
Abstract
Recent improvement in the survival of patients presenting with a ruptured abdominal aortic aneurysm (rAAA) has been credited to endovascular aneurysm repair (EVAR). We present our clinical series in the management of rAAA from 2007 to 2011. A total of 55 consecutive patient charts were reviewed. Thirty-eight patients underwent EVAR, 17 of the 55 patients did not have favorable anatomy for EVAR. Nine of the 17 patients underwent standard open repair. Eight patients underwent a ‘hybrid repair’ defined as suprarenal aortic endovascular balloon control followed by open repair. Overall 30-day mortality for all 55 patients was 22%. Mortality for the patients managed by endovascular aortic aneurysm repair was 26% compared with 22% with open repair. There were no deaths in the eight patients undergoing the hybrid repair. Endovascular balloon control of the aorta followed by open rAAA repair in patients who are not candidates for rEVAR has produced good results in our experience. Improved results being reported in the management of rAAA may not be on the basis of endovascular repair alone.
Introduction
Since the introduction of endovascular aneurysm repair (EVAR), the procedure was regarded as an appealing minimally invasive alternative to the traditional open standard approach of abdominal aortic aneurysm (AAA) repair. EVAR subsequently became established as an effective entity in the treatment of AAA with an early postoperative mortality advantage that is eventually lost in 18–36 months.1–5 Gradually, endovascular approach began to become utilized for complex vascular pathologies including ruptured AAA repair (rAAA). 6 Subsequent studies reveal a 30-day mortality advantage of rAAA treated with EVAR (rEVAR) as compared with open AAA repair with ranges of 18–39% as compared with 40–52% mortality, respectively.7–9 However, EVAR repair remains only suitable in about 42–67% in case of rAAA, which is mostly secondary to decreased infrarenal neck length and increased neck diameter as compared with elective AAA repair.10–13 It should be noted that EVAR might not be feasible in all facilities given the technical challenges and the dedicated operating room personnel and equipment that it requires.
We hereby present our experience in the management of rAAA from 2007 to 2011. We describe the institutional protocol that we follow for all rAAA that present to the emergency room and summarize the results that are apparent from following the three different treatment paradigms of standard open rAAA repair, rEVAR and hybrid repair. Hybrid rAAA repair as defined with endovascular proximal aortic balloon control in open ruptured AAA repair in patients who are not candidates for rEVAR. Endoluminal balloon occlusion has been described in endovascular ruptured aortic aneurysm repair for proximal control of bleed particularly in hemodynamically unstable patiens.14–16
Methods
Institutional Review Board permission was obtained and a retrospective chart review was performed for all consecutive patients who presented with rAAA from 2007 to 2011. The total number of patients was 55. Patients who were pronounced dead upon arrival or in emergency room were not accounted for in our patient population. An established protocol was followed when patients presented to the emergency room with suspicion of rAAA. The concept of permissive hypotension in this situation is embraced with avoidance of aggressive fluid resuscitation. Patients were stratified into to two groups: stable and unstable patients. Unstable patients were consistently hypotensive with systolic blood pressure (SBP) < 80 mmHg that lasted more than 15 minutes. Unstable patients who presented with no previous imaging had bedside abdominal ultrasonography in emergency room upon arrival when an rAAA was suspected before being taken directly to the operating room where an aortography was performed. A total of nine patients or 16% of the total patient population were hemodynamically unstable: three in rEVAR group (7.8%), three in open repair group (33%) and three in hybrid repair group (37.5%). The choice of treatment was dependent on anatomy of rAAA with patients who had an aneurysm neck length of at least 10 mm and non-occluded iliac vessels undergoing rEVAR. While patients who had an AAA neck length of less than 10 mm or occluded or nearly occluded iliac vessels underwent open or hybrid rAAA repair. The decision to undergo open standard repair or hybrid rAAA repair was dependent on surgeon preference.
