
Abstract
The optimal treatment of patients facing imminent amputation after multiple (≥2) failed prior ipsilateral bypasses is unclear. We analyzed a group of patients undergoing multiple lower extremity bypasses for limb salvage to assess the utility of attempting multiple revascularizations. From 1990 to 2005, 105 revascularization procedures were performed in 55 limbs of 54 patients with imminent limb-threatening lower extremity ischemia after failure of ≥2 prior infrainguinal bypasses in the same leg. Fifty-five operations were the third procedure (Group A) and 50 operations were the fourth or more (Group B). We compared primary/secondary patency and limb salvage rates by Society for Vascular Surgery criteria. Limb salvage rates did not differ between patients undergoing a third bypass and those undergoing four or more bypasses at one year (62 versus 65%, NS) or at three years (58 versus 61%, NS). Secondary patency was not different between groups (76 versus 76%, P = NS) at one and three years (71 versus 70%, NS). Primary patency also did not differ between the two groups, at one year (24 versus 35%, NS), or at three years (11 versus 15%, NS). No differences were observed in morbidity and mortality rates between the groups. In conclusion, the likelihood of success of repetitive limb revascularization was unrelated to the number of previous failures. The expected incremental failure rate with each successive bypass was not found. These results, coupled with the three-year limb salvage rate of over 50% in patients who otherwise would have required amputation, lend support to aggressive use of limb revascularization in selected patients even after two or more failed bypasses.
Keywords
Introduction
Since its inception, lower extremity bypass has been considered the gold standard treatment for limb-threatening lower extremity ischemia. With the aging population as well as improvements in technique, these procedures have been performed with increasing frequency over the past several decades. Recently, endovascular techniques have been applied more often in these patients, and while many centers, including our own, have adopted an ‘endovascular first policy’, the results of these procedures have yet to match the durability of open surgery, for which there remains a role in the treatment of chronic limb ischemia. However, bypass grafts also have finite life spans and require close follow-up and commonly reintervention. Even with close monitoring there is a significant failure rate with many patients experiencing recurrent symptoms of severe lower extremity ischemia. A subset of patients may require multiple re-interventions and/or bypasses for effective limb salvage. The optimal treatment of such patients facing imminent amputation after two or more failed bypasses is not well known. Many authors believe that primary amputation is better than another bypass in this setting while other reports have supported multiple bypass attempts for limb salvage after the failure of two previous bypass grafts.1-3 Studies have also shown that while autogenous conduit is preferred, successful limb salvage can be achieved with prosthetic grafts and that patient survival is improved with successful limb salvage.4-6 Moreover, one might suspect that patients undergoing a lower extremity bypass after two or more previous failures would have a poorer outcome on the basis of disease severity and progression, as well as the difficulties associated with re-operation. These difficulties include complicated redo dissections, increased risk of subsequent graft and/or wound infection, lack of a suitable autogenous conduit, and the need for more proximal inflow and/or more distal outflow. However, whether or not there is a marked reduction in patency and/or limb salvage rates and an increase in complications in patients undergoing multiple bypasses are unclear.
For many years our policy has been to avoid amputation in patients with imminent limb threat by further attempts at limb revascularization even when patients have failed two or more previous bypasses.7,8 Although we have had anecdotal successes, we did not have stronger evidence that these repetitive re-vascularizations were justified. In the present report we analyze the outcomes of this approach.
Methods
A review of information in our prospectively collected vascular database was conducted. From 1990 to 2005, we identified in 55 limbs of 54 patients undergoing a total of 105 surgical revascularization procedures performed for imminent limb-threatening lower extremity ischemia after failure of two or more prior ipsilateral infrainguinal bypasses. The hospital and office records of these patients were reviewed. For the purposes of this study only new bypasses or extensions and revisions were included. Thrombectomy, thrombolysis and/or balloon angioplasty with or without stenting were not included as separate procedures in this analysis although they may have contributed to the calculation of secondary patency.
The patients were then divided into two groups for analysis. Group A was comprised of all third procedures and consisted of 55 operations in 54 patients. Group B was comprised of all fourth or higher reconstructive arterial procedures and included 50 operations in 26 patients. Thus, 26 of the 54 patients having a third bypass went on to have a fourth or more bypasses, for an additional 50 procedures (Figure 1). Group A and Group B were then compared with regard to primary patency, secondary patency and limb salvage rates according to established Society for Vascular Surgery (SVS) criteria. 9 To assess for any demographic differences between the group of patients undergoing three procedures only and those undergoing four or more procedures, the subgroup of 28 Group A patients who had only three operations (Group Aa) was compared with the 26 Group B patients.
