
Abstract
The aim of the paper is to determine the incidence of celiac artery compression (CAC) based on computed tomography (CT) scan and correlate the findings to the clinical presentation of patients presenting for CT scan in a hospital. Abdominal CT scans of patients were reviewed between September 2010 and November 2010. CAC was diagnosed if the celiac axis appeared to have a hook or U-shaped appearance with stenosis. The medical records of the patients were reviewed for gastrointestinal symptoms (abdominal pain, nausea, vomiting, constipation, diarrhea), as well as food fear and weight loss. Patients with CAC had lower incidence of symptoms compared with those without CAC (42.1 versus 65.3%, P = 0.042). A total of 450 patients were evaluated. In the end, 284 had both complete medical records and CT scans. The mean age for all patients was 51.3 ± 1.2 years. There were 124 men (42.6%) and 160 (57.4%) women. Nineteen (6.7%) patients had radiological evidence of CAC. CAC is not an uncommon CT finding in patients presenting for CT scan.
Introduction
The celiac artery compression syndrome (CACS), otherwise known as Dunbar's syndrome, is a very controversial and much debated entity among vascular surgeons. Harjola et al. 1 was one of the first to describe such a syndrome and associate it with the compression of the celiac artery. The typical features of CACS include postprandial epigastric pain, food fear resulting in weight loss and epigastric bruit among others. While the syndrome is under debate, the existence of celiac artery compression (CAC) is, for the most part, accepted as a true pathology. CAC is thought to be caused by several mechanisms. Extrinsic compression is perhaps the most commonly discussed mechanism. Extrinsic compression may result from the celiac ganglion, surrounding fibrous tissue or from the median arcuate ligament (i.e. the median arcuate ligament syndrome). Rainer and Jiminez 2 published their findings in Boley's Vascular Disorders of the Intestine where they found ostial stenosis to be the cause of celiac occlusion in 86% of their 81 patients. Occlusion of the celiac artery may also be a consequence of less common factors such as compression from an enlarged pancreas (inflammation or tumor), tumor invasion, arterial tear and congenital etiology.3–7 Although the existence of celiac artery compression has been well documented, the causal relationship between CAC and the signs and symptoms of CACS remains unclear. We believe that radiological evidence of celiac artery compression does not necessarily result in the abdominal symptoms of CACS. Our study aims to investigate whether a clear association exists between the symptoms of CACS and CAC.
Methods
Our study was approved by the Institutional Review Board. During the months of September 2010–November 2010, all abdominal CT scans performed at the University of Toledo Medical Center were prospectively analyzed along with the patients’ medical records. All patients with CT scans and full medical records were included in this study. Patients whose CT scans did not clearly show the celiac trunk or did not have a complete medical record were excluded from the study. The CT scans were performed on a 64 slice Toshiba Aquillion CT scanner. In cases in which CT contrast was utilized, patients were given 80 ml of contrast. The patients were routinely asked to hold their breath at the end of inspiration. Longitudinal and cross-sectional views of the celiac, superior mesenteric and inferior mesenteric arteries were analyzed for compression, stenosis and/or calcification. If the celiac artery had a U-shape or hooked appearance on CT, it was considered to be compressed.8,9 The cross-sectional and longitudinal views of the arteries were visually inspected for areas of narrowing and calcification. Measurements of arterial diameter were taken at the point of narrowing and compared with the adjacent normal segment. Medical records at the time of presentation were reviewed. Data collection included abdominal pain and its characteristics, nausea, vomiting, diarrhea, food fear, weight loss, signs of malnutrition and epigastric bruit. The data were analyzed with SPSS version 17.
