
Abstract
Vertebral arterial disease (VAD) is a less commonly recognized and treated source of cerebrovascular ischemia compared with carotid artery disease. Patients are often referred for treatment after they have developed symptoms in the form of transient ischemic attacks or had a posterior hemispheric stroke. Traditional treatment of VAD has been surgical. More recently, endovascular treatment of VAD has been utilized. We performed a retrospective review of our institutional experience in treating VAD from 2001 to 2010. For treatment of proximal VAD, perioperative morbidity is lower for the endovascular group than for the surgical group, but six-week mortality was higher for the endovascular group. Complete resolution of symptoms occurred more frequently with surgery than with endovascular therapy. Therefore surgical reconstruction appears to be preferable to angioplasty and stenting for treatment of proximal vertebral artery occlusive disease.
Introduction
Although less commonly recognized as a source of cerebrovascular pathology, vertebral-basilar occlusive disease can be a significant cause of morbidity and mortality. 1 Atherosclerosis of the vertebral artery has been shown to be present in 25–40% of individuals with cerebrovascular disease.1–3 The proximal segment of the vertebral artery is the most commonly involved by atherosclerotic disease. 4 Lesions of the proximal vertebral artery can account for up to 30% of patients presenting with transient ischemic attack (TIA) or stroke 5 but historically only 5–8% of surgeries performed for cerebrovascular disease address these lesions.5,6
Surgical treatment of proximal vertebral arterial disease was first described over 50 years ago 7 and has been the standard treatment for these lesions. Surgical endarterectomy and angioplasty of the vertebral artery origin and subclavian artery were the first used to treat these lesions.7–9 More recently bypass and arterial transposition via extra-thoracic approach have become more popular. Vertebral artery to common carotid artery transposition has become the most commonly reported surgery to address lesions of the proximal vertebral artery causing vertebro-basilar symptoms, TIA or stroke. Surgical reconstruction of the proximal extracranial vertebral artery is relatively safe with morbidity and mortality comparable with that of carotid endarterectomy.6,10,11
Percutaneous balloon angioplasty of the vertebral artery was first successfully performed in 1981. 12 Since then, interest in treating proximal vertebral artery disease (VAD) with endovascular methods has increased markedly. Although numerous studies have shown technical success treating these lesions,4,13–17 these case series have been relatively small, re-stenosis rates have been as high as 40–50% 3 and follow up has typically been brief. Despite the increasing use of endovascular therapy for proximal vertebral artery occlusive disease, there have not been any reported studies directly comparing these two treatment modalities with regard to proximal vertebral artery lesions. We reviewed our institutional experience over the past 10 years in treating lesions of the proximal vertebral artery in order to better define their uses and outcomes.
Methods
Institutional Review Board approval was obtained prior to the study. A retrospective identification of patients treated surgically was made by the use of CPT billing codes for the vertebral to carotid artery transposition which is the standard procedure at our institution for surgical re-vascularization of the proximal or V1 segment of the vertebral artery. Patients having vertebral artery angioplasty are routinely referred to the neuroradiology department at our institution. This department has an active database which was accessed for identification of patients having a vertebral artery intervention. All of these patients then had their hospital and office records reviewed for pertinent data. Patients were contacted during the study and offered a free neurovascular exam and surveillance duplex ultrasound of their vertebral artery transposition. If the patient would not come in for an exam and ultrasound then they were queried about the status of their symptoms. Patients whom we could not contact were then searched for in the Social Security Administration database to identify those who had expired. Patients with a non-atherosclerotic etiology for their vertebral artery pathology were subsequently excluded. After tabulating the results, comparisons for categorical variables were made using the χ2 (Chi-Square) or the Fisher exact test where appropriate. Analysis of variance was used to compare the groups. Survival and patency were calculated using lifetable analysis.
