
Abstract
To investigate thoracoabdominal surface respiratory motion and monitor the corresponding displacement of external targets, a respiratory motion phantom driven by lead-screw stepper motors was developed to simulate physiologically relevant surface movements. A binocular vision-based monitoring system was designed to accurately track the motion of targets affixed to the phantom’s surface. The phantom replicates prescribed respiratory motion, while the monitoring system continuously records target positions and reconstructs their motion trajectories. Experimental results demonstrate that the average measurement error of the monitoring system is 1.5911%. Under a predefined respiratory pattern, the system measured a vertical displacement of 14.472 mm for the target, closely matching the reference amplitude of 14.665 mm, with a relative error of 1.3161%. The Pearson correlation coefficient between the measured and reference motion curves within a single cycle reached 0.9828. These findings confirm that the developed phantom can effectively reproduce thoracoabdominal surface respiratory motion, and the proposed monitoring system enables accurate tracking of target motion on the phantom’s surface.
Introduction
Cancer poses a significant threat to human health. Lung cancer is among the most common malignancies, characterized by high mortality rates, and most patients require radiotherapy. 1 However, thoracoabdominal tumors are often located near critical organs, and their motion is influenced by the patient’s respiration and other physiological activities. Thus, radiotherapy poses a potential risk to surrounding critical organs, and the precise localization and tracking of tumor targets continue to present significant challenges.2–4 Direct tracking of internal tumor motion during radiotherapy remains technically challenging. An alternative approach monitors the movement of an external surface target while simultaneously measuring internal tumor displacement. This allows the establishment of a correlation model between surface motion and tumor respiratory motion, enabling prediction of tumor movement and supporting more precise radiotherapy guidance.5,6 Respiratory motion phantoms provide a safe and controllable means of replicating human breathing and are therefore widely used for system validation and performance evaluation. In this study, we developed a thoracoabdominal phantom integrated with a motion generation and monitoring system to simulate respiratory-induced surface motion and quantitatively track target displacement.
Traditional respiratory motion phantoms simulate human breathing by driving organ inflation and deflation via pneumatic or hydraulic mechanisms, such as in the lungs. Neumann et al. developed an early anthropomorphic thorax phantom in which lung motion was generated using a manually operated air pump. 7 Although this approach offered structural simplicity, the resulting respiratory motion lacked precise controllability. To address this limitation, Nobnop et al. incorporated a respirator connected to an oxygen tank to actively drive lung inflation, enabling more controlled respiratory motion. 8 Court et al., 9 Perrin et al., 10 Abdollahi et al., 11 and Chrysanthou-Baustert et al. 12 introduced programmable pumping systems to regulate lung inflation and deflation. These systems significantly improved motion controllability and repeatability. Despite these advancements, most pneumatic and hydraulic phantoms focused primarily on lung volume changes and did not explicitly account for the biomechanical role of the diaphragm in physiological respiration. To better reproduce realistic breathing mechanics, Black et al., 13 Lee et al., 14 and Serban et al. 15 employed piston-driven mechanisms to induce water displacement within internal chambers, translating the reciprocating motion of a piston rod into lung deformation that more closely resembles natural respiratory behavior.
Although previous respiratory motion phantoms achieved a high degree of biomimetic realism, many were limited by insufficient motion accuracy and poor long-term repeatability. To address these limitations, several studies introduced motor-driven actuation for direct control of respiratory motion. Laidlaw et al., 16 Vogt et al., 17 Kashani et al., 18 and Chang et al. 19 employed electrically driven mechanisms to actuate lung deformation, resulting in improved motion accuracy compared with pneumatic or hydraulic systems. However, because these phantoms relied on compliant materials such as silicone to reproduce organ deformation, their long-term performance remained susceptible to material fatigue and aging effects. Other actuation strategies were also investigated. Naghibi et al. utilized a pneumatic brake to drive a moving platform, 20 achieving a lightweight design but at the cost of limited positioning accuracy. To further improve motion precision and repeatability, subsequent studies shifted toward simplified mechanical architectures in which rigid platforms are driven directly by motors. Within this framework, Nioutsikou et al. 21 and Nakayama et al. 22 simulated respiratory target motion via three-axis actuation, enabling complex motion trajectories, although the motion was confined to a single target point. Similarly, Ahmad et al. realized combined translational and rotational target motion by actuating a cylindrical rod with stepper and servo motors. 23
Beyond single-point motion, several groups extended motor-driven designs to simulate respiratory motion over larger anatomical regions. Gnanago et al. 24 developed a modular dynamic torso phantom capable of reproducing respiratory and cardiac motion, and validated its motion performance in a 3T MRI environment. Lempart et al. 25 and Park et al. 26 employed stepper-motor-driven platforms to simulate vertical planar respiratory displacement. Pallotta et al. 27 further decoupled internal and external motions by actuating the phantom’s components independently. These approaches successfully realized planar respiratory motion predominantly along a single axis. In contrast, Lustermans et al. 28 and Dunn et al. 29 employed multiple motors to combine anterior–posterior and superior–inferior motions, enabling two-dimensional planar respiratory motion simulation.
Despite substantial progress in motor-driven respiratory motion phantoms, several limitations remain. Most existing designs reproduce motion at a single target point or over a rigid planar surface, which prevents independent control across multiple thoracoabdominal regions. Consequently, regional differences in respiratory motion, such as the distinct contributions of thoracic and abdominal breathing, are not adequately represented. Many studies also rely on predefined motion inputs without an integrated measurement system to continuously monitor phantom motion. This limitation makes it difficult to verify whether the intended motion is accurately and repeatably reproduced. As a result, reported motion accuracy often reflects a combination of actuation performance and measurement uncertainty, rather than the intrinsic performance of the phantom. These limitations highlight the need for a respiratory motion phantom capable of multi-region motion control while providing quantitative, real-time verification of surface displacement.
To address the above challenges, this study proposes a respiratory motion phantom based on lead screw–driven stepper motors. The phantom is actuated by stepper motors controlled through an Arduino platform. Linear motion is transmitted to thoracoabdominal surface plates via lead screws and nuts. To achieve precise control of motion direction, custom motor mounts are fabricated using 3D printing. Each mount is set at a predefined angle. This configuration allows the direction of motor-driven displacement to be accurately determined by the geometric orientation of the mount. Different respiratory motion patterns can be generated by modifying the mounting angles of the stepper motors using interchangeable 3D-printed components. The motion stroke of each surface plate is adjusted through the motor rotation range. Moreover, multiple motors with distinct preset orientations allow simultaneous simulation of respiratory motion across several thoracoabdominal regions. This setup reproduces spatially distributed surface movement. Predefined respiratory motion profiles are achieved through coordinated motor actuation, ensuring consistent and repeatable surface displacement. In addition, a binocular distance measurement system is used for real-time monitoring of surface target motion. The system captures the vertical displacement of surface targets during respiratory motion and quantifies surface movement in the superior–inferior direction. To ensure reliable evaluation, the system’s performance is first assessed through dedicated accuracy experiments. It is then used to evaluate the fidelity of the phantom’s respiratory motion by comparing the measured target trajectories with the predefined motion profiles. Such a system can provide a controllable experimental platform for respiratory motion simulation, enabling quantitative evaluation and validation of motion management and image-guided radiotherapy techniques.
