
Abstract
There are greater than 120,000 above-knee amputations (AKA) and below-knee amputations (BKA) performed in the USA each year. Traditionally, general anesthesia (GA) was the preferred modality of anesthesia. The use of regional nerve blocks has recently gained popularity, however, without the supporting evidence of any mortality benefits. Our objective was to evaluate whether regional nerve blocks yield significant mortality reduction in major lower-extremity amputations. Retrospective data of both AKA and BKA procedures at the Maimonides Medical Center from 2005 to 2009 were analyzed. Patients received either general sedation, spinal or ultrasound-guided regional nerve blocks as per decision of the attending anesthesiologist. Regional nerve blocks for major lower-extremity amputations consisted of femoral, sciatic, saphenous and popliteal nerve blocks. A retrospective inquiry of 30-day mortality was performed with reference to the Social Security Death Index and hospital records. One hundred and fifty-eight patients were included in the study (82 men and 86 women with mean age of 74.5 years ± 12.9 SD, range of 33-98 years) of which 46 patients had regional nerve blocks and 112 had GA or spinal blocks. Patients who received both regional blocks and GA/spinal blocks within 30 days were excluded. The overall 30-day mortality was 17.1% (27 patients) consisting of 15.2% for regional nerve analgesia versus 17.9% for GA/spinal blocks (P = 0.867). Age did not affect mortality outcome in either groups of anesthesia modality. Our analysis did not reveal any mortality benefit of utilizing regional nerve block over GA or spinal blocks.
Introduction
Every year there are more than 120,000 major lower extremity amputations (MLEA) performed. 1 Many of these patients have extensive co-morbidities Thus, despite advances in perioperative management, postoperative mortality for MLEAs remain as high as 14% for below-knee amputations (BKA) and 30% for above-knee amputations (AKA).2-8 Recent approaches have been to experiment with different modalities of anesthesia provided during the procedure in hopes of reducing the postoperative mortality rate. One of such modalities is to provide regional nerve blocks. In regional nerve blocks, local anesthetics are provided via ultrasound-guided injection to the appropriate nerves. The localized delivery of anesthesia helps reduce the systemic effect experience with general anesthesia and minimize the depression of cardiopulmonary functions. There are numerous case reports across Europe, North America and Asia providing support for the use of regional nerve blocks in place of general anesthesia.9-11 While there is increasing interest in regional nerve block, there has not been any study comparing its efficacy to that of general anesthesia or spinal block.
We investigated the use of regional nerve block via a retrospective review of past major lower-extremity amputations examining how regional nerve analgesia may influence mortality risk of major lower-extremity amputations.
Methods
After obtaining institutional review board approval, a retrospective analysis was performed of all MLEAs performed between July 2005 and August 2009 at Maimonides Medical Center (Brooklyn, NY, USA). Non-elective cases and patients who received both regional blocks and general anesthesia or spinal blocks within 30 days were excluded from the study. Patient data were collected from hospital charts including demographics, pre-existing medical conditions, indications for surgery, laboratory results, perioperative data and outcome. A retrospective inquiry of 30-day mortality was performed with reference to the Social Security Death Index and hospital records. Perioperative date included anesthesia type, amputation type and side. The attending surgeon determined level of amputation with preoperative and intraoperative physical exam findings dictating choice of amputation level. The type of anesthesia provided was chosen by the attending anesthesiologist independent of amputation level – general sedation, spinal or ultrasound-guided regional nerve blocks. Those in the general anesthesia group received a balanced technique with opioids and inhalational anesthetics. Regional nerve blocks were provided via ultrasound-guided lidocaine injections to the femoral, sciatic, saphenous and popliteal nerves. Statistical analyses were performed using two-tailed Fisher's exact test. A P value of ≤0.05 is significant for all analyses.
Results
One hundred and fifty-eight procedures were included in the study (81 men and 77 women with mean age of 74.5 years ± 12.9 SD, range of 33-98 years). Of these procedures, 46 received regional nerve blocks, 27 received spinal blocks and 85 received general anesthesia. Most commonly associated co-morbidity was hypertension followed by diabetes mellitus and coronary artery disease. The patient demographics for each group are shown in Table 1.
