk” to participating in POR, whether it be the risk of re-traumatization, or financial risk (P011). In addition, participants recognized that equity-deserving populations, and those who already face barriers to participation, are especially impacted when compensation is not offered, and that this may result in harm. One participant noted that “vulnerable populations can be dealing with so many challenges but if the research team can provide some financial support, then again that’s one less barrier that they need to worry about to participate in the research” (P015).
While the desire for appropriate monetary compensation was made clear, alternative forms of reciprocity were also seen as important. For example, some participants indicated that while they may not actually need or want financial compensation in some situations, the meaning of the compensation held value. For some, compensation was a means of legitimizing and valuing their express expertise and contributions as patient partners and community members, as opposed to just their time. As noted, participants also highlighted that their skills typically expanded far beyond lived experience and included broad personal and professional experiences and insights. As many of the patient and community partners captured in this research held prominent roles in their respective communities and related organizations, their contributions included broader professional insights relevant to the engagement of diverse communities. This included a deep understanding of cultural and social values that can underpin meaningful engagement and impactful change. Thus, steps to offer appropriate recognition were seen as important, including direct recognition for their individual contributions and co-authorship on manuscripts.
Taking a Trauma-Informed and Culturally Sensitive Approach
Engaging with POR teams requires a strong sense of humility and reflexivity. This was particularly important among community and patient partners, who were often asked to share personal and vulnerable experiences in a unidirectional manner, without similar vulnerability flowing from researchers. As one participant explained, “you’re the only one at the table with a personal view …it’s a vulnerable space” (P026).
Participants expressed that a safe and inclusive partnership space was critical to enabling them to share their experiences, and that this included a need for research teams to adopt trauma-informed and culturally sensitive practices. In doing this, patient and community participants expressed the need for reciprocity and respect, along with partnership spaces that were affirming, accountable, open, and safe. Participants identified the need for dedicated resources and strategies to support participants, who may experience potential distress, harm, or trauma when sharing their own experiences. For example, for those engaged in research focusing on mental health or substance use disorders, fears of, or experience of, stigma and prejudice was noted and contributed to poor partnership experiences. As one participant cautioned “we never know what’s going to trigger somebody…” (P006), while others discussed experiences of harms and re-traumatization, which left them needing time to ‘recover’ (P026) following research engagements.
When working with culturally diverse communities, community and patient partners recognized that engaging team members with expertise in trauma-informed practices is essential. For some, this was a means of creating spaces whereby the diverse experiences and perspectives that may exist could be acknowledged and recognized, as well as working to establish safe spaces through which the team could discuss and challenge dominant discourses and vantage points around health and healthcare issues. For Indigenous participants, or those engaged with Indigenous communities, the need to centralize community perspectives and needs was recognized, requiring researchers to create meaningful and reciprocal research spaces, recognizing the importance of Indigenous knowledges and worldviews. Furthermore, another patient partner commented on the importance of body language, both in terms of how researchers physically present themselves and how they perceive body language displayed by various individuals or groups.
Equally important to engagement was the recognition and mitigation of barriers (e.g. linguistic, ethnic, or cultural) that impede communication, compounding an already sensitive and complex situation. For example, newcomer populations (i.e. immigrants and refugees) often experience increased complex care needs and higher healthcare inequities (Bergold & Thomas, 2012; Snow et al., 2018). These groups often experience greater barriers for inclusion in POR, which may further perpetuate negative health outcomes. As a result, community partners working with newcomer groups noted that they often leaned on other patient partners for guidance and support, particularly during engagement activities that were sensitive. Finally, those working with older adult and rural communities also recognized that technical support and access to appropriate technology (e.g., tablets and printers) may be necessary, especially where virtual activities were planned and offered.
