
Abstract
Internal jugular vein (IJV) thrombosis is a rare entity. It is usually secondary to various etiologies such as ovarian hyperstimulation, deep vein thrombosis of upper limbs, venous catheter, malignancy, trauma, infection, and neck surgery and hypercoagulable status. We report an unusual case of internal jugular vein thrombosis with cerebral sinus thrombosis, postpartum in a 22-year-old female patient who presented with a painful swelling on the left side of her neck. Diagnosis was established by color Doppler ultrasonography and magnetic resonance venography. Thorough evaluation of the patient revealed no etiological factor leading to thrombosis. Patient was treated with low-molecular-weight heparin.
Introduction
Thrombosis of the internal jugular vein (IJV) is a relatively rare condition and associated with a variety of predisposing factors. IJV thrombosis presents with pain and swelling of the neck or face and presentation may be subtle at times. Regardless of the cause, the role of computed tomography, Doppler ultrasound and magnetic resonance imaging have been described for the diagnosis of IJV thrombosis. In the puerperium, it is rare to see cerebral sinus thrombosis with IJV thrombosis and we are reporting such a case.
Case report
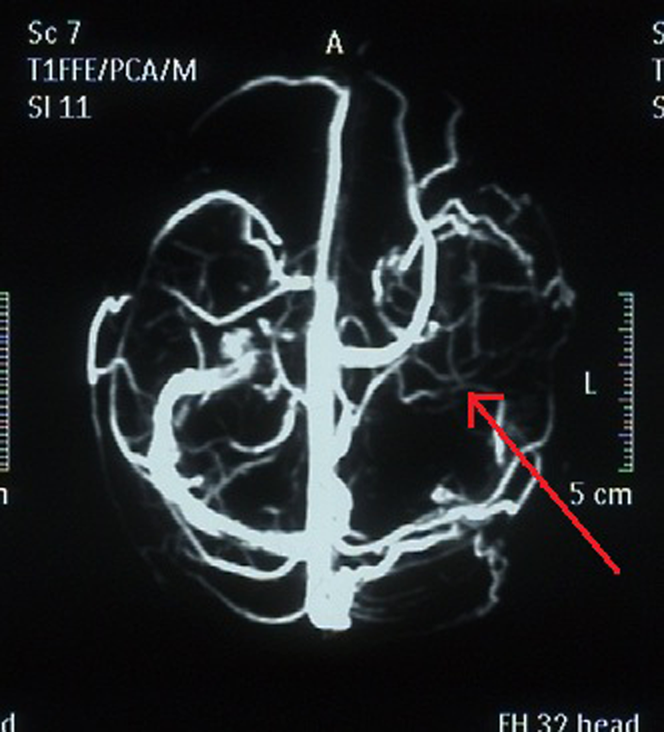
A 22-year-old women, weighing 45 kg, one month postpartum presented with gradually progressive pain and swelling in the left side of lower neck for 15 days. There was no history of calf pain, ovulation-stimulating drugs for pregnancy, use of oral contraceptives, previous neck surgery, any ear, nose, throat infection, previous menstrual irregularity, or any bleeding disorder. There was no history of headache, convulsions, stroke, and dizziness. Family history was non-contributory. She had one previous uneventful normal vaginal delivery. On examination her vital signs were with-in normal limits (temperature 37℃, pulse 86/minute, blood pressure 120/84 mmHg). There was a tender diffuse lower neck swelling on left side associated with restricted neck movements. Cervical lymph nodes were not palpable. The examination of rest of body was normal. Neck ultrasound scan showed a dilated non-compressible left jugular vein containing mixed echogenic thrombus with left cervical chain lymphadenopathy along IJV. Color Doppler flow scan showed absence of color flow in dilated left IJV and no wave pattern on spectral Doppler (Figure 1). Right IJV, bilateral common carotid artery, internal carotid artery, external carotid artery were normal. Color Doppler of lower limbs was normal. Abdominal and pelvic ultrasound were also normal. Hematological investigations revealed a hematocrit of 32%, white cell count of 8000/mm3, platelet of 2.5 lakh/mm3, and normal clotting and bleeding time, prothrombin time and activated patial thromboplastin time were normal as also the thyroid functions. Low-molecular-weight heparin (parnaparin) was started immediately with a dose of 7000 IU/day. Patient improved symptomatically. Magnetic resonance (MR) venography on fifth day revealed thrombosis in left sigmoid and transverse sinus with loss of signal void on T1W, T2W images (Figure 2). Low-molecular-weight heparin was given for three weeks and patient was switched over to nicoumalone 2 mg per day. Patent has completed two-month follow-up on oral anticoagulant 2 mg per day. Neck swelling has completely resolved without any pain and tenderness.