Fourty-six patients presented to the emergency room department hemodynamically stable and were taken immediately to the computed tomography (CT) scan for thin-sliced CT scan (2.5 mm cuts) to determine patients with anatomy favorable for rEVAR (Figure 1). Patients who were candidates for EVAR with favorable iliac landing zone that were hemodynamically stable underwent aorto-biliac graft repair. Among patients who had EVAR those who were unstable or had unfavorable iliac landing zone had aorto-uniliac graft with occluder and femoral–femoral bypass.
Ruptured AAA treatment algorithm. AAA, abdominal aortic aneurysm; CTA, computed tomography angiography; EVAR, endovascular aneurysm repair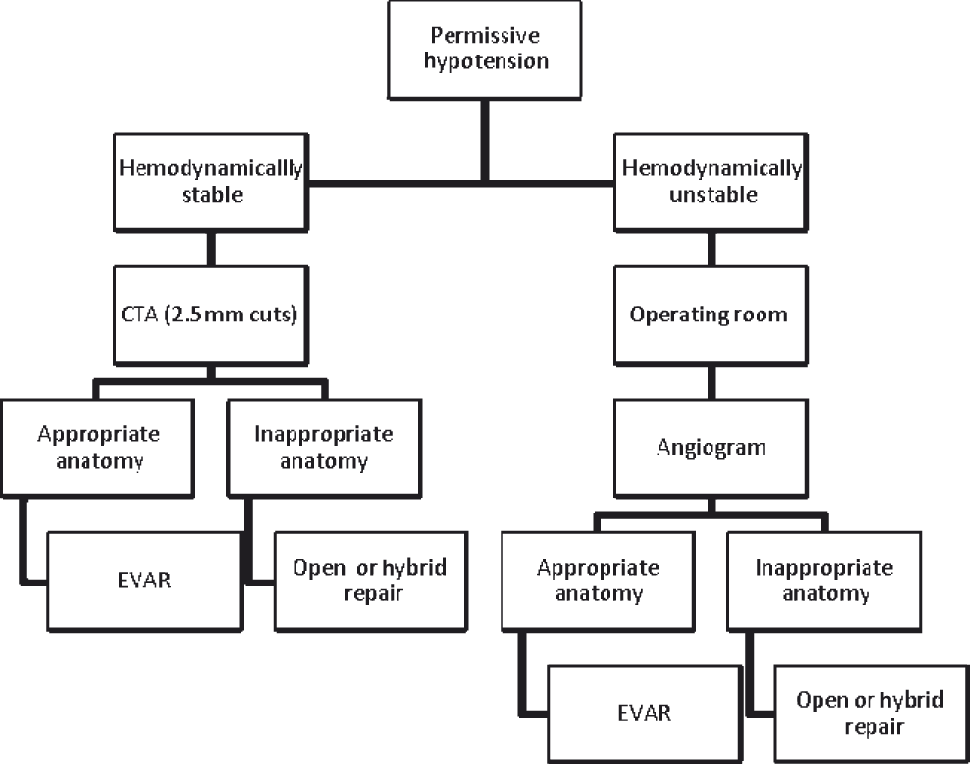
The technique of proximal aortic balloon occlusion was performed in the following manner. Under ultrasound guidance the common femoral artery is accessed bilaterally with two 6F Proglide sutures. In patients with excessive calcifications in the walls of common femoral artery (CFA) a cut down was performed. Subsequently, a 12F sheath is placed in one CFA while a 6F Proglide is placed in the contralateral CFA. Compliant occlusion balloon is then inserted through the 12F sheath and advanced into the abdominal aorta under fluoroscopic guidance. Subsequent inflation of the compliant balloon proximal to the rAAA would then be performed. Aortogram is performed. General anesthesia would be induced after establishing proximal balloon control. Endovascular repair was performed when anatomy was favorable in 38 patients. Standard open repair was performed in 17 patients when anatomy was not favorable for endovascular repair. Combined open rAAA repair along with maintaining endovascular control of aorta proximal to rAAA (hybrid rAAA repair) was performed in eight patients while nine patients underwent open rAAA repair without proximal balloon control.