Discussion
For the patient and community partners in this study, the experience of feeling valued was strongly grounded in effective communication, with factors such as the use of active listening, plain language, and open discussion around expectations and responsibilities being central to the experience of meaningful engagement. These emerging factors reflected a need for attention to power relations, the creation of safe spaces for collaboration, and active work to promote access, humility, and reflexivity for all team members. For example, while the importance of communicating in inclusive and plain language in POR has been recognized previously, it can mitigate barriers of knowledge exchange between partners that have diverse professional and knowledge backgrounds (Bergold & Thomas, 2012; Bishop et al., 2018; Borg et al., 2012). This is crucial, especially for individuals with limited proficiency in an official language, as well as those living with potentially stigmatizing conditions, where technical and clinical language can hinder inclusion (Collisson et al., 2011). As noted in a commentary by Tai-Seale and colleagues (2016), there is a need to ‘transform the mindset’ of where expertise lies. This includes recognizing the importance of shared or sensitive terminology, along with a need to create comfortable spaces whereby patient partners can contribute and raise concern. Further, active listening and effective communication across the spectrum of research activities emerged strongly in our research. These factors are corroborated by existing studies, including studies that emphasize the need for active listening to promote effective team functioning (Ministry of Supply and Services Canada, 1991; Shailes, 2017; van Diggele et al., 2020), significance of respecting confidentiality when working in partnership with patients (Smith et al., 2019), and need for active and mutual engagement that fosters relationships across the research process (Bird et al., 2020).
Analysis of the data also revealed the importance of recognizing expertise and contributions. Community and patient partners explained that they wanted to be treated as equal members of the research team, having their expertise and input incorporated into project development; they want to see how their input created tangible outputs of value to their community. Similar factors were reinforced in a recent scoping review by Bird and colleagues (2020) who reported that a key facilitator for patient partnerships was attempting to evenly distribute power differences at the beginning of a study and being consistent with all team members to offset this difference. Drawing on the work of Bauer (2014), we adopted intersectionality as a guide to unpack the power relations associated within POR. Our findings corroborate and extend the existing literature, drawing attention to how power relations are embedded in research processes that seek to engage diverse patient backgrounds and experiences. This adds a nuanced perspective from patients themselves, showcasing the need for conceptual and paradigm shifts that intentionally value diverse knowledge systems and partner contributions. Moreover, it reflects attention to researcher bias and the need for critical reflexivity in promoting equity in POR methods and knowledge translation (Straus et al., 2020).
Compensation is a multifaceted and complex issue in POR and is a factor that can contribute to patient partners feeling valued and respected. Within this research study, participants recognized the importance of monetary compensation, noting that other members of the research team are paid for their time, and the need for timely remuneration of expenses (e.g., childcare, parking, etc.). Participants expressed that a lack of monetary compensation left them feeling that their contributions and time were not truly valued. In this sense, compensation illustrated more than payment, it demonstrated a commitment to fostering equity and support for all team members. Previous literature has similarly outlined the impact of compensation on patient partners and highlighted the importance of monetary compensation, with a commitment to patient partners (Domecq et al., 2014; Richards et al., 2018, 2022). Further, Poitras and colleagues (2020) highlight the need to ‘normalize’ compensation in POR, ensuring agreement is reached at the onset of the work and that there is a clear distinction between compensation for contributions and expenses incurred through participation. Interestingly, there are several guidelines and policy documents in Canada and the United Kingdom that inform both financial and nonfinancial compensation with patient partners (Fox et al., 2024). Fox and colleagues (2024) concluded that implementation of these compensation guidelines needs to be further explored. Our study further emphasized the need for deliberate and thoughtful attention to compensation, noting that a failure to provide adequate and timely compensation and support partners for equity-deserving populations may impede participation and place an unfair burden on those already experiencing significant barriers. Continued exploration around compensation needs and implementation is warranted, particularly for populations that face barriers to engagement in research.
Building a relationship is important in the success of any team, however, POR with populations that experience barriers requires intentional planning and robust relational practices. Participants explained that brave and safe spaces of engagement formed a foundation for meaningful relationship building, including promoting mutuality, reciprocity, and trust, and helped sustain this over time. Relationship building and trust in partnered research has been widely addressed in the POR literature (de Wit et al., 2011; Sunderji et al., 2019; van der Velde et al., 2009; Zibrowski et al., 2021). In this research, participants identified factors that facilitated or challenged their engagement in POR, including describing how their own positionality, i.e., lived experience, ethnicity and research knowledge impacted the partnership process. Of note, many participants identified how their own social locations or the presuppositions of others around expertise impacted contributions. For example, among immigrant, newcomer, and refugee community partners, ethnocultural beliefs around research were entangled in experiences of political and social fear shaping research patient power relations (e.g., limiting what was shared during an interview if it may negatively impact family back in their home country). Likewise, for participants with lived or living experience of mental health conditions, their experience of stigmatizing language was seen to limit their participation and impede meaningful contributions to research. Further research is needed to better understand the factors that promote or challenge engagement in POR, including a need for robust evaluation (Aubin et al., 2019).