Results
Patient demographics
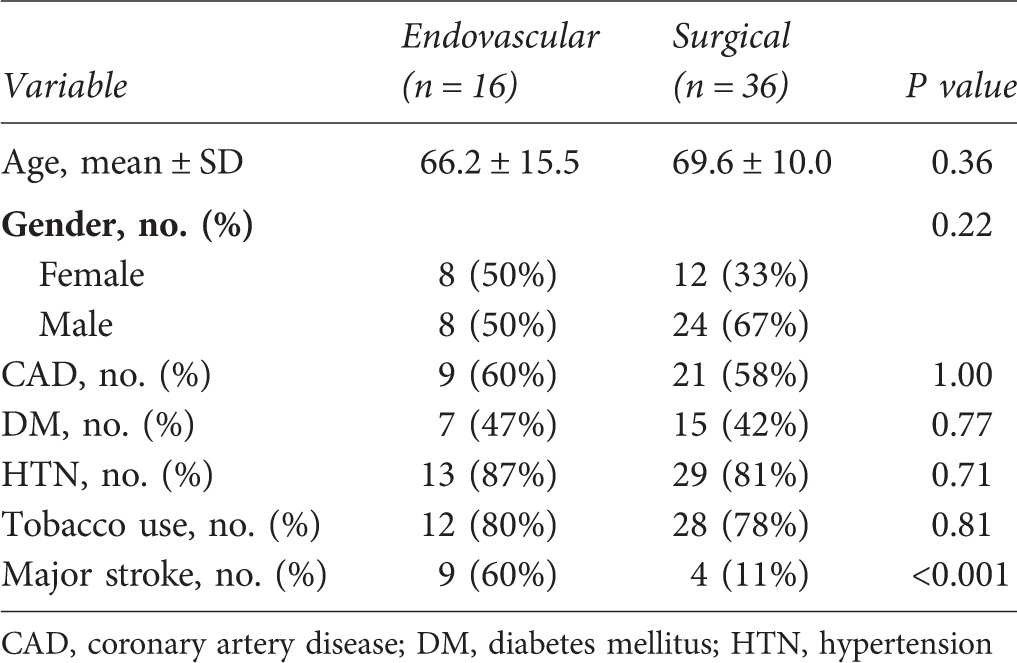
CAD, coronary artery disease; DM, diabetes mellitus; HTN, hypertension
Surgical group
In the surgical group all of the patients were symptomatic. Three patients had a posterior CVA as their presenting symptom. The remaining patients had the following vertebro-basilar symptoms: ataxia (n = 20), syncope or near syncope (n = 7), visual changes (n = 8) and dizziness (n = 7). Multiple symptoms were present in 20 patients and 16 patients had a single complaint. Three patients had a history of anterior circulation stroke. The preoperative arteriograms demonstrated greater than 50% stenosis in the treated vessel in all of the patients and greater than 70% stenosis in 33 patients. No patient had surgery for an occluded proximal vertebral artery. With regard to the three patients with lesions in the 50–60% range, one had a simultaneous subclavian artery aneurysm repair and was having posterior circulation TIAs. In another, the contralateral vertebral artery ended in the posterior inferior cerebellar artery (PICA) and in the last patient there was concomitant severe disease in the P1 segment of the posterior cerebral artery.
The vertebral artery contralateral to the treated vessel was severely diseased or occluded in 14 and was hypoplastic, aplastic or ended in the PICA in 11 patients. It was normal without disease in 11 patients. In this latter group of patients, the treated vertebral artery was the dominant artery in 10 and in the other there was an ulcerated lesion in the setting of a cerebellar stroke. Eighteen patients also had severe carotid artery occlusive disease. Two patients had previously undergone carotid endarterectomy (CEA) and one had previously been treated with carotid artery stenting (CAS). Seven patients were noted to have significant intracranial occlusive disease.
Thirty-four patients underwent vertebral artery to common carotid artery transposition. The left side was treated in 27 patients and the right side was operated on in the remaining nine patients. Five patients had a simultaneous vertebral artery transposition in combination with ipsilateral carotid endarterectomy, and one had a subclavian artery aneurysm repair. One patient who had a carotid endarterectomy also underwent external to internal carotid artery bypass four months after his initial procedure.
In our surgical patients, perioperative morbidity and six week mortality were 6 and 3% respectively. The one death occurred secondary to postoperative myocardial infarction. The other major morbidity was a bleeding complication, which required re-exploration. The median length of stay was 2.0 days (range 1–5 days).
Postoperatively in the surgical group, 31 (86%) patients reported complete relief of their symptoms, two (5.6%) reported partial relief and three (8.6%) had no relief. The three patients who were treated for stroke had no recurrent stroke or symptoms following surgery. The partially improved patients were treated for dizziness (which improved after a pacemaker was placed) and near syncope (which decreased from 3 times a day to one). The unimproved patients were treated for ataxia (2 patients) and dizziness (which resolved after pacemaker implantation). In the 11 patients who had isolated VAD and a non-diseased contralateral vertebral artery, the treated artery was the dominant vessel in all of the cases. These patients all complained of ataxia or dizziness and all were completely improved following surgery. In the subgroup of 11 patients treated for unilateral VAD with a normal contralateral vertebral artery, 10 of these involved the dominant vertebral artery and the surgery was performed for symptoms of vertebro-basilar insufficiency (VBI). In the other patient, the stenosis was ulcerated and had led to a cerebellar CVA. All of these patients were cured of their symptoms after surgery.