Compared with previously reported respiratory motion phantoms that typically simulate motion at a single point or along a single direction, the proposed system enables multi-region actuation across the thoracoabdominal surface and integrates an independent stereo vision–based monitoring system for quantitative motion evaluation. This design provides a compact and flexible platform for reproducing respiratory motion and assessing motion accuracy in radiotherapy-related research.
Methods and materials
The schematic diagram of the respiratory motion phantom and the integrated monitoring system is illustrated in Figure 1. The phantom simulates respiratory surface motion through plates driven by lead screw stepper motors. Compared with conventional respiratory phantom designs, this configuration offers improved motion accuracy and repeatability. Given the intrinsic positioning accuracy and repeatability of lead-screw stepper motors, the system was implemented using an open-loop control strategy, without incorporating feedback-based controller design. Respiratory motion is reproduced across multiple thoracoabdominal regions by independently driven surface plates. Its compact structure is achieved with lead screw stepper motors. To evaluate the simulated motion, surface target displacement is measured using a cost-effective binocular ranging method, which maintains adequate tracking accuracy while avoiding additional system complexity.
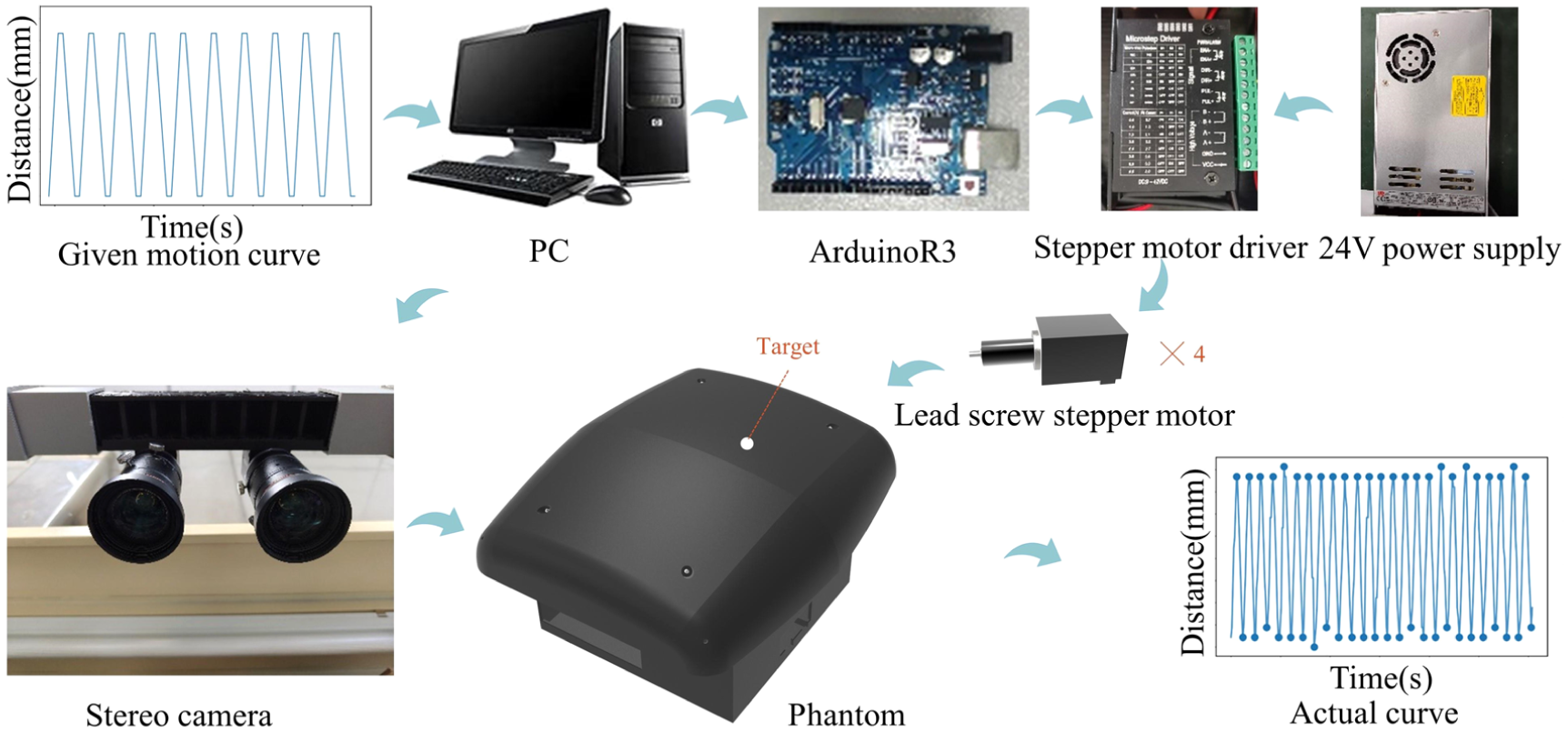
Schematic diagram of the phantom system and stereo vision-based respiratory motion tracking setup.
Design and implementation of the respiratory motion phantom
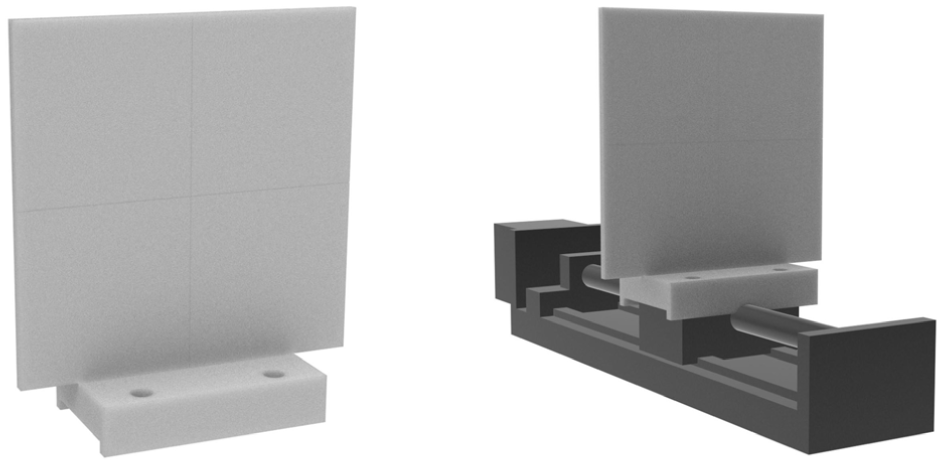
Figure 2 shows the respiratory motion phantom developed in this study. The phantom reproduces respiratory expansion and contraction by actuating surface plates using lead-screw–driven stepper motors. The stepper motors are controlled through a step–direction interface implemented on an Arduino R3 board, where the input pulse frequency determines the rotational speed of the motor and, consequently, the linear velocity of the lead-screw mechanism. The phantom is actuated using lead-screw stepper motors (model FG28NC45-5.08-25.4), which integrate a 28-series stepper motor with a lead screw. Each motor has a lead of 5.08 mm, a maximum linear travel of 25.4 mm, a holding torque of 0.12 Nm, and a rated phase current of 1 A. Motor actuation is implemented using TB6600 stepper motor drivers, which receive step and direction signals from the Arduino R3 control board. Pulse signals are generated by the Arduino through designated digital output pins. The pulse frequency determines the motor speed, while the total number of pulses defines the linear displacement of each surface plate, allowing the motion stroke to be precisely controlled. A custom control program is uploaded to the Arduino board to generate the required pulse sequences by switching the logic levels of the corresponding output pins. To more realistically represent surface motion during respiration, the thoracoabdominal region is subdivided into four sections, with a corresponding simulation plate fabricated for each section, as shown in Figure 2(a) and (c). Owing to the limited anatomical space of the thoracoabdominal region, four independent lead-screw stepper motors are used to actuate the surface plates. This design avoids the excessive structural enlargement commonly associated with conventional sliding platforms driven by stepper motors, thereby maintaining a compact and practical phantom configuration.