Patient demographics
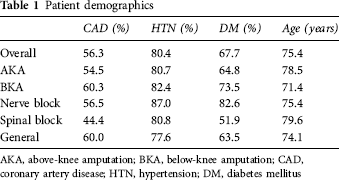
AKA, above-knee amputation; BKA, below knee amputation; CAD, coronary artery disease; HTN, hypertension; DM, diabetes mellitus
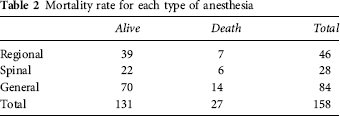
The overall 30-day mortality rate for all MLEAs was 17.1% (27 patients). Shown in Table 2, the mortality rate for regional nerve block, spinal block and general anesthesia was 15.2, 21.4 and 16.7%, respectively. Those who received regional nerve blocks had a 15.2% mortality rate versus a 17.9% mortality rate for those who received spinal blocks or general anesthesia (P = 0.8178). There were no significant differences in patient characteristics between those who received regional nerve blocks versus spinal block or general anesthesia. Furthermore, the two groups did not differ in terms of reason for amputation. Tables 3 and 4 illustrate how patient co-morbidity influences the comparison of regional nerve block with spinal block or general anesthesia.
Mortality rate for each type of anesthesia
Coronary artery disease (CAD) on mortality rate
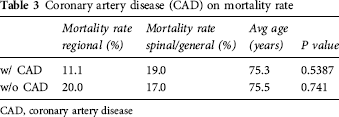
CAD, coronary artery disease
Diabetes mellitus on mortality rate
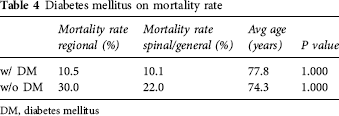
DM, diabetes mellitus
There were 69 BKA performed and 89 AKA performed. The 30-day mortality rate for BKA and AKA was 8.7 and 23.6%, respectively. Table 5 illustrates the 30-day perioperative mortality rate corresponding to each anesthesia modality. The numbers of spinal were too small and not significantly different from GA, and have been included with the results of GA (Table 6).
AKA and BKA mortality rate
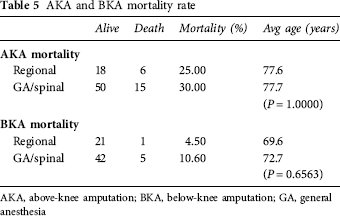
AKA, above-knee amputation; BKA, below-knee amputation; GA, general anesthesia
AKA and BKA mortality
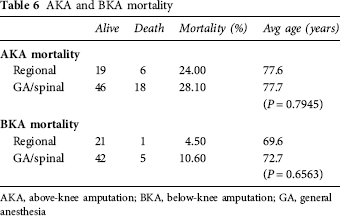
AKA, above-knee amputation; BKA, below-knee amputation; GA, general anesthesia
Discussion
The optimum management of patients undergoing surgical procedure is continuously being refined and experimented. We implement novel techniques in hope of improving upon the outcome of our patients. However, it is essential to thoroughly investigate new practices before widespread utilization.
During our investigation, we failed to demonstrate any significant mortality benefit of utilizing regional nerve block over general anesthesia or spinal blocks in major lower extremity amputations. This may be because mortality risks are contributed more significantly from patient's preoperative co-morbidity versus the type of anesthesia provided during the operation. Such hypothesis makes sense when considering that lower-extremity amputation procedures are typically done swiftly without any intraoperative complications. Therefore, blood loss for these procedures is minimal and exposure to prolonged cardiovascular depression is reduced. Furthermore, improvements in anesthesia monitoring have contributed greatly to the prevention of intraoperative risk. When we compare the mortality risk of spinal blocks to general anesthesia, it is consistent with previous reports of mixed mortality benefit in the spinal block versus general anesthesia groups.12,13
Although we did not demonstrate significant mortality benefits of utilizing regional nerve block over other modality of providing analgesia during the procedure, we did not examine other postoperative outcomes such as postoperative pain management. There has been recent support from Ong et al. 14 suggesting that spinal blocks may yield better postoperative pain control versus general anesthesia. This may also be true for regional nerve blocks as suggested by a report of improved pain management via catheter delivery of regional nerve analgesia. 15 We were not able to explore this issue in our data-set.
As we further examine the mortality benefits of regional nerve blocks in those with a history of coronary artery disease, we noted a trend towards decrease in mortality rate for those who received regional nerve blocks. While this was not statistically significant, this trend may suggest that those patients with a history of coronary artery disease are more vulnerable to the system effects of general anesthesia due to their decreased cardiopulmonary reserve. Therefore, we may better illustrate this trend by increasing the sample pool of future studies.
Of note, the retrospective nature of this study may have resulted in bias. Various anthesiologists may have preferred one type of anesthesia over another in certain patients. Although we were not able to detect significant differences between the groups, only randomized prospective data would be able to answer some of these issues.
In conclusion, our findings did not suggest any mortality benefit when using regional nerve blocks for major lower-extremity amputations. The additional time devoted to applying local anesthesia may not be justified solely on improvements in mortality risk.