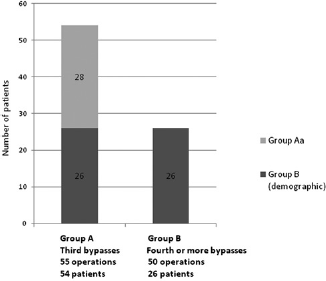
Graph showing the 28 patients undergoing three bypasses only (Group Aa, light gray) and the 26 patients who underwent a third, and ultimately a fourth or more bypasses (Group B demographic, dark gray)
Patients were followed until their death or, if they survived, for at least five years with serial pulse examinations and surveillance duplex at one, three, six, nine and 12 months postoperatively and every six months thereafter. Graft patency was determined according to SVS criteria. 9 The mean follow-up for group A patients was 23 months with a range of 3-76 months from the time of the third operation and the mean follow-up for group B patients was 43 months with a range of 3-122 months from the time of the fourth operation. The mean length of follow-up for all patients from the time of their first arterial revascularization procedure was 60 ± 43 months (median 48 months, range 10-217 months).
Demographic data and risk factors were compared between patient groups; continuous variables were analyzed using Student's t-test, whereas univariate analysis of categorical variables was performed using Fisher's exact test or Yates’ correction, as indicated (c2 for contingency tables, two-tailed P value). Primary and secondary graft patency, limb salvage, and patient survival were determined using the Kaplan-Meier method. The log-rank test (Mantel) was used to specify statistical differences between the subgroups. For statistical analyses, SPSS for Windows version 11.0 (SPSS Inc, Chicago, IL, USA) was used.
Results
There were no significant differences in the demographic data of patients having only three operations (Group Aa) and those having four or more operations (Group B) (Table 1). Of note, 36 of the 54 patients (67%) had significant enough peripheral vascular disease involving the contralateral limb to require either operative revascularization and/or amputation (Group Aa: 64%, Group B: 73%), and one patient had multiple surgical revascularization procedures on both lower extremities. The majority of patients in both groups were on warfarin anticoagulation with a slightly higher, but not significantly greater number, in Group B (Group Aa: 75%, Group B: 92%). There was no statistically significant difference between the groups with regard to the incidence of hypertension, coronary artery disease, tobacco use, diabetes mellitus, hyperlipidemia and end-stage renal disease. There was, however, a somewhat lower incidence of end stage renal disease than might be expected in both groups.
Demographic characteristics comparing Group Aa (patients with a third bypass only) with Group B (patients with four or more bypasses)
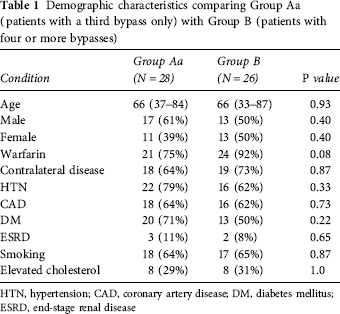
HTN, hypertension; CAD, coronary artery disease; DM, diabetes mellitus; ESRD, end-stage renal disease
The indication for revascularization for all patients in this series was severe limb-threatening ischemia and no patient underwent re-operation unless major amputation was felt to be imminent. Progressive gangrene or ulceration (category 5 chronic ischemia) was the indication for intervention in 44 of 55 Group A procedures (80%) and in 44 of 50 Group B procedures (88%). Severe rest pain (category 4 chronic ischemia) was the indication in 11 (20%) Group A procedures and 6 (12%) Group B procedures (P = NS). 6
Procedures considered in this report fell into two categories, new bypasses and revisions/extensions. A new bypass was defined as placement of a new conduit with two new arterial anstomoses. A revision/extension was defined as placement of a new bypass graft but utilizing a short portion of patent or thrombectomized, proximal or distal existing graft for inflow or outflow.
There were a total of 31 (56%) new bypasses in Group A and 28 (56%) in Group B (P = NS). There were 24 (44%) revisions/extensions performed in Group A and 22 (44%) in Group B (P = NS). Within Group B, 26 of the 50 total procedures were fourth procedures (52%), 15 were fifth procedures (30%), four were sixth procedures (8%), two were seventh procedures (4%), two were eighth procedures (4%) and there was one ninth procedure (2%). Therefore 48% of the patients in this report had four or more operations and 28% had five or more operations.