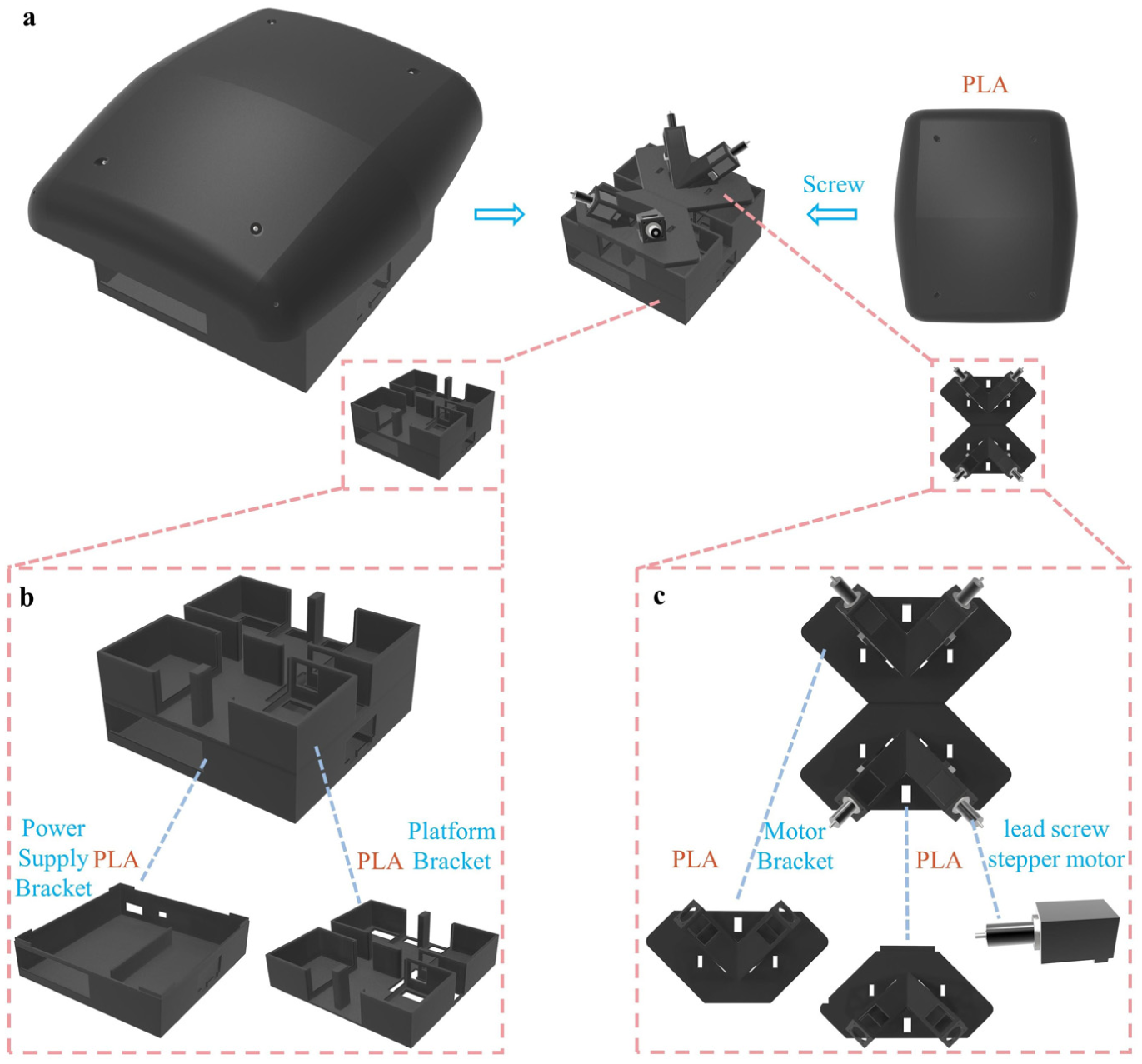
Structural design of the respiratory motion phantom. (a) The phantom is primarily constructed from PLA using 3D printing. The surface simulation plates are connected to the lead-screw stepper motors via threaded couplings. (b) The power supply and platform brackets, also fabricated from PLA, support the power module and Arduino driver, and provide structural positioning for the motor system. (c) The motor bases feature adjustable angles, achieved by altering the printed mount design, enabling directional control of motor travel.