Results
Patient characteristics
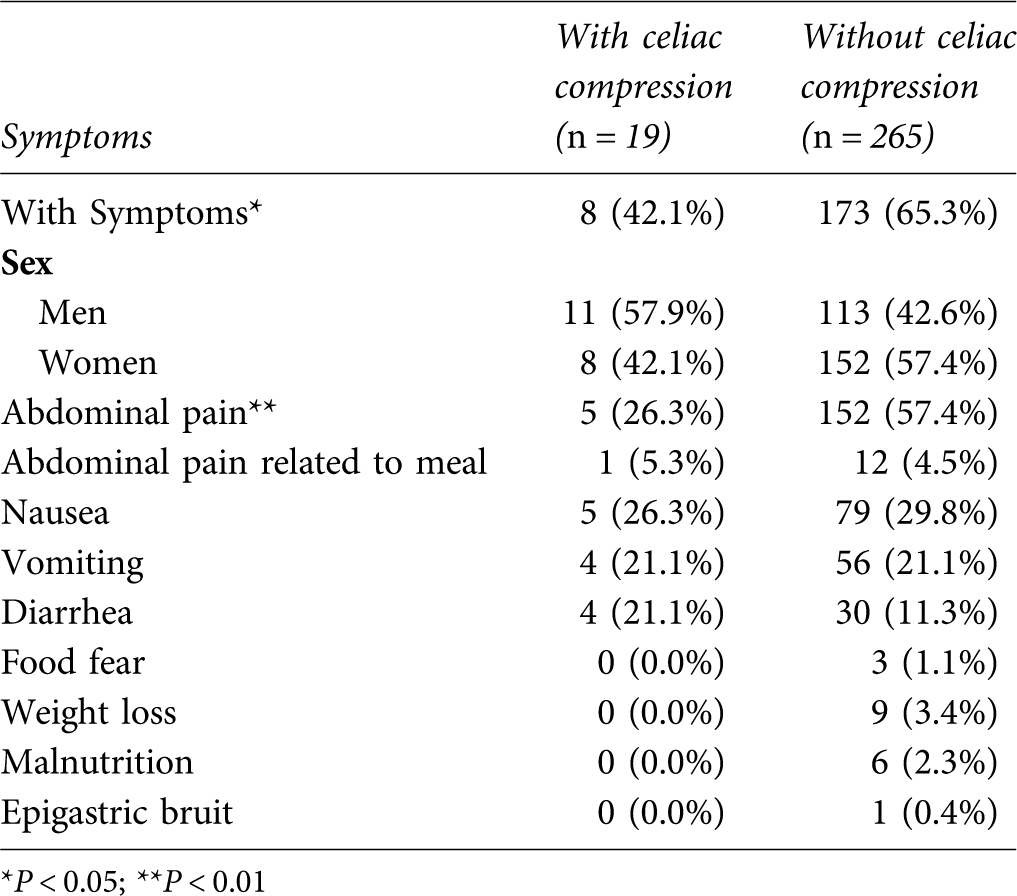
*P < 0.05; **P < 0.01

Graph signs and symptoms
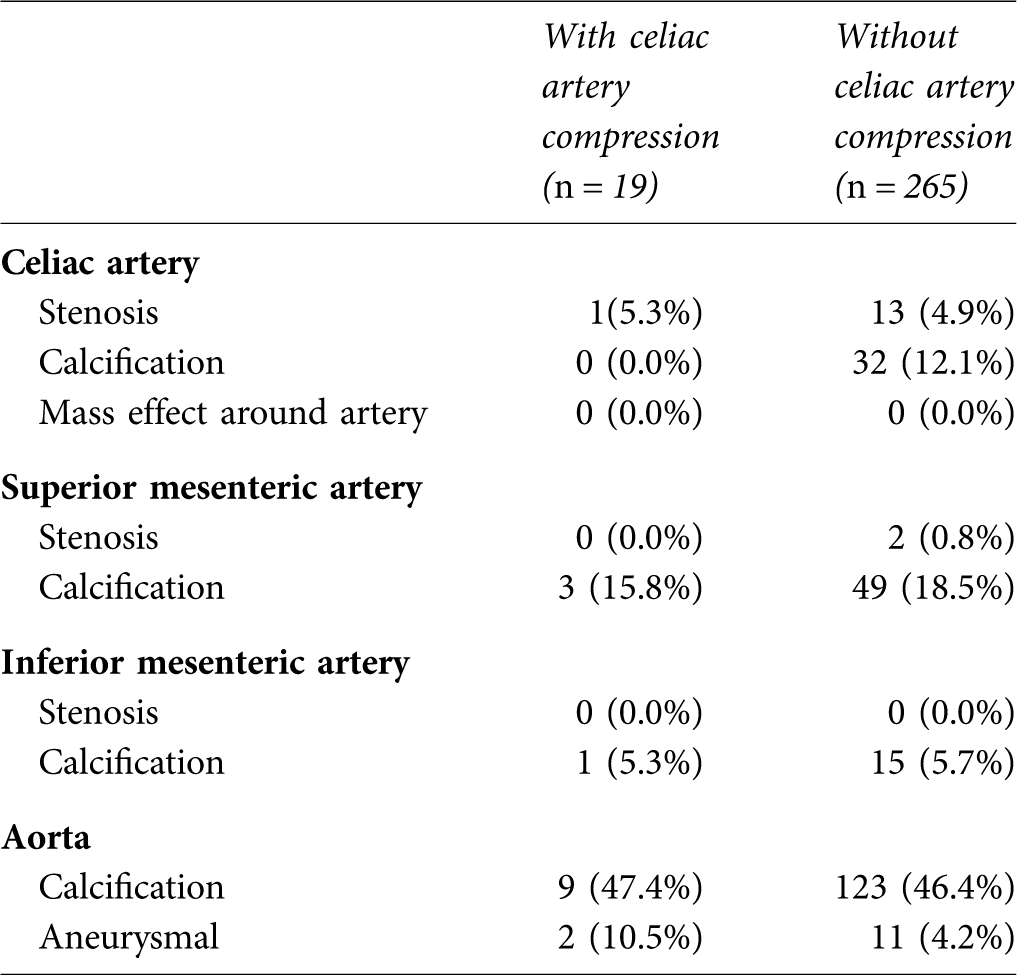
Incidence of other arterial abnormalities
Discussion
Celiac artery compression was first described by the anatomist Lipshutz in 1917 when he noted structures surrounding the celiac artery, such as the median arcuate ligament (MAL), compressing the artery at its origin in cadavers. 10 In 1957, Mikkelson 11 published a thorough and descriptive case of intestinal angina. It was not until 1963 that an association was made between CAC and the symptoms of CACS by Harjola. 1 He reported the case of a 57-year-old man with epigastric bruit who also experienced postprandial abdominal pain. The patient's celiac artery was found to be compressed by a fibrotic celiac ganglion that was surgically released and is the first published account in which the fibrotic celiac ganglion was divided to release the celiac axis compression. Harjola went on to write several papers documenting cases of abdominal angina and CAC throughout the 1960s.12–16 Dunbar et al. 17 at the Ohio State University reported 15 cases of CAC and abdominal angina. His descriptive account of CACS and treatment led to the alternative name of Dunbar's syndrome. Three years later, Lord et al. 18 also associated chronic CAC with stenosis.
In the literature, there has been a wide range of incidence reported for CAC. However, a range between 10 and 25% 19 appears to most accurately reflect the true incidence in the general population. In a selected group of patients presenting to the hospital, a review of CT scans in our patient population resulted in 6.7% (19 out of 284) incidence of CAC. Women have been reported to have a greater incidence of CAC than men.8,20 We did not have a significant difference in incidence between men and women in our study population; however, symptoms associated