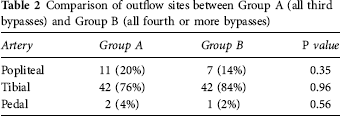
The outflow vessel in both groups was primarily the tibial arteries with a distribution that was similar between the two groups (Table 2). The below-knee popliteal artery was used for outflow in 11 (20%) Group A procedures and 7 (14%) Group B procedures. Tibial outflow was used in 42 (76%) Group A procedures and 42 (84%) Group B procedures. There were 2 (4%) Group A procedures and 1 (2%) Group B procedures that were performed to pedal or plantar vessels.
Comparison of outflow sites between Group A (all third bypasses) and Group B (all fourth or more bypasses)
Autogenous conduit was used in 36 (34%) of the total procedures, 24 (43%) in Group A and 12 (24%) in Group B (Table 3). Greater saphenous vein (GSV) was the most commonly used autogenous conduit, used in 15 (27%) of autogenous Group A procedures and 6 (12%) of autogenous Group B procedures. Lesser saphenous (LSV) and arm veins were less frequently utilized comprising 6 (11%) and 3 (6%), respectively, of autogenous reconstructions in Group A, and 1 (2%) and 4 (8%), respectively, of autogenous reconstructions used in Group B. One procedure in Group B utilized cryopreserved vein. Prosthetic material (Ringed PTFE; WL Gore, Flagstaff, AZ, USA) was used in 63 (60%) of the total reconstructions, including 30 (55%) in Group A and 33 (66%) in Group B. Composite sequential grafts were used in six cases, 1 (2%) in Group A and 5 (10%) in Group B. These composite sequential reconstructions were performed with grafts consisting of a proximal portion of polytetrafluoroethylene (PTFE) and a distal segment of vein. The reconstructions were accomplished by securing the distal vein bypass to the outflow artery and then to the isolated patent proximal segment. The proximal PTFE reconstruction was then performed with anastomoses to the inflow artery and to the proximal portion of the vein graft. 10 There were no significant differences between the groups with regard to the conduit used.
Conduits used for bypass in Groups A (all third bypasses) and B (all fourth or more bypasses)
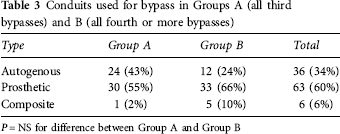
P = NS for difference between Group A and Group B
The 30-day operative mortality for Group A was 0 (0%) and for Group B was 2 (4%) for an overall rate of 2% (Table 4). Other 30-day morbidity included one myocardial infarction in Group A, one wound infection in Group B, one wound hematoma in Group A and four in Group B. One patient in Group A required prolonged ventilator support.
Complications in Group Aa (all third bypasses) and Group B (all fourth or more bypasses)
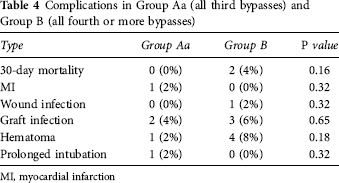
MI, myocardial infarction
The one- and three-year primary patency rates for Group A procedures were 24 and 24%, while for Group B procedures they were 35 and 19%, respectively. These differences were not statistically significant. The one- and three-year secondary patency rates for Group A procedures were 76 and 71%, while for Group B procedures they were 76 and 70%, respectively. These differences were also not statistically significantly different. The one- and three-year limb salvage rates analyzed by procedure were 62 and 58% for Group A and were 65 and 61%, respectively, for Group B procedures. Limb salvage rates, analyzed either by procedure or by limb, were not statistically significantly different between the two groups. Kaplan-Meier curves for limb salvage are shown in Figure 2.
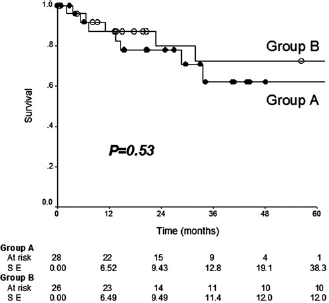
Kaplan-Meyer curves for limb salvage in the two groups
Discussion
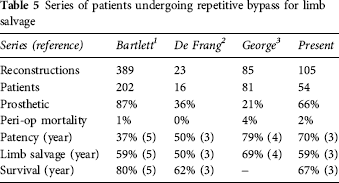
Secondary bypasses for limb ischemia are largely assumed to have marginal patency and limb salvage rates. Over the past several decades we have maintained an aggressive approach to revascularization and limb salvage even in patients with multiple previous bypass failures and when the use of prosthetic grafts is required. 7 Other authors have also advocated such an approach (Table 5) with similar reported outcomes.1-3 However, the question has legitimately been raised, ‘when is enough, enough?’. 8
Series of patients undergoing repetitive bypass for limb salvage
We, like other authors, have found that the overall 30-day and three-year morbidity and mortality in this cohort of patients with advanced peripheral vascular disease undergoing repetitive bypass procedures was surprisingly low, with a three-year patient survival of 62% in Group Aa and 73% in Group B.1,2 Additionally, an incremental increase in mortality in the group having four or more bypasses was not found.