A simplified breathing motion pattern was implemented, with all surface simulation plates expanding and contracting synchronously at equal amplitudes. This requires uniform displacement of each plate along the x, y, and z axes. As illustrated in Figure 3, the motor direction vectors from left to right and top to bottom are defined as
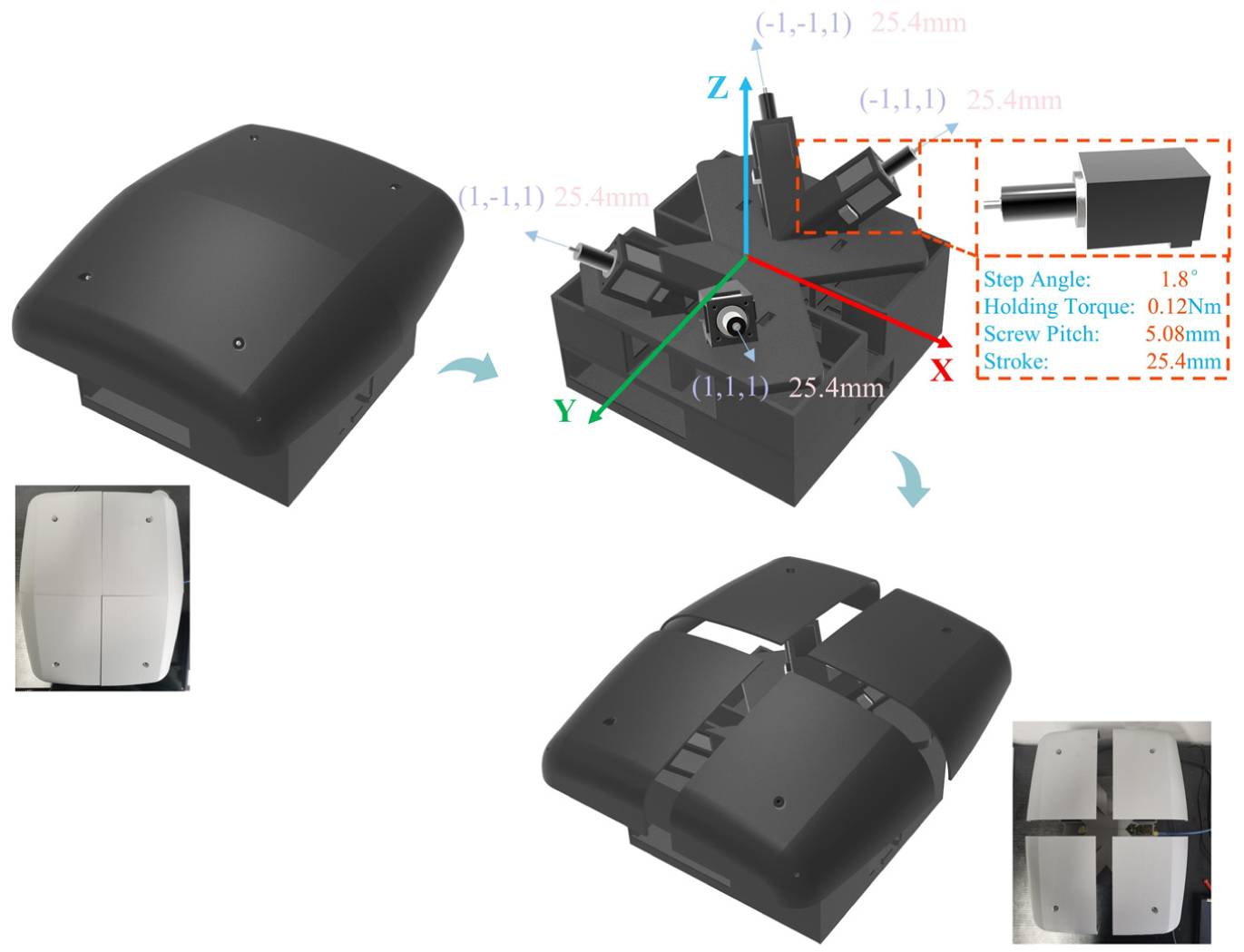
Motor rotation directions and operational states of the phantom during inhalation and exhalation.
Design and implementation of a target respiratory motion monitoring system
The target respiratory motion monitoring system relies on binocular ranging for spatial tracking. To enable 3D scene reconstruction, we used Zhang’s calibration method to estimate both the intrinsic and extrinsic parameters of the cameras and to determine their relative spatial positions. 30 The binocular system was built using two Hikvision MV-CS050-10UC industrial cameras, with the complete distance measurement setup costing approximately 6500 RMB (∼950 USD). For calibration, a black-and-white checkerboard with 8 × 6 corners and 15.5 mm square spacing was employed. A total of 20 stereo image pairs were captured, as illustrated in Figure 4.
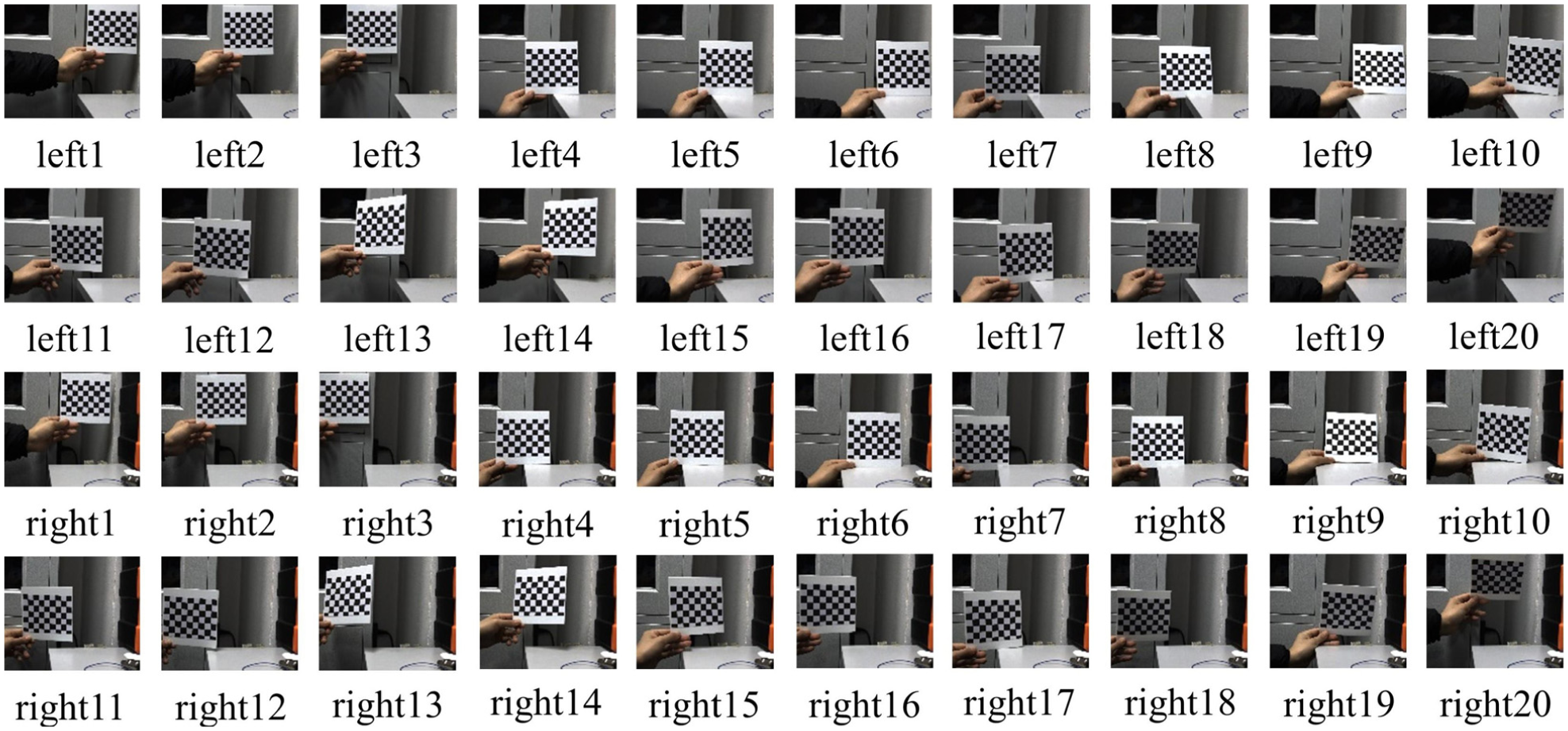
A total of 20 stereo image pairs captured by the left and right cameras were used for calibration of intrinsic and extrinsic parameters.