Of the 36 patients in the surgical group, 25 were alive at the time of this review. The average post surgery survival was 56.5 months. Of the 25 living patients, seven had current follow-up imaging (within the last year). Eleven patients were contacted and nine declined further follow up while two agreed to come in for a follow-up check but did not show up for their appointment. Seven patients were lost to follow up. Follow-up imaging was nonetheless available in 22 patients and ranged from two to 103 months with a mean follow up of 32.6 months. All 22 patients had patency of their transposition demonstrated. Nineteen patients had ultrasound studies that showed patency with antegrade flow. One patient had a computed tomographic angiography (CTA) demonstrating patency. Two patients had magnetic resonance angiography studies demonstrating patency. One patient later required an extracranial to intracranial (ECIC) bypass for severely symptomatic anterior and intracranial artery occlusive disease.
Endovascular group
Fifteen of the patients in the endovascular group were symptomatic with proximal vertebral artery lesions. The remaining patient was asymptomatic and was treated prophylactically prior to coronary bypass secondary to bilateral occlusion of her internal carotid arteries and a hypoplastic contralateral vertebral artery. Nine patients were treated in the setting of an acute posterior circulation CVA. The remaining patients were treated for symptoms of syncope (n = 2), dizziness (n = 2), ataxia (n = 2) and visual changes (n = 1). Three patients complained of multiple symptoms. The pretreatment arteriograms demonstrated stenosis in the treated vessel of greater than 60% in all of the patients, greater than 70% in 15 patients and greater than 80% in 12 patients. The contralateral vertebral artery was severely diseased or occluded in 12 patients, hypoplastic in one patient and normal without disease in two patients. These last two patients were treated for severe unilateral stenosis which led to a cerebellar infarct in one and medically refractory vertebro-basilar symptoms in the other. Seven patients had significant carotid artery occlusive disease and 5 were noted to have significant intracranial occlusive disease.
The left vertebral artery was treated endovascularly in 10 and the right was addressed in six patients. No patient had bilateral angioplasty. Eight patients had primary angioplasty as their only treatment and eight patients were stented. Five of the stent procedures were primary and by intention. In two cases, stenting was done to treat a suboptimal result secondary to dissection. One patient had been previously treated with angioplasty alone before the study period and presented with a symptomatic recurrent stenosis, which was stented. Two patients were treated in the setting of an acute stroke secondary VAD and secondary basilar artery thrombosis. Both of these patients also had adjunctive percutaneous mechanical thrombectomy and thrombolysis. The procedures were performed over 0.014 guidewire and usually through a 5 French guiding sheath. Balloon sizes ranged from 3 to 4 mm in diameter and 9 to 24 mm in length. Stents ranged from 3 to 5 mm in diameter and 9 to 24 mm in length. The stents were all balloon expandable coronary stents. Embolic protection devices (EPDs) were not employed except in one case. One patient later had a second procedure. He had developed a high grade re-stenosis four months after his initial angioplasty, which was treated with a single stent.
In the endovascular group, the periprocedure morbidity was 6% and the six-week mortality was 12%. The technical success rate was 100% and the median length of stay was 1.5 days (range 1–40 days). One patient developed unstable angina which resolved with appropriate therapy and two patients in the endovascular group died within six weeks for a mortality rate of 12%. Their causes of death were pneumonia in one and the other one died from a combination of his stroke and congestive heart failure.
Of the 16 patients in the endovascular group, 15 were identified as symptomatic with proximal vertebral artery lesions. Of the 15 patients, nine presented for treatment after a major stroke. The other patients presented with symptoms of vertebro-basilar insufficiency (VBI). Four patients had complete relief of symptoms (27%). Eight had partial improvement (53%) and three had no relief (20%). In the subset of patients presenting with an acute stroke, three had complete relief, four had partial improvement and two were unchanged. In the subset of endovascular patients not presenting with an acute stroke, only one was cured, four were improved and one was unchanged. Thirteen patients had occlusion or severe disease of the contralateral vertebral artery and it was hypoplastic in another. Two patients had treatment of a vertebral artery lesion opposite a non-diseased artery for symptoms of VBI. One was completely improved and the other was not improved. Comparative analysis of the surgical and endovascular groups did show a statistically significant (P < 0.001) difference in relief of symptoms favoring surgery.