Results
Patient demographics for the three treatment modalities
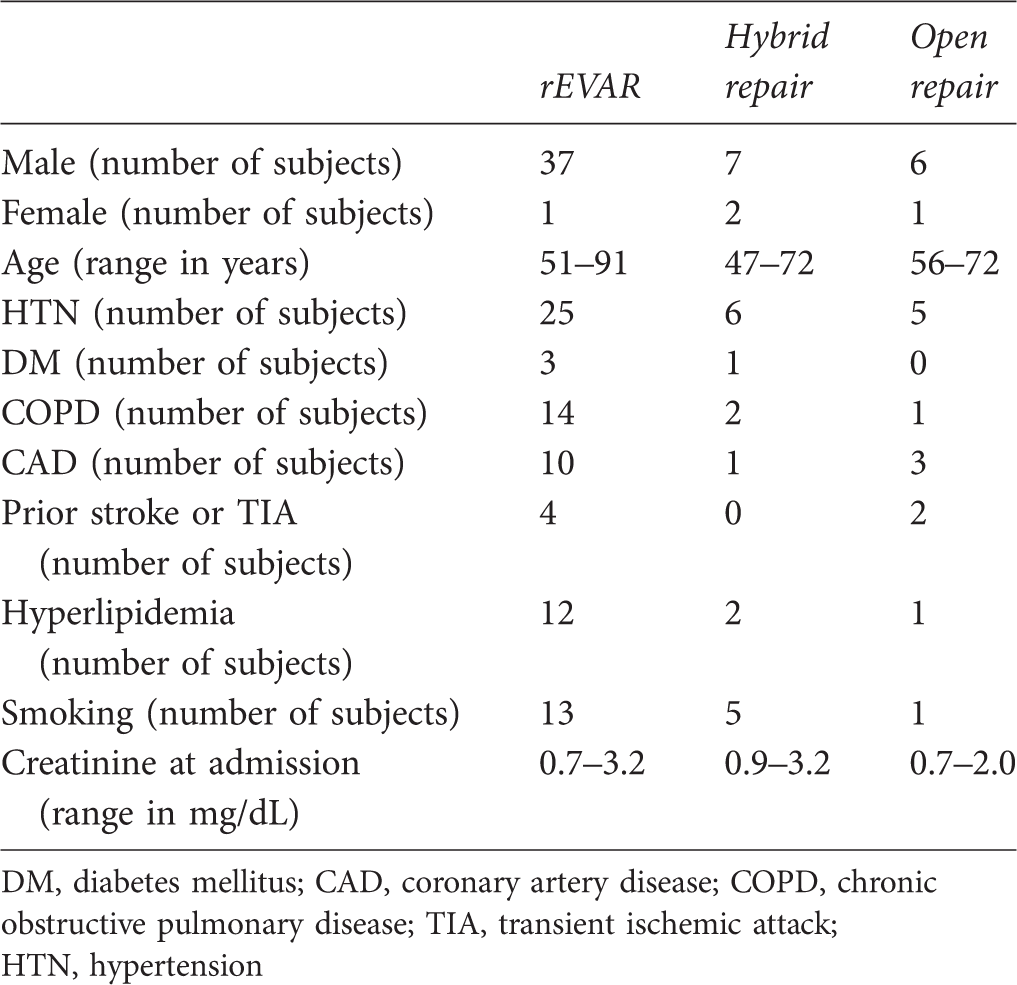
DM, diabetes mellitus; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; TIA, transient ischemic attack; HTN, hypertension
Primary outcome is 30-day mortality. Overall mortality was 21.8%; in the EVAR group was 26% (n = 10), open group was 22% (n = 2) and 0% in the hybrid group. Secondary outcomes included myocardial infarction (MI), renal failure, ischemic colitis and compartment syndrome. Two patients had postoperative MI in the EVAR group (5.2%) and none in the other two groups. Postoperative renal failure was 31.6% (n = 12) in EVAR group compared with 44.4% (n = 4) in open group and 62.5% (n = 5) in hybrid group. Eighty percent of patients with renal failure in the hybrid group needed hemodialysis, but none in the other two groups. Incidence of ischemic colitis was 25% among patients with hybrid approach as compared with none in open approach and EVAR. The incidence of postoperative compartment syndrome requiring decompressive laparotomy was 7.9% in EVAR group with none in open and hybrid approach.