Stereo camera calibration was performed using a standard checkerboard-based method in Python. Intrinsic and extrinsic parameters were estimated using OpenCV calibration routines, and lens distortion was corrected using standard undistortion procedures. The calibration results, including intrinsic parameters and distortion coefficients, are summarized in Table 1. The stereo baseline B was 80.394 mm, and the mean reprojection error was 0.26 pixels.
Stereo camera calibration parameters.

After calibration, stereo images were preprocessed to enhance target detection. Both HSV-based filtering and binary thresholding were evaluated, and binary thresholding was selected due to its greater robustness under varying illumination conditions. Morphological operations were applied to improve segmentation accuracy, and target centers were extracted using minimum enclosing circle fitting Let the detected target centers in the left and right images be

With the optical center of the left camera defined as the origin of the 3D coordinate system, the spatial coordinates of the target point are given by


With the optical center of the right camera defined as the origin of the 3D coordinate system, the spatial coordinates of the target point are given by


When the midpoint between the optical centers of the left and right cameras is defined as the origin of the 3D coordinate system, the target coordinates can be expressed as either
Respiratory motion simulation and monitoring scheme
To simulate a regular respiratory cycle, a periodic motion pattern consisting of 5 s inhalation, 1 s pause, 5 s exhalation, and 1 s pause was implemented. The stepper motors were driven using a pulse–direction control strategy via an Arduino-based controller, enabling coordinated forward and reverse motion to reproduce the respiratory waveform. Forward motion was used to simulate inhalation, while reverse motion was used to simulate exhalation, maintaining consistent motion characteristics across cycles.
A 3D-printed PLA disc measuring 3 mm in diameter and 1 mm in thickness was used as a surface marker for motion tracking. After placement on the simulation plate, the phantom was aligned beneath the monitoring system for respiratory tracking experiments. Figure 5 shows the process of stereo image acquisition and processing. During operation, both cameras captured real-time images, which were then filtered and analyzed to extract the target’s center coordinates. Based on the disparity between the two views, the depth of the target was calculated. Successive depth measurements enabled reconstruction of the target’s displacement along the Z axis (posterior–anterior). Combined with measurements along the X (lateral) and Y (cranio–caudal) axes, the system provides full 3D monitoring of respiratory-induced target motion.
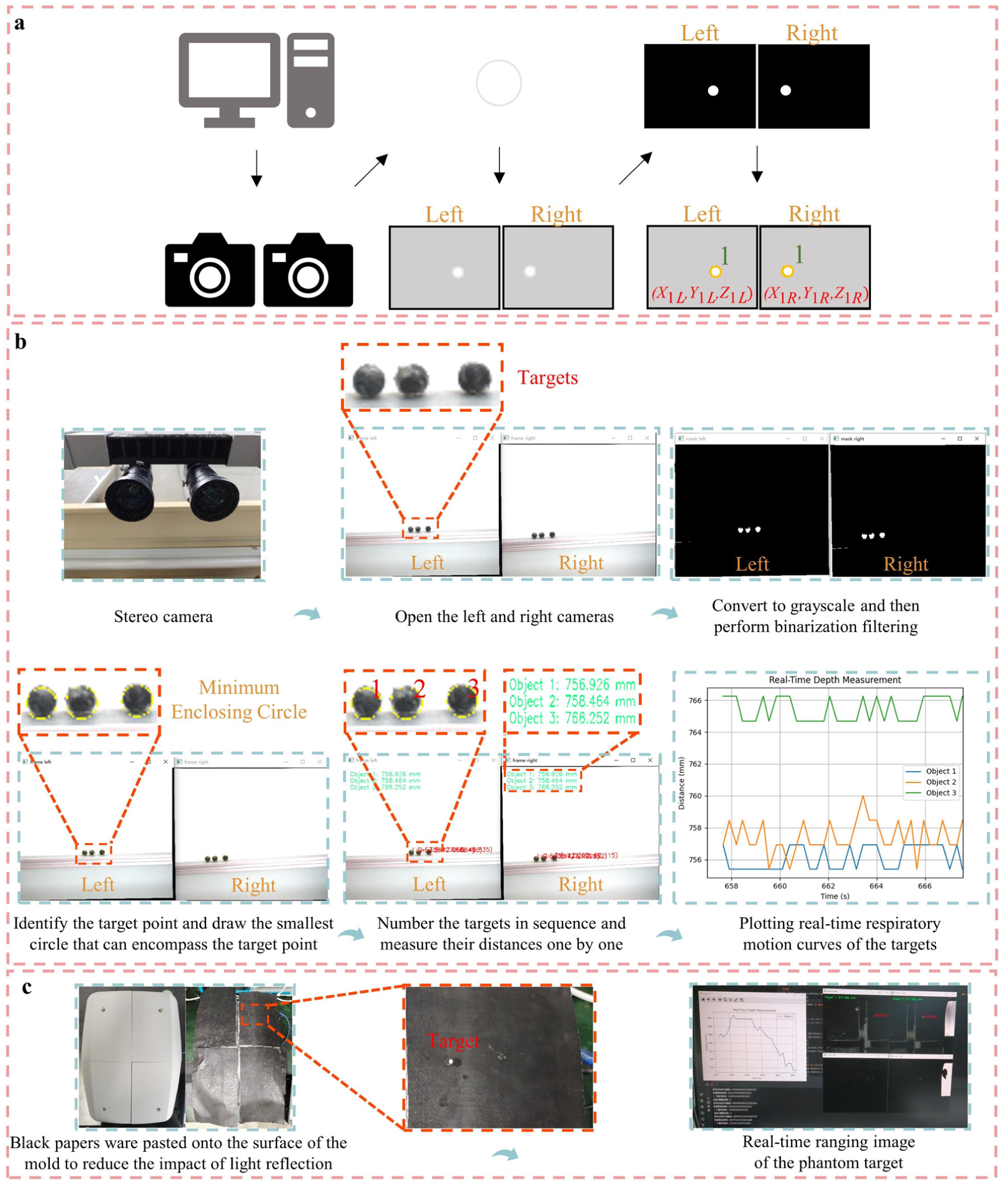
Workflow of the stereo vision-based system for tracking target respiratory motion: (a) image acquisition and processing solution, (b) actual image processing steps and ranging result, and (c) range measurement demonstration of phantom target.