As a component of safe research spaces, participants also identified the need for trauma-informed and culturally sensitive research approaches. Participants explained that team members should be prepared to engage with people with diverse experiences, being accepting, mindful, and proactive. For many participants, this involved teams being aware of the potential harms associated with sharing their lived experience and fostering ways to mitigate risks and provide support. There has been growing attention to trauma-informed POR practices in the literature (Roche et al., 2020; Shimmin et al., 2017), along with the emergence of broader frameworks and research approaches that promote social justice and health equity in research, including the ‘Valuing All Voices Framework’ which emphasizes the need for trust, self-awareness, empathy, and relationship building (Roche et al., 2020). Further, a recent article by Gum and colleagues (2023) highlights the need for research teams to both facilitate safe spaces to promote optimal patient engagement and to formally recognize trauma-related experiences and insights and integrate this within their research. Engagement of those in boundary spanning roles can be valuable in some circumstances, especially where populations are facing extreme exclusions, marginalization, and disparities. This was mirrored by our team community partners, who highlighted that some populations are facing critical barriers and disparities, such as home and financially insecure populations, who may be focusing on surviving. Unless direct and tangible benefits arise immediately within the settings, engagement in research may result in direct harms. Continued investment in equity and trauma-informed POR resources, including those to support critical reflexivity, cultural humility, and trauma-informed practices, is urgently needed.
Recommendations
This research study has provided a deep exploration into POR with populations that face barriers to engagement in research, perspectives that are seldom heard. Key messages from the wider study are summarized in a range of infographics and resources (Banner et al., 2022a; 2022b; 2022c; 2022d; 2022e). Here, we have learned from patient and community partners that experience a range of overlapping barriers and social exclusions, examining factors that shape patient experiences in POR. These factors included effective communication, navigating mutuality and respect, compensation and recognition, relationship building, and trauma informed practices. While many of these factors reflect those described in the broader POR literature, we learned how these insights can be more nuanced when reflecting the diverse characteristics, identities, and contexts of those engaged and how common barriers can compound exclusion in POR. Researchers must be appropriately prepared to engage with diverse communities and well positioned to support meaningful partnerships and tangible impacts. Two main recommendations arose from this work: 1) Co-development of tools to support critical, reflexive, and equity-centered and trauma-informed practices, and 2) Co-creation and mobilization of anti-racist, equity-centered, and trauma-informed POR training programs.
In order to promote safe and trauma-informed relational practices in POR, research teams need to be well prepared and critically reflexive. Continued exploration of engagement practices among populations that face barriers is warranted and should continue to work to identify and promote best and promising practices. The creation and widespread mobilization of practical engagement and evaluation tools is needed. Tools should incorporate intersectionality (Kelly et al., 2021) and trauma-informed lens (Knowledge Translation Program, n. d.), while including actionable strategies that can assist teams to collectively navigate complex research and social spaces. In doing this, research teams must work together to continually examine, challenge, and evaluate their engagement practices.
Equity-centered, and trauma-informed POR training programs are needed. This is particularly important given the widespread drive among research funders to adopt equity, diversity, and inclusion within health research. A failure to adequately prepare research teams may give rise to harmful, tokenistic, and traumatic engagement spaces. Fulsome, intentional, and sustained engagement of diverse populations in the creation of training programs and infrastructure is warranted as a means of fostering inclusion and plurality, while avoiding the continued perpetuation of dominant voices and perspectives.
Limitations
While this study extends the existing literature and provides an in-depth analysis of the factors that shape engagement experiences in POR for people who experience multiple barriers, this study has some important limitations that must be considered. First, despite seeking to reach a diverse cohort of participants, the majority of participants were located in urban areas of British Columbia. Future studies should explicitly seek to engage community and patient partners from more diverse communities, including rural and remote areas, since this may yield new insights relevant to participation in POR teams. Secondly, as this research was focused specifically on British Columbia, future research that is broader in scope is warranted, including exploring experiences at a national and international level. Finally, while sex- and gender-based considerations were explored during analysis, this did not emerge strongly in the thematic analysis. However, greater diversity with respect to sex and gender in future studies would be beneficial.