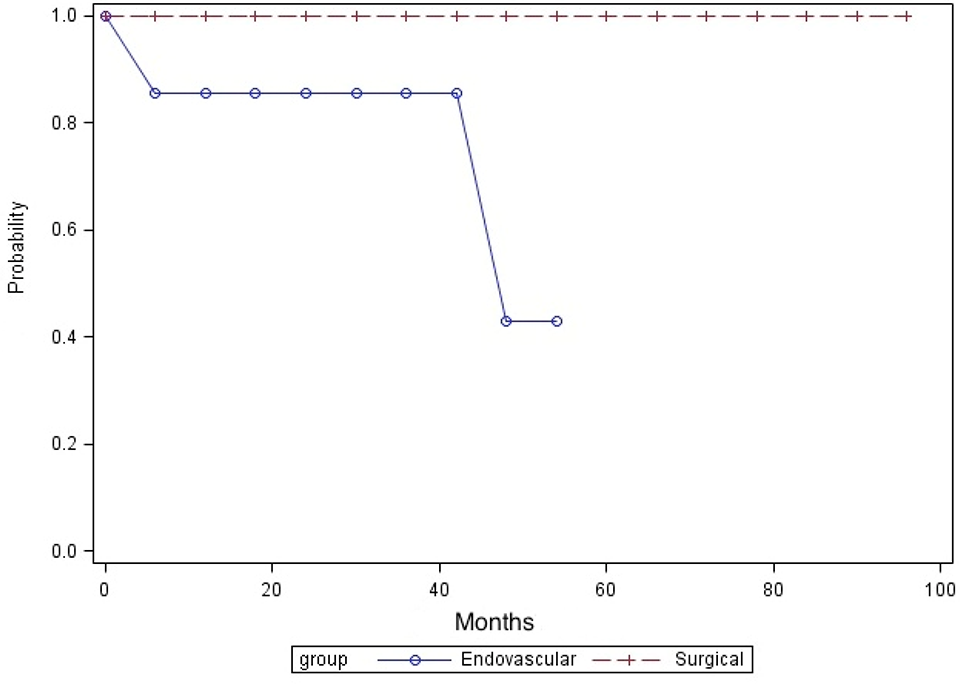
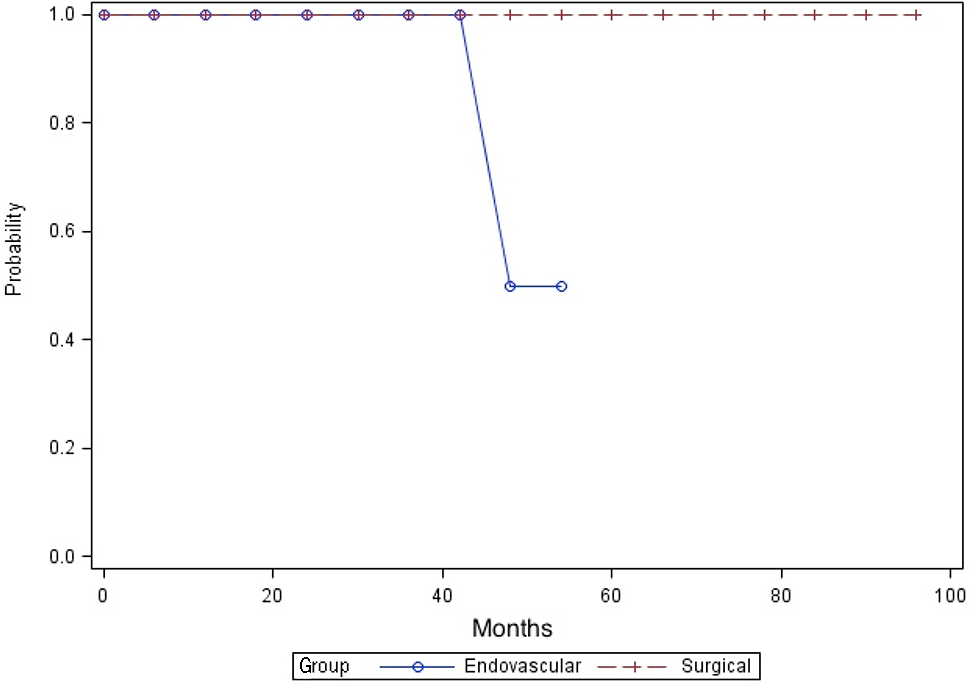
Of the 16 patients in the endovascular group, 12 were alive at the time of this review. The mean post procedural survival was 30.5 months. Three patients had imaging within the last year. Overall seven of 16 patients in our endovascular group had follow-up imaging, which ranged from seven to 54 months with a mean of 26.6 months. Of those patients three were imaged with ultrasound showing patency. One had an asymptomatic occlusion by ultrasound. One patient had asymptomatic narrowing by CTA. One patient who had an angioplasty alone required secondary stenting four months after his initial procedure for symptomatic re-stenosis. Three-month follow-up angiography showed a 90% in stent re-stenosis. He had developed collateral circulation, was asymptomatic and, therefore, further intervention was not pursued. A single patient in this group also underwent an ECIC bypass during the follow-up period. By lifetable analysis there was no significant difference in survival between the two groups (Figure 1). The primary and assisted primary patency rates were better in the surgical group (Figures 2 and 3) but this did not reach statistical significance.