Experimental section
Measurement accuracy experiment of the target respiratory motion monitoring system
To evaluate the measurement accuracy of the system, an experiment was conducted to test the respiratory motion tracking performance for surface targets. As shown in Figure 6, a test platform was mounted on a lead screw linear stage driven by a stepper motor, with a circular target fixed at its center. The amplitude of the platform’s movement was configured to 50 mm, with an actual displacement of 49.6 mm. The programed motion pattern included a 4-s uniform forward motion, a 0.5-s dwell, a 4-s return, and another 0.5-s dwell at the initial position. The motion data obtained from the tracking system were compared with the reference trajectory to assess measurement accuracy. Due to computational load and hardware performance limitations of the host computer, the effective data acquisition rate of the stereo vision system was relatively low and not strictly constant. During the measurement accuracy experiment of the monitoring system, the average sampling interval was approximately 0.3 s. For the respiratory motion simulation experiment of the phantom, the sampling interval increased to approximately 0.6 s after switching to a lower-performance laptop.
Stepper-motor-driven lead screw stage and test platform.
Respiratory motion simulation experiment of the phantom
The target respiratory motion monitoring system was used to evaluate the phantom’s performance in simulating respiratory motion. To ensure stable and reliable data acquisition under the limited and non-uniform sampling rate of the stereo vision system, short dwell periods were introduced at the extreme positions of the phantom motion. Specifically, a pause duration of 1 s was applied at the end of both inhalation and exhalation phases. This design allowed sufficient time for image acquisition and processing, thereby improving the robustness of displacement measurement at the motion endpoints. The stroke length of
Result
Experimental results of the target respiratory motion monitoring system accuracy experiment
As illustrated in Figure 7(a), the monitoring system successfully captured the periodic displacement of the target over 20 consecutive motion cycles. The measured trajectories exhibited consistent periodicity and stability, indicating reliable real-time tracking performance. A comparison between the measured and reference trajectories within a single cycle is presented in Figure 7(b). The two curves show strong agreement in both amplitude and temporal characteristics. Quantitative error analysis results are summarized in Figure 7(c). The mean relative measurement error across all cycles was 1.5911%, and the mean squared error (MSE) was 0.6259 mm2. In addition, the Pearson correlation coefficient between the measured and reference trajectories reached 0.9984, demonstrating an excellent linear correlation. These results indicate that the stereo vision-based monitoring system provides sufficient accuracy and repeatability for respiratory motion tracking applications.
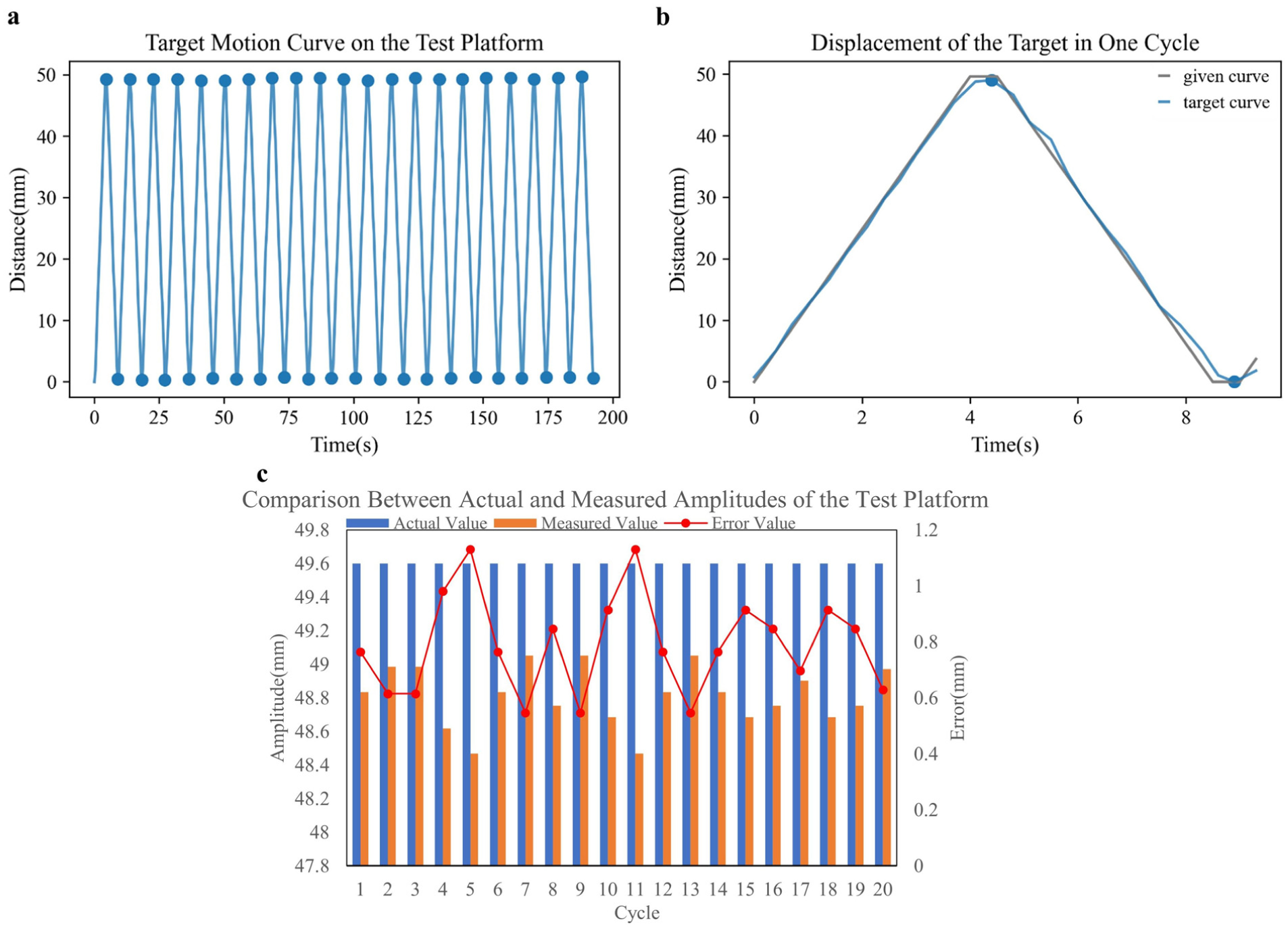
Accuracy evaluation of the respiratory motion tracking system: (a) target trajectory measured by the stereo vision system, (b) comparison between the measured and reference trajectories within one cycle, and (c) quantitative assessment of tracking accuracy.
Results of the respiratory motion simulation experiment of the phantom
The respiratory motion simulation capability of the developed phantom was evaluated using the same stereo vision-based monitoring system. Each lead-screw stepper motor had a stroke length of 25.4 mm, corresponding to a theoretical vertical displacement of 14.665 mm based on the geometric configuration of the motor mounting angles. The phantom was programed to execute a predefined respiratory cycle consisting of inhalation, pause, exhalation, and pause phases. Figure 8(a) shows the tracked vertical displacement of the surface target over 25 consecutive respiratory cycles. The measured displacement curves exhibit stable periodic behavior, closely matching the predefined respiratory pattern. A comparison between the measured and reference trajectories within a single cycle is shown in Figure 8(b), where the overall waveform and phase alignment are well preserved. The quantitative evaluation results are presented in Figure 8(c). The average measured vertical displacement was 14.472 mm, slightly lower than the reference value of 14.665 mm, corresponding to a relative error of 1.3161%. The MSE of the displacement was 0.3597 mm2, and the Pearson correlation coefficient between the measured and reference trajectories reached 0.9828. The maximum absolute error across all measurements was 1.077 mm. These results demonstrate that the phantom can accurately reproduce the intended respiratory motion with good repeatability and consistency.