with CACS were reported by 116 (72.5%) women and 65 (52.4%) men. Patients without CACS-related signs or symptoms were found to have a higher incidence of CAC on CT scan (10.7%) than those with symptoms (4.4%, P = 0.042). The majority of our patients underwent abdominal CT (Figures 2 and 3) for evaluation of abdominal symptoms such as nausea, vomiting, etc. A small number were found to have renal colic, or were being evaluated for non-related causes such as renal transplant surgery. The most characteristic symptoms of CACS (postprandial pain, food fear, weight loss, malnutrition and abdominal bruit) were found to exist less frequently compared with the more general abdominal complaints such as nausea, vomiting and diarrhea. As such, the symptomatic patients in this study may not be comparable with the patients suspected of having CACS in the literature and may be considered a weakness of this study. In 1972, Levin et al. 8 sought to study the incidence of CAC in 50 patients free of symptoms that were randomly selected. These patients underwent abdominal angiography for reasons not associated with abdominal pain or gastrointestinal tract symptoms. Two films were taken of the aorta after dye was injected above the celiac axis and respiration was held after full expiration. The patients with more than 50% stenosis were considered to have celiac artery narrowing. Their patient population consisted of 20 men and 30 women ranging in age from 21 to 77 years. Of the 50 patients studied, 12 (24%) had a narrowing of their celiac axis of at least 50%. Only one of 12 had an epigastric bruit and only three had collateral vessels from the SMA to the celiac axis. Other authors report similar results.21,22 These results correlate well with our findings and prove that CAC/narrowing may be more prevalent in the general population. The presence of CAC does rarely lead to symptoms and to the development of CACS.