Color Doppler image showing thrombus in IJV (arrow) MR venography showing cerebral sinus thrombosis (arrow)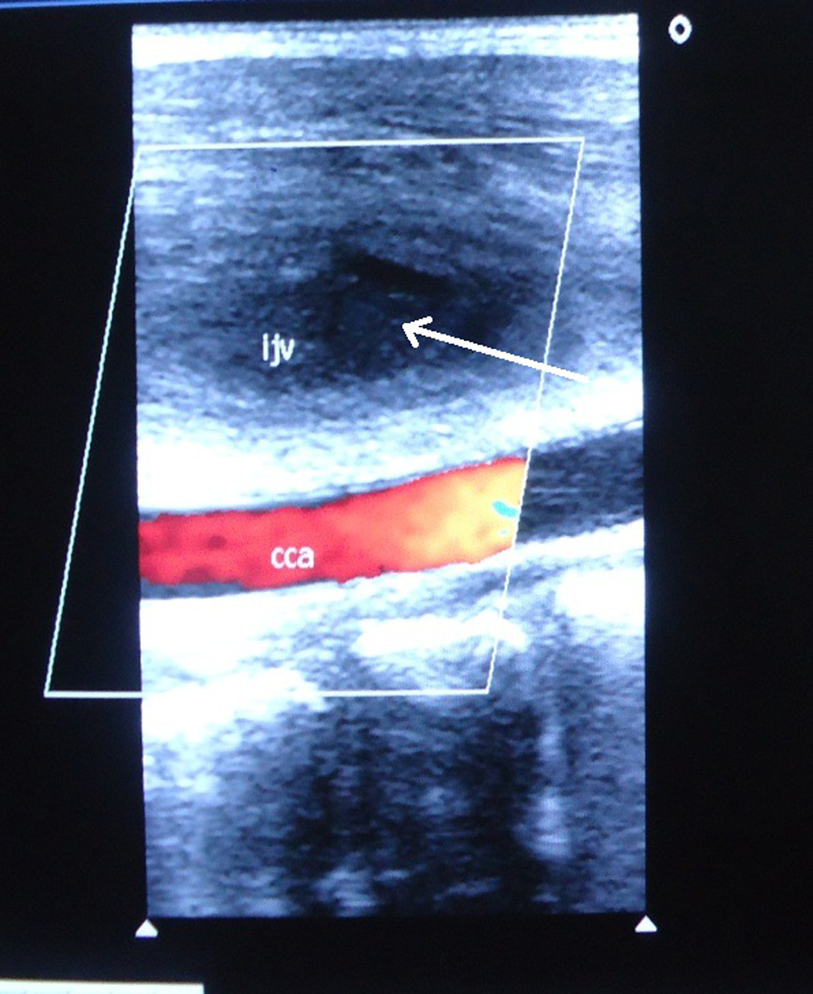
Discussion
Review of the literature showed most of the cases of internal jugular thrombosis to be associated with ovarian hyperstimulation syndrome (OHSS) after ovulation-stimulating drug.1,2 Many other causes of IJV thrombosis include complication of surgical procedures, presence of an indwelling venous catheter, tumor invasion, hypercoagulability, caudal extension of sigmoid sinus thrombosis, compression from adjacent tumor or nodes, a complication of adjacent infectious process, direct venous injection and after deep vein thrombosis of upper limbs.3–7 Most of the indwelling venous catheter thrombosis were associated with genetic risk factors for thrombophilia. Factor V Leiden was found to play the major role in these cases.8,9 Thrombophilic abnormalities like deficiency in antithrombin, proteins C and protein S (using functional and/or antigenic assays), factor V Leiden and prothrombin 202 10A mutations, primary antiphospholipid antibody syndrome are associated with increased risk of deep vein thrombosis.
Puerperium is itself a risk factor for venous thromboembolism. During pregnancy there are increased levels of most of the circulating clotting factors in preparation for placental separation. This increased level of clotting factors is a risk factor for thromboembolism.
Schanzer et al. 10 reported a case of IJV thrombosis in a patient with OHSS. Van den et al. 11 reported a case in a patient with malignancy (colorectal carcinoma). Simmers et al. 12 reported a case after neck traction. The literature is silent on such a case of postpartum internal jugular thrombosis associated with cerebral sinus thrombosis. Cerebral sinus thrombosis may manifest as simple headache, which is the most frequent but least specific symptom. Neurological signs like hemiparesis or aphasia may develop depending on the location of thrombus. Many patients present with behavioral symptoms like delirium, amnesia and mutism. Sometimes it may remain silent.
Imaging plays a major role in the diagnosis of internal jugular thrombosis. Color flow Doppler ultrasonography is highly sensitive and specific for the diagnosis of IJV thrombosis. 13 MR venography should be done to exclude cerebral sinus thrombosis whether cerebral symptoms are present or not. In the present patient there were no cerebral symptoms but on MR venography cerebral sinus thrombosis was detected.
In conclusion, internal jugular thrombosis may present as painful neck swelling. Color Doppler ultrasonography is the diagnostic modality of choice. Patients with spontaneous IJV thrombosis should be investigated thoroughly to exclude thrombophilia, hormonal disturbances, malignancy and cerebral sinus thrombosis.
Footnotes
Acknowledgements
No such support in the form of grants, equipment, drugs etc. were obtained for this case report.