It is not surprising that there was a higher (NS) percentage of tibial bypasses and prosthetic conduit used in the group B patients reflecting the need for a more distal outflow with successive bypasses. Our use of LSV and arm vein reflects our commitment to the use of vein for tibial and plantar bypasses whenever possible. Veins were evaluated preoperatively with duplex and judged to be suitable only if they measured at least 2.4 mm in diameter and dilated to approximately 3 mm at the time of operation. When analyzed by conduit, primary patency between the groups was roughly equivalent while secondary patency for PTFE was better, but not significantly different than for vein. In this group of patients undergoing multiple bypasses these results suggest that, while a good vein is preferable to PTFE, PTFE is preferable to a poor quality vein. Although half the veins used in this study were GSV in many cases these were short segments and represented residual small ipsilateral or contralateral GSV. Additionally, the ability to restore patency with thrombectomy or thrombolysis with PTFE at least in part explains why PTFE had higher secondary patency rates than vein.
There are several inherent significant limitations in the current study. First, our data were prospectively collected, but was retrospectively analyzed. Second, for the purposes of patency (but not demographic) analyses a subset of Group A patients, undergoing four or more bypasses, make up the patients in Group B. We felt such an approach would be useful to evaluate for the effects of an increasing number of bypasses. We recognize that this is essentially a descriptive study of a group of patients who underwent repeat bypass procedures, with outcomes that exceed what might be expected in such a complex group. Third, this study contains a select, and perhaps somewhat more resilient, group of patients who were able to progress to the multiple bypass category. Fourth, although we have characterized the outflow vessels the procedures performed in this study represent a heterogeneous group as might be expected in such a patient population. Fifth, we did not perform a cost or quality-of-life analysis for this study, although previous studies have suggested a cost advantage of successful revascularization. 11 Sixth, decisions regarding the risk of limb threat and the need for intervention were based on clinical judgment, and as such are somewhat subjective in nature. Finally, there was insufficient hypercoagulability data available for inclusion in this report. Whether or not improvements in medical therapy, especially antiplatelet medications which were widely used, contributed to these results in relation to previous studies is unclear.
The decision to divide the patients into groups, those having had three operations and those having had four or more, was arbitrary since this division allowed for an approximately equal group of procedures and patients in both groups. This division also allowed us to test the premise of worsening outcomes with successive bypasses as well as to test for demographic differences between these two groups.
Another important issue that cannot be answered by the current study is that of patient selection for multiple revascularization procedures. The selection criteria for re-operation was not addressed and the number of patients who failed two or more bypasses and who were not candidates for repeat intervention on the basis of no outflow, severe infection or non-ambulatory status was not determined. Therefore, the denominator of the entire group of potential patients is not known. However, our philosophy has been that any patient who is ambulatory and active, has suitable inflow and outflow arteries, is free from progressive gangrene or infection at the proposed bypass anastomotic sites, and who can provide informed consent, should have an attempt at repeat bypass. 8
As centers and operators gain experience, with the majority converting to an endovascular first as well as rescue approach, it is unclear whether patients will be in a position to undergo multiple attempts at surgical revascularization as outlined in this report. Although endovascular techniques will result in limb salvage in a number of patients, there are a substantial number of patients who will require a bypass and to whom this approach still applies. This report also underscores the importance of exercising therapeutic restraint when performing endovascular techniques so that inflow and/or outflow arteries are preserved should a subsequent bypass be required.
In summary, the likelihood of success of repetitive limb revascularization was unrelated to the number of previous failures and the expected incremental failure rate with each successive bypass was not found. These results, coupled with the three-year limb salvage rate of over 50% in patients who otherwise would have required amputation, lend support to aggressive use of repetitive limb revascularization in selected patients even after two or more failed bypasses.
Footnotes
Acknowledgments
Supported by a grant from the William J von Liebig Foundation.