The association between CAC and clinical symptoms has been doubted by a number of authors. One of the most outspoken critics, Szilagyi et al. 19 reviewed 165 surgically treated cases by a total of 26 various authors. They found fault in many of these reports as not enough relevant information was collected as well as the lack of agreement in their diagnostic and treatment strategies. Furthermore, they highlighted the short follow-up periods averaging only 20 months. They reviewed over 200,000 hospital records at their own institution Henry Ford Hospital in Detroit, Michigan and could not find one case of CACS that was properly documented. The researchers also randomly selected 157 cases and evaluated the patients’ abdominal arteriograms (performed either by transfemoral catheters or by translumbar aortography) taken between 1 October 1970 and 30 June 1971. They studied the lateral view of the celiac artery and determined celiac artery narrowing by measuring the diameter of the celiac artery at the point of narrowing. A discussion included in the article among several other surgeons did include opposing opinions and experiences.
The gold standard for diagnosing CACS, especially by external compression, continues to be lateral aortic angiography. CAC appears in lateral aortograms with the artery having a hooked or U-shaped appearance.8,9 CT angiograms in combination with three-dimensional (3D) reconstruction are capable of projecting the same anatomical information as conventional angiography.
23
Multidetector computed tomography (MDCT) scans with 16 and 64 slices are capable of providing exact imaging.
9
The imaging for our study utilized 64 slice MDCT scans with the patient's respiration suspended at the end inspiratory phase. Studies performed in the 1970s24,25 proved that the MAL, celiac artery and aorta vary in their positions during respiratory cycle. Compression of the celiac artery is most visible during expiration. Lee et al.
26
studied a total of 100 patients undergoing magnetic resonance imaging (MRI) of the upper abdomen. Patients were divided into two groups consisting of 50 patients each. One group had an MRI taken at end expiration and the other at end inspiration with venous phase acquisitions done during the opposite phase of respiration. The radiological studies were reviewed by two blinded radiologists that were instructed to group the patients according to the degree of stenosis into five groups (none, minimal 1–20%, mild 20–40% mild to moderate 40–60%, moderate 60–80% and severe >80%). In their patient population, 55 patients (57%) had a minimum mild artery narrowing at end expiration. Out of the 55 patients, 40 (73%) had less narrowing at the end of the inspiratory phase while 11 (20%) had no change. The angle of the aorta in patients found to have mild to severe celiac artery narrowing was lower (41° ± 19°) than in those classified as having minimal to no narrowing (50° ± 19°). The authors concluded that it was best to perform these imaging studies at the end of inspiration in order to properly identify CAC so as to not misdiagnose. In 1973, Reuter and Bernstein
25
published a paper in which surgical clips were placed at the free edge of the MAL of eight patients. The researchers then studied the movement of these clips during respiration via fluoroscopy. These studies revealed that the celiac artery, the MAL, as well as the aorta moved downward during inspiration and upward in expiration. As a result, the MAL and celiac artery moved closer together during expiration, thus exaggerating the degree of CAC. Images taken during suspension of breathing at end expiration most accentuates the compression of the celiac artery
24
and allows for a clear picture unhindered by the breathing movements.
26
Although opinions vary, all seem to agree that CAC appears more clearly at end-expiration. The evidence published by Lee convincingly favors studying the celiac artery axis at the end of inspiration. Furthermore, acquiring images at the end of inspiration will decrease false-positive diagnosis.
External compression of the celiac artery as seen on computed tomography (white asterisk) External compression of the celiac axis (indicated by arrow)

Other techniques have also been shown to be useful in diagnosing CAC such as spiral CT angiography, Doppler US, selective catheter angiography, MRA,24–26 and gastric exercise tonometry.23,27,28 Kopecky et al. 29 reported a case in which spiral CT was used to identify CAC after catheter angiography failed to reveal it in two of their patients. In 2003, Wolfman et al. 30 published a case report in which duplex and color flow ultrasound were used to evaluate the velocities of the celiac arteries during inspiration, expiration and in the erect position of two patients. Bech 31 also greatly supported the use of duplex ultrasound for realtime imaging of the celiac axis through the respiratory cycle. Selective catheter angiography was utilized by Cina and Safar 32 to diagnose CAC in their case report published in 2002. MRI by Lee 26 has been detailed in the previous section. Gastric exercise tonometry was utilized by Otte 27 and Mensink 28 to more effectively determine the best candidates for celiac decompression. In their experience, stenosis was detected with an accuracy of 86%. Except for the latter method of diagnosis, radiological tests lack the ability to correlate the presence of external compression and its potential of producing the clinical symptoms.