Discussion
Even with the advances in graft designs to accommodate more challenging AAA anatomy, not all patients are eligible for EVAR. In our study, about 69.1% (n = 38) were eligible for EVAR which is similar to the reported range in the literature, 42–67%.10–13 Using intra-aortic proximal balloon control to control bleeding in rAAA patients has been described mostly for EVAR in hemodynamically unstable patients.14–16 We have applied this to our proposed hybrid approach in patients with rAAA and anatomy unfavorable for endovascular repair. Proximal aortic control prior to the induction of general anesthesia is of utmost importance to prevent further hypotension in these high-risk patients.
Following an institutional algorithm protocol for the management of rAAA has been shown to improve outcomes with up to 35% risk reduction in 30-day mortality.17–19 The protocol followed in our institution stratifies patients into hemodynamically stable or unstable groups. Stable patients underwent a preoperative thin-cut CT scan while the hemodynamically unstable group (patients with SBP < 80 mmHg) were taken immediately to the operating room. Thirty-eight patients had EVAR, nine had open repair, and eight underwent a hybrid rAAA approach.
Overall 30-day mortality rate for all approaches for rAAA was 21.8%. Subgroup analysis revealed a 26% mortality rate (n = 10) in the EVAR group. The 22% mortality rate in standard open approach group and no mortalities in hybrid approach group which falls well below the reported range of standard open approach rate of 40–52%.7–9
Postoperative renal failure was higher in the hybrid group (62.5%) as compared with the EVAR (31.6%) and open groups (44.4%). Postoperative MI was more evident in open rEVAR group with 5.7% which is similar to reported literature rate. 20 No incidence of MI was reported in both hybrid AAA repair and open AAA repair. There was no evidence of compartment syndrome in the open or hybrid group, while the EVAR group had a 7.9% incidence lower than the reported rate of 20%.20,21
The higher incidence of renal failure and ischemic colitis in the hybrid repair group as compared with the open repair group or rEVAR group might be partially due to selection bias because of the presence of more hemodynamically unstable patients in the hybrid group (37.5%) compared with the open (33%) or rEVAR groups (7.8%). It is important to mention at this point that given the small sample size in all three groups and specifically the hybrid group (only 8 patients) it is difficult to make overachieving conclusions concerning the lack of mortality in this group or the increased incidence of renal failure (in 5 patients) and ischemic colitis (in 2 patients). Therefore, large-scale studies need to be conducted to better elaborate and evaluate hybrid repair compared with rEVAR and traditional open rAAA repair.
The limitations of our study is: retrospective review, single institution, multiple operators and small sample size of 55 patients with only eight having had hybrid rAAA repair performed.
Finally, technical problems that can be encountered with establishing proximal aortic balloon control are problems encountered with vascular access with difficulty cannulating the artery in case of weak or absent pulses, potential dissection, pseudoaneurysm, thrombosis or occlusion of the native arteries. In two small series, trans-femoral balloon occlusion was associated with no direct complications.16–19
Conclusion
While we await the results of the randomized controlled trials such as the Amsterdam Acute Aneurysm trial 22 and IMPROVE trial (ISRCTN 48334791) to provide answers with regard to the definitive treatment modality for rAAA, it has become apparent that the sample size for patients being enrolled in the Amsterdam Acute Aneurysm trail has been increased as the results of open rAAA repair are proving to be better than anticipated. At this time then, management of rAAA appears to present a clinical equipoise.
Endovascular balloon control of the aorta followed by open rAAA repair in patients who are not candidates for rEVAR has produced good results in our experience. Large-scale studies and multi-institutional expertise will be necessary to validate our claim.