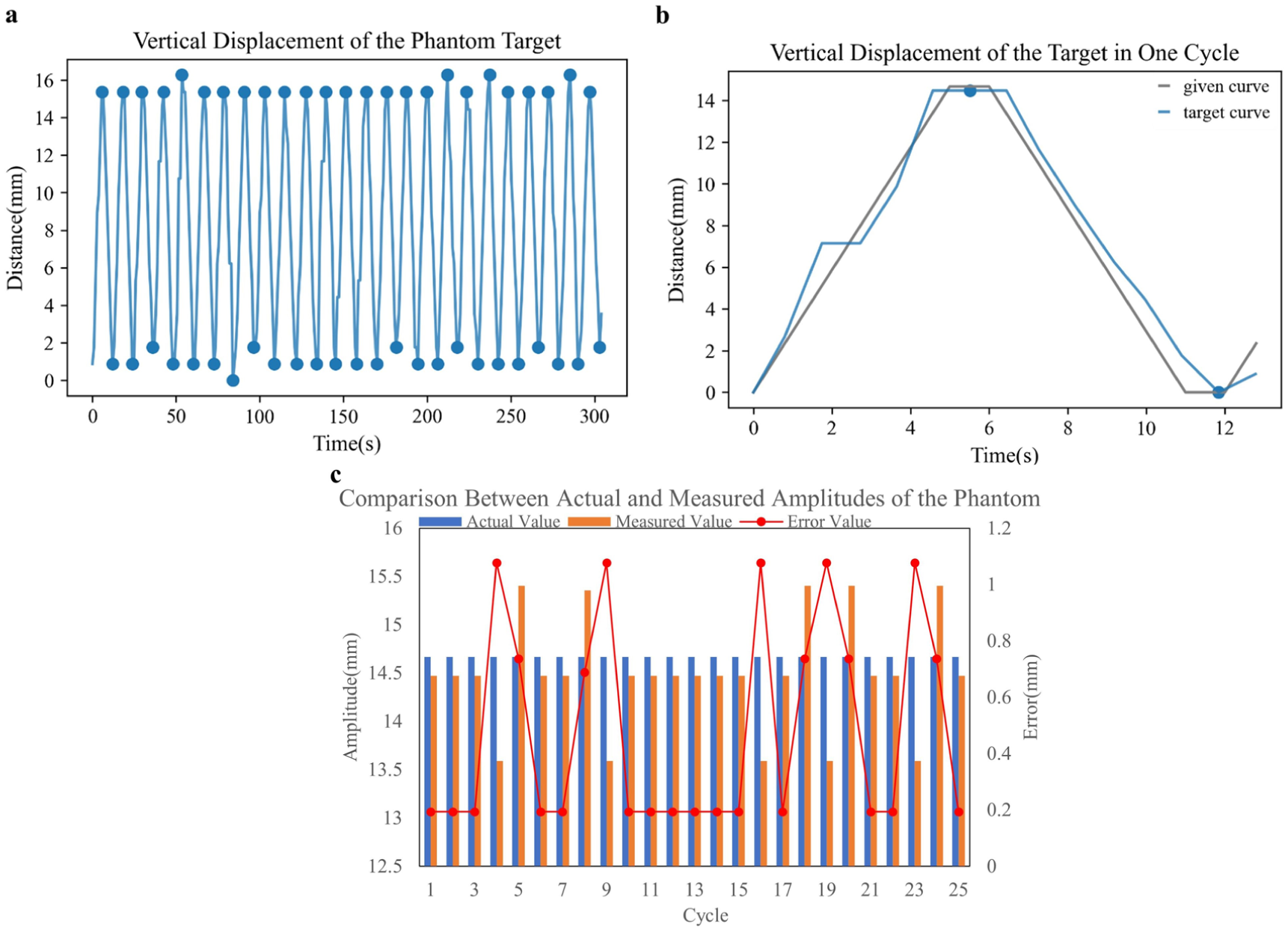
Evaluation of the phantom’s respiratory motion simulation: (a) tracked motion trajectory of the phantom measured using stereo vision, (b) comparison between the measured and reference curves within a single cycle, and (c) summary of simulation accuracy results.
Discussion and conclusion
In this study, a respiratory motion phantom driven by lead-screw stepper motors was developed and experimentally validated using an independent stereo vision–based monitoring system. The results demonstrate that the proposed phantom can accurately reproduce prescribed respiratory motion, while the monitoring system provides reliable displacement measurements for performance evaluation. To address the limited temporal resolution of the measurement system, short dwell periods were introduced at the end positions. Specifically, the phantom was held for approximately 1 s at each extremum, allowing multiple samples to be acquired under nearly constant displacement. This approach reduces sampling jitter in amplitude estimation and improves measurement stability, which is particularly beneficial for respiratory motion where displacement changes smoothly and becomes quasi-static near turning points.
For the stereo vision–based monitoring system, the mean relative error was 1.5911%, with a Pearson correlation coefficient exceeding 0.99. Although stereo vision can theoretically achieve sub-millimeter accuracy, practical factors such as baseline length, centroid extraction errors, residual lens distortion, and target size introduce unavoidable measurement uncertainty. A compact baseline of 80.394 mm was adopted to reduce system footprint, representing a trade-off between structural compactness and depth resolution. The system was used to track vertical respiratory motion of surface markers on the phantom and to generate corresponding displacement–time curves. Despite these limitations, the achieved accuracy is sufficient for respiratory motion monitoring, where displacement typically ranges from millimeters to centimeters.
The relatively low sampling rate of the stereo vision system (0.3–0.6 s per frame) is primarily due to the computational cost of stereo image rectification and processing. The high-resolution images used in this study (2448 × 2048 pixels per camera) require pixel-wise remapping and interpolation during rectification, which is computationally demanding on a CPU. As a result, the frame rate is limited by processing speed. Nevertheless, for respiratory motion simulation, where displacement varies smoothly over several-second breathing cycles, this sampling rate is sufficient to capture the overall motion trend.