Survival of patients treated for proximal vertebral artery disease Primary patency of treated vertebral arteries Assisted primary patency of treated vertebral arteries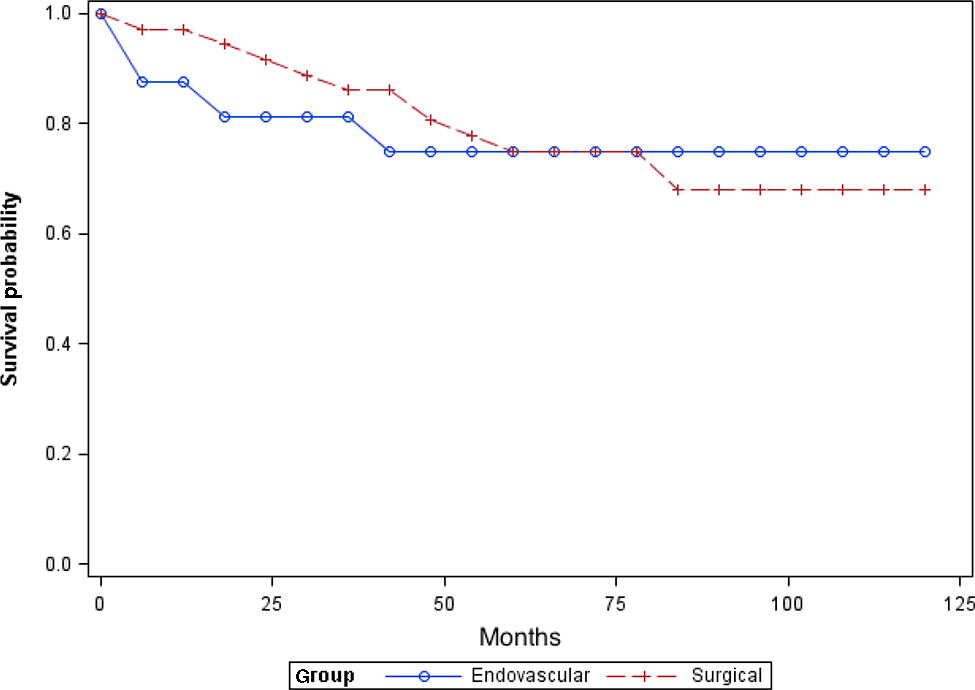
Discussion
Symptomatic VAD is much less frequently encountered than carotid artery occlusive disease. Nevertheless, it has been identified in 25–40% of patients with cerebrovascular disease. Its symptoms may be manifest secondary to an embolic event causing a transient ischemic event or stroke. In addition, patients can develop hemodynamic insufficiency to the hindbrain from VBI. The most common cause of VAD is atherosclerosis, although other etiologies include trauma, dissection or rare arteriopathy. Anatomically, the vertebral artery normally arises from the proximal posterior subclavian artery although in 8% of the patients the left vertebral artery takes its origin off from the aortic arch. The vertebral artery is divided into four segments (V1, V2, V3 and V4). The V1 segment is the portion of the artery from its origin to the point at which the artery enters the transverse cervical foramen (usually at the C5 or C6 level). The V2 segment is the trans cervical foramina portion and the V3 segment is the short length of the artery from its exit from the C2 transverse cervical foramen up to the point at which the artery enters the skull base. The V4 segment is the intracranial portion of the vessel which terminates in the basilar artery, usually after joining the contralateral vertebral artery. Occasionally, the vertebral artery is aplastic, hypoplastic or terminates in the PICA. While atherosclerosis can involve any segment or segments of the vertebral artery, it most frequently involves the V1 segment. Many of these patients also have associated carotid artery and intracranial cerebral occlusive disease.
The initial treatment modality of posterior circulation disease has always been medical. The failure of medical treatment, however, in many cases eventually leads to surgical intervention. The surgical methods of treating proximal vertebral artery occlusive disease are protean and historically date back about 50 years.
7
Ligation, endarterectomy and bypass have all been employed.
18
Currently, transposition of the V1 segment to the ipsilateral common carotid is the preferred surgical method at our institution as well as others6,10 (Figure 4). The modern surgical results for this operation are reported to have a stroke rate of 1.9% and a death rate of 0.9% with five-year patency rates of 80%.