Conclusion
Patient-oriented research is a valuable approach that fosters meaningful engagement of patients and community members to identify and respond to patient priorities and improve health outcomes (CIHR, 2019). POR is a valuable approach to the integration of diverse knowledge systems into health research, and an effective means of promoting diverse patient voices and experiences. To date, POR has been hailed as a mechanism to promote the creation and mobilization of relevant and responsive research that improves health system and patient outcomes, while reducing costs (Allin, 2008; Chalmers & Glasziou, 2009; Devine et al., 2013; Manafo et al., 2018). Despite many strengths, however, POR has been criticized for its failure to adequately engage patients with diverse experiences and perspectives (Bishop et al., 2018; Olson & Windish, 2010; Truog, 2012). Additionally, researchers and professional knowledge users hold significant power, and their views are typically privileged and valued over others.
By examining what makes POR participants feel valued in the process, this research contributes to advancing diversity within POR methods and provides strategies for engagement methods and practices for inclusivity of diverse patient partners and other community partners who experience barriers to engagement. In this paper, we examined the insights of patient partners, researchers and community not for profit groups to promote more inclusive POR in British Columbia, Canada. In doing this, we draw attention to what makes patient partners feel valued during the research process, highlighting the nuanced needs and values of patients and partners from diverse equity-deserving populations. Our findings suggest that greater attention to relational and reflexive practices, including acknowledging the explicit value of experiential knowledge and promoting structures to optimize inclusion of diverse patient partner perspectives and participation in POR, in order to support the meaningful inclusion of community and patient partners who face multiple barriers to engagement in POR. By doing this, we provide POR teams with insights to best support research co-production and shared decision-making with populations that face barriers to engagement in research.
Supplemental Material
Supplemental Material - My Opinion Matters Too! What Makes Patient Partners Feel Valued in Patient-Oriented Research? Learning From Research Partners who Experience Barriers to Engagement in Healthcare and Research
Supplemental Material for My Opinion Matters Too! What Makes Patient Partners Feel Valued in Patient-Oriented Research? Learning From Research Partners who Experience Barriers to Engagement in Healthcare and Research by Kiranpreet Ghag, Davina Banner, Barbara Croome, Daisy Au, Nancy Clark, Maryam Dehnadi, Shayna Dolan, Ursula Ellis, Jessica Froese, Joyce Griffith, Russell Maynard, Shannon Freeman and Susan Mills in International Journal of Qualitative Methods.
Footnotes
Acknowledgements
First, this research was undertaken across British Columbia, Canada. In doing so, we wish to express our gratitude to be guests and visitors on the unceded, traditional territories of many Indigenous Peoples, whose ancestors have inhabited these lands for countless generations. Second, we thank the British Columbia Support Unit and Canadian Institutes of Health Research who graciously funded this research. Finally, we would like to offer our sincere thanks to all of those that participated in this project. Your passion, time, and wisdom were inspirational.
Ethical Considerations
This research was approved by the BC harmonized research ethics board (#H19-01726-A001).
Consent to Participate
Participants were provided with a comprehensive information sheet and consent form and were asked to provide written or verbal consent to participate in this research study.
Consent for Publication
Informed consent for publication was provided by the participant to trained research associates.
Author Contributions
The study was co-led and conceptualized by DB, BC, NC, & SM. Data were collected by DB, BC, SD, NC, & SM and analyzed by DB, NC, SD, KG, JG, & JF. Manuscript preparation was conducted by DB and KG. All authors reviewed and contributed to edits of a draft of the manuscript. All authors have reviewed and approved the final manuscript and Kiranpreet Ghag and Davina Banner are considered joint first authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to acknowledge receipt of funding from the British Columbia SUPPORT Unit and Canadian Institutes of Health Research to conduct this research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is not available for secondary analysis or use due to the sensitive nature of the data. This is in congruence with our research ethics board approval and as discussed in the participant consent process.
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.