The respiratory motion phantom exhibited a mean displacement error of 1.3161%, indicating accurate and repeatable performance of the lead-screw–driven stepper motor mechanism. Compared with pneumatic or hydraulic phantoms, which are prone to nonlinear deformation and long-term drift, the rigid mechanical transmission used here provides stable and reproducible motion profiles. The observed underestimation of displacement can be attributed to multiple factors, including limited fabrication precision of the 3D-printed motor mounts, which may lead to slight deviations in installation angles, as well as minor alignment errors in the assembly. In addition, the stereo vision–based measurement system introduces an inherent uncertainty of approximately 1.5911%, which contributes to the overall discrepancy. To address the apparent inconsistency between the measurement system uncertainty and the reported phantom displacement error, an independent ground-truth verification was introduced using digital calipers. The caliper-based measurements verified that the motor-driven linear stroke was 25.4 mm within the resolution of the instrument, with no detectable deviation. Therefore, the reference displacement used in this study is defined based on ground-truth mechanical and geometric constraints, rather than being derived from the stereo vision system. The monitoring system is used to assess the agreement between the reproduced motion and the predefined trajectory, rather than to establish absolute accuracy beyond its intrinsic uncertainty (1.5911%). Accordingly, the reported displacement error of 1.3161% should be interpreted as the deviation between the phantom’s realized motion and the ground-truth-defined reference trajectory, as observed through the measurement system, rather than as a direct indication of measurement precision exceeding the system’s uncertainty.
Compared with existing motor-driven respiratory phantoms, which typically reproduce motion at a single point or within a single plane, the proposed system enables multi-region actuation across the thoracoabdominal surface. By independently controlling each motor’s orientation and driving parameters, a variety of respiratory motion patterns can be generated. Although the present experiments primarily focused on synchronous motion with identical amplitudes, the system architecture also enables asynchronous and region-specific respiratory motion. To illustrate this functionality, additional experiments were conducted in which the thoracic and abdominal regions were driven with different displacement amplitudes, resulting in larger motion in the thoracic region and smaller motion in the abdominal region, consistent with general respiratory mechanics. The corresponding experimental demonstrations are presented in Supplemental Figure S6. Furthermore, regional phase differences were introduced by applying a start delay between motor groups. In this configuration, the thoracic plates lagged behind the abdominal plates by 0.5 s, enabling asynchronous respiratory motion (Supplemental Figure S7). Amplitude modulation is achieved by adjusting the rotation range or speed of each motor, while phase shifts are implemented through controlled activation timing. Although the experimental data do not provide a full quantitative validation, they demonstrate the system’s capability to reproduce differential amplitudes and phase delays within physiologically relevant ranges. These specific experiments were conducted primarily to demonstrate the system’s unique capability for asynchronous, multi-region motion control. As there is currently no established “gold standard” reference for asynchronous thoracoabdominal surface motion, these results are presented as qualitative demonstrations of system flexibility and functional versatility. The proposed system allows independent motion profiles to be assigned to each region, enabling the simulation of heterogeneous breathing patterns such as thoracic- and abdominal-dominant respiration.
From a systems engineering perspective, the proposed respiratory motion phantom can be regarded as a simplified biomedical robotic platform, integrating actuation (stepper motor–lead screw mechanisms), sensing (stereo vision–based tracking), and trajectory execution (predefined respiratory motion profiles) within a closed-loop framework analogous to robotic systems used in medical applications. Although based on a low-degree-of-freedom linear actuation architecture, the proposed control and monitoring strategy is scalable to more complex kinematic systems, such as high-degree-of-freedom parallel31,32 or hybrid robotic structures, 33 where kinematic coupling, singularities, and multi-actuator error propagation become critical considerations. In such cases, independent external monitoring, as implemented via stereo vision in this study, provides an additional layer of validation for motion transparency and system safety. Furthermore, 3D-printed components introduce inherent manufacturing tolerances and material-dependent uncertainties, which are typical in low-cost biomedical robotic systems and may affect absolute accuracy while preserving motion repeatability.34,35 These considerations align with established validation frameworks for additive-manufactured medical devices and patient-specific assistive systems, where engineering tolerances are explicitly incorporated. Overall, the proposed system bridges respiratory motion phantoms and biomedical robotics, providing a scalable platform for motion simulation, system validation, and radiotherapy-related algorithm testing.
In conclusion, a reconfigurable multi-plate respiratory motion phantom integrated with a stereo vision–based monitoring system was developed for quantitative evaluation of thoracoabdominal motion. The proposed system achieves a mean displacement error of 1.3161% (phantom motion fidelity relative to ground-truth reference), while the stereo vision monitoring system exhibits a measurement error of 1.5911%, demonstrating high consistency between the generated motion and the measured trajectories. These quantitative results validate the reliability of both the actuation system and the vision-based monitoring framework for respiratory motion reproduction and assessment. Beyond performance validation, the key contribution of this study lies in enabling independently controllable multi-region respiratory motion, which extends conventional single-point or single-plane phantoms to a more physiologically representative thoracoabdominal model. This capability provides a practical and scalable platform for simulating heterogeneous breathing patterns, which is of direct relevance to motion management strategies in radiotherapy. From a broader perspective, the proposed system establishes a bridge between respiratory motion phantoms and biomedical robotics by integrating actuation, sensing, and trajectory control within a unified framework. This offers both theoretical significance in terms of system-level design of biomedical robotic simulators and practical significance for the validation of motion tracking and image-guided radiotherapy algorithms. We acknowledge that the use of rigid plates introduces edge discontinuities and does not fully reproduce soft-tissue deformation. In future work, a thin compliant layer will be introduced to better replicate surface motion without compromising motor stroke. Efforts will also focus on improving measurement accuracy and extending the system to more complex, patient-specific respiratory patterns. In addition, the monitoring system may be applied to record respiratory motion from different subjects, which can then be reproduced by the phantom for systematic evaluation of realistic breathing behavior.
Supplemental Material
sj-docx-1-ade-10.1177_16878132261461109 – Supplemental material for A reconfigurable multi-plate respiratory motion phantom with integrated stereo-vision verification
Supplemental material, sj-docx-1-ade-10.1177_16878132261461109 for A reconfigurable multi-plate respiratory motion phantom with integrated stereo-vision verification by Can Wang, Jie Wang, Yuwen Wu, Yuze Zhang, Mostafa Orban, Mahmoud Elsamanty and Kai Guo in Advances in Mechanical Engineering
Supplemental Material
sj-zip-1-ade-10.1177_16878132261461109 – Supplemental material for A reconfigurable multi-plate respiratory motion phantom with integrated stereo-vision verification
Supplemental material, sj-zip-1-ade-10.1177_16878132261461109 for A reconfigurable multi-plate respiratory motion phantom with integrated stereo-vision verification by Can Wang, Jie Wang, Yuwen Wu, Yuze Zhang, Mostafa Orban, Mahmoud Elsamanty and Kai Guo in Advances in Mechanical Engineering
Supplemental Material
Footnotes
Handling Editor: Aarthy Esakkiappan
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Key R&D Program of China (2023YFB4706200), Chinese Academy of Sciences International Talent Plan (PIFI) Project (2024VBB0010), the pilot projects for fundamental research in Suzhou (SSD2023014), Science and Technology Development Plan Project of Jilin Province (20240305049YY), Natural Science Foundation Project of Shandong Province (ZR2022QH214), and Natural Science Foundation Project of Chongqing (2024NSCQ-MSX0007), Project of the State Administration of Foreign Experts Affairs (H20240225).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.