10
Vertebral to carotid artery transposition anastomosis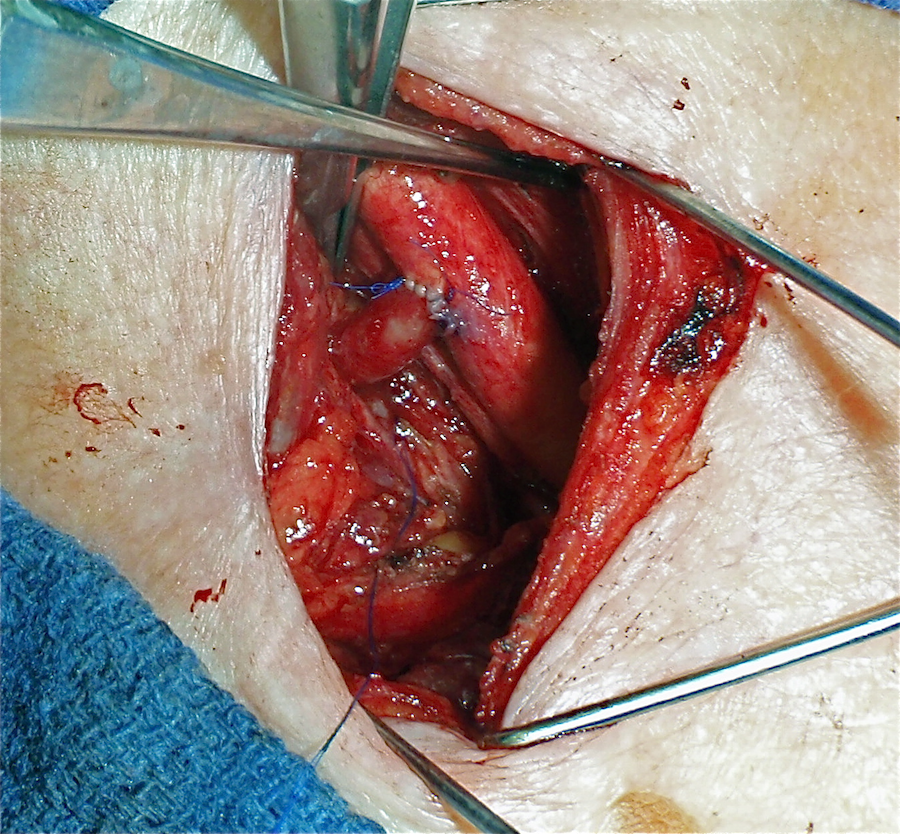
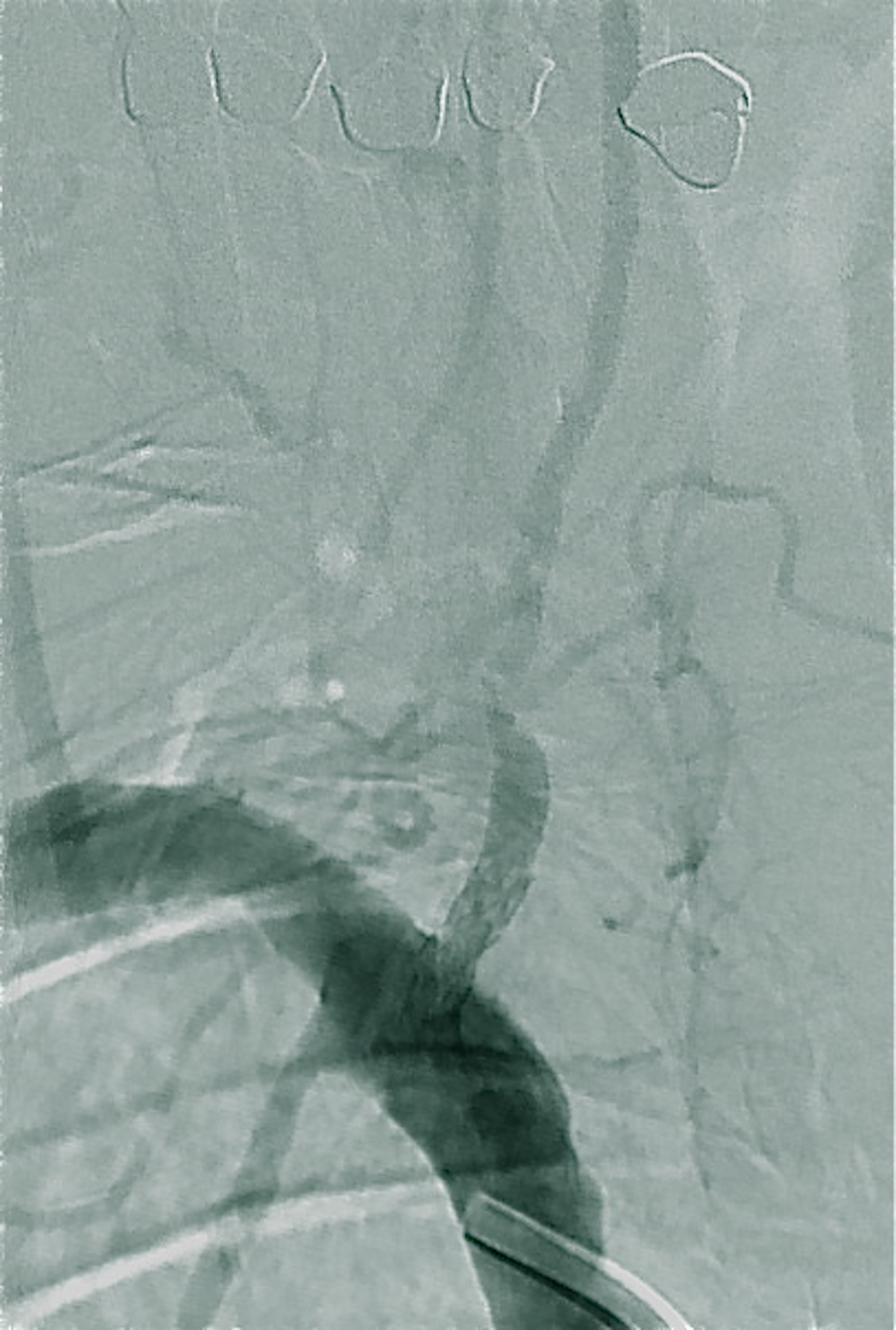
Endovascular treatment of the vertebral artery was first reported in 1981 when an intraoperative angioplasty was performed. Over the next 20 years there were many more reports of percutaneous angioplasty (PTA) of the VA (Figures 5 and 6). In the last 10 years, stent angioplasty of the VA has been increasingly performed to address the problems of dissection and recoil that PTA alone suffered (Figures 7 and 8). Yet, objective evidence of the appropriate treatment for proximal vertebral artery occlusive disease remains incomplete. A recent Cochrane review could find only a single randomized trial involving only 16 patients split between medical and endovascular treatment.
19
Twenty case series were identified in which a total of 313 patients were treated with angioplasty (160) or stenting (173) in which the 30-day major stroke and death rate was 3.2% and the TIA and non-disabling CVA rate was also 3.2%. Over 90% of patients have been reported to have improved after interventional treatment for proximal VAD.4,13,14,17,20 Problems noted after endovascular treatment include re-stenosis rates of 10–43%
1
and stent fracture.
21
Severe left vertebral artery stenosis Severe left vertebral artery stenosis after percutaneous angioplasty Severe right vertebral artery stenosis Right vertebral artery after primary stenting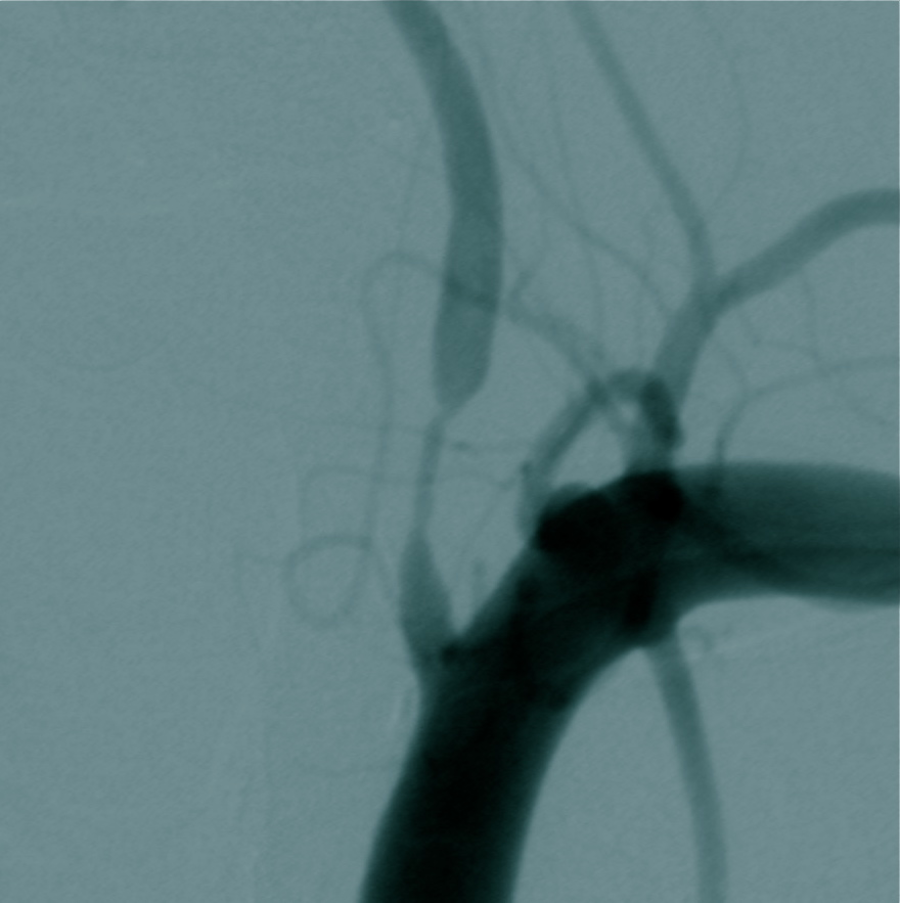


We sought to review the experience at our institution during the last 10 years in treating proximal VAD with surgery or endovascular techniques and more specifically to determine the type of patients, their pretreatment symptoms, interventional treatment and results according to type of revascularization given the increasing use of angioplasty and stenting and the limitations in those reports as noted above. The patients in our review are equivalent to those in both the surgical and endovascular reports with regard to age, co-morbidities, presence of carotid disease and intracranial cerebral occlusive disease. The incidence of diabetes in these patients is lower than usually seen in patients with carotid artery occlusive disease and peripheral artery occlusive disease. 