In 1967 Harjola 12 published a paper describing the surgical intervention of 13 patients (10 women and 3 men). All 13 patients complained of crampy abdominal pain manifesting between 20 minutes and one hour postprandially and each were found to have an epigastric bruit upon auscultation. Stenosis of the celiac artery was verified by aortography. Patients were grouped into three main categories depending on the etiology of the compression. The first category had eight patients in whom the celiac ganglion was constricting the celiac artery. The second group had four patients with the esophageal hiatus compressing the celiac axis into a loop. The third and last group consisted of only one patient that had constriction of the artery by the celiac ganglion and of the axis by the aortic hiatus. All surgeries involved surgical release of the celiac artery and/or axis. Patients were followed up for anywhere between six months to four years. Of the 13 treated patients, nine remained asymptomatic throughout the follow-up period, three complained of mild epigastric pain, and one experienced no improvement at all. Dunbar et al. 17 reported their experience in 1965 surgically treating patients with CAC. Their patient population consisted of 15 patients found to have CAC after more common causes were ruled out. The article reported a follow-up of 15 months for one case and a period of more than nine months for all the other cases. Out of the 15 patients, 13 were surgically treated to decompress the celiac trunk. The 12 women and one man were reported to have complete alleviation of their abdominal pain following surgical intervention.
Minimally invasive decompression has been described in celiac artery decompression. Laparoscopic decompression of the celiac axis was first published by Roayaie et al. 33 as a case study in 2000. More recent accounts of minimally invasive procedures have been published since then.34–37 Roseborough 37 published a case series in 2009 in which 15 patients with CAC underwent laparoscopic decompression of the celiac axis. The patients ranged in age from 20 to 61 years (median age of 40.6 years) and included 13 women and two men. The procedures were all performed by the same surgeon. The first procedure mimicked that of a case report previously published in which the gastroesophageal junction was mobilized followed by exposure of the aorta (from the aortic hiatus to the celiac axis) and concluded with crural repair. Subsequent intervention spared the dissection of the aortic hiatus as well as crural repair, thereby greatly decreasing operative time and preventing the development of gastroesophageal reflux. Of the 15 patients, four were converted to open surgery after unintentional arterial injury. Patients underwent a thorough work-up in order to rule out other possible underlying gastrointestinal causes. Of the 15 patients treated by laparoscopy, one was considered to be a clinical failure as his symptoms were refractory to treatment. Another patient reported an improvement in symptoms; however, the patient complained of a mild constant pain. Furthermore, additional stenting of the celiac artery in four of the patients was done due to their persistent symptoms following the laparoscopic procedure. Other researchers such as Vaziri et al. 38 have also reported success in laparoscopic decompression of the celiac artery. Their group treated three women aged 37, 47 and 49 after extensive work-up ruled out other possible causes and contrast CT and MRI revealed celiac compression. Following intervention, two of the three women reported complete alleviation of symptoms while one had improvement of her symptoms with persistent pain. Duplex ultrasound of the three women performed within six months postintervention showed normal velocities in their celiac arteries. Van Petersen et al. 34 described their novel retroperitoneal endoscopic technique in 46 of their patients. Of the 46 patients, 41 experienced resolution or improvement of their symptoms during a median follow-up period of 20 months.
Conclusion
Celiac artery compression has been a long debated entity. It has been described in the literature as early as 1917 and became associated with symptoms in the 1960s. The causal relationship between compression of the celiac artery axis and the symptoms which comprise the CACS has been a controversial topic. Many theories exist as to the underlying etiology of the gastrointestinal symptoms experienced by patients found to have compression of the celiac artery. Various diagnostic modalities have been shown to be effective in identifying the compression and surgeons have developed minimally invasive techniques to treat their patients. Although the existence of celiac artery compression has been well published in the literature, its existence is infrequently associated with symptoms. Coexisting abdominal symptoms usually are not typical for gastrointestinal ischemia in that weight loss and postprandial pain are usually absent. Only one research group used a function test (gastric tonometry) to confirm functional gastrointestinal impairment. In our study CAC by CT scan was present in 6.7% of patients with little association with clinical symptoms indicating that CAC is more of a radiological finding than a clinical syndrome.