10 This has been reported, but not specifically noted, in other reports of VA disease. There was a significant incidence of associated carotid artery and intracranial occlusive arterial disease as well. Our two subgroups (surgical and endovascular) were comparable with each other as well. There was a higher proportion of women, in the endovascular group but this was not statistically significant due to the small sample size. The symptom distribution of the patients in our surgery group also is comparable with those in the literature having surgical revascularization. In our endovascular group there were significantly higher number of patients being treated for acute stroke compared with our surgery group as well as with other endovascular studies reported. We found that many of the endovascular patients were referred directly to neuroradiology after being admitted with a stroke. More of the surgical patients were evaluated electively for vertebro-basilar symptoms. This led to a selection bias with a much higher percentage of stroke patients in the endovascular group compared with the surgery group and with those reported in the literature.
Our surgical results also compare favorably with previous reports and we believe are consistent with the expected morbidity and mortality of the procedure for symptomatic patients with V1 disease. 10 The single death in the surgical group was secondary to the intraoperative injury of the left internal mammary artery (LIMA) which had been used previously during a coronary bypass procedure. Obviously, caution should be used when performing a left-sided vertebral transposition to avoid the LIMA in case it has been used or will be used for coronary revascularization. The morbidity and mortality of our endovascular results are inferior to other reports with regard to symptomatic relief and early survival. This could relate to the higher percentage of patients with stroke who were present in this study group. It is well accepted that stroke does adversely affect survival and the two patients who died within six weeks of their procedure had presented with acute strokes. Interestingly, these were not the patients who required percutaneous thrombectomy of their basilar artery. However, the patients who were treated endovascularly and did not present with an acute stroke fared equally poorly with regard to symptomatic relief compared with the stroke patients minimizing this argument. EPDs also were not used during the majority of our endovascular procedures but the majority of endovascular patients reported have not had an EPD used, so this is unlikely to have affected our results compared with other reports. These diminished results also could be related to the fact that stents were not routinely utilized in the endovascular group and PTA alone might not provide the same hemodynamic improvement compared with PTA with stenting. In a previous study of angioplasty only of the vertebral artery only 62% of patients were improved or cured of symptoms. 22 A more recent study used stents routinely and 84% of patients were cured or improved. 3 The proximal segment of the VA can be unsuitable for stenting because of its small diameter, tortuosity and often post stenotic dilation can make it a difficult size match. The effect of using drug eluting stents is unknown at this time. In the surgical group it was noted that there were more patients treated for unilateral disease of a dominant vertebral artery than in the endovascular group. This, however, did not adversely impact the surgical results and all of these patients benefited from the procedure whereas only one of two benefitted in the endovascular group. Therefore, in selected patients such as these surgery appears to be beneficial. This finding, combined with the observation that even the VBI patients in the endovascular group did not respond as well as the surgery patients, suggests that surgery may lead to a better hemodynamic result.
Conclusion
Patients with proximal vertebral artery occlusive disease often present with multiple symptoms and/or strokes. They frequently have signficant cerebrovascular disease affecting the carotid arteries, contralateral vertebral arteries and intracranial vessels. Both vertebral to carotid artery transposition and vertebral angioplasty can be performed safely with a high degree of success in these patients with comparable morbidity and six-week mortality. Some of these patients will require further intervention to alleviate their symptoms as we had patients in both groups who later had ECIC bypasses and pacemaker implantation. Based on our experience, symptomatic relief appears to be better after surgical reconstruction than endovascular therapy and is even beneficial in selected patients with vertebro-basilar symptoms secondary to a severe unilateral stenosis in a dominant vertebral artery. The long-term patency of surgical reconstruction is superior to that of endovascular intervention and the need for secondary intervention is similarly less. It would appear from these data that surgical reconstruction is currently the preferred elective treatment for proximal VAD.