
Abstract
Atherosclerosis, the main cause of heart attack and stroke, is the leading cause of death in most modern countries. Preventing clinical events depends on a better understanding of the mechanism of atherosclerotic plaque destabilization. Our knowledge on the characteristics of vulnerable plaques in humans has grown past decades. Histological studies have provided a precise definition of high-risk lesions and novel imaging methods for human atherosclerotic plaque characterization have made significant progress. However the pathological mechanisms leading from stable lesions to the formation of vulnerable plaques remain uncertain and the related clinical events are unpredictable. An animal model mimicking human plaque destablization is required as well as an in vivo imaging method to assess and monitor atherosclerosis progression. Magnetic resonance imaging (MRI) is increasingly used for in vivo assessment of atherosclerotic plaques in the human carotids. MRI provides well-characterized morphological and functional features of human atherosclerotic plaque which can be also assessed in animal models. This review summarizes the most common species used as animal models for experimental atherosclerosis, the techniques to induce atherosclerosis and to obtain vulnerable plaques, together with the role of MRI for monitoring atherosclerotic plaques in animals.
Keywords
Introduction
Cardiovascular disease is widely recognized as the leading cause of morbidity and mortality in developed countries and is predicted to become the predominant disease worldwide in the near future. 1 Atherosclerosis is the most important single factor contributing to this disease. 2 Evolution of atherosclerotic plaque can lead to advanced lesions causing severe stenosis or to atherothrombosis upon plaque rupture. The precise mechanisms at play in atherosclerotic plaque progression are yet to be fully understood. One solution to this major public health problem is improving the prevention, screening and treatment. Better understanding of the underlying causes and mechanisms that lead to the development of vulnerable plaque and clinical events are essential while technological innovations for diagnosis and treatment are still needed.
Histological features of vulnerable plaque are now well described in human coronary and carotid arteries.3–5 Recent development of morphological and functional imaging improved our knowledge of vulnerable plaque. Imaging techniques allowing precise characterization of human atherosclerotic plaque in vivo such as magnetic resonance imaging (MRI) are available. 6
These human observations provide insights into the state of plaque evolution but remain limited for ethical reasons and are insufficient to understand the mechanisms leading up to plaque rupture, emboli or thrombosis. Cell culture is essential to try to elucidate specific signalling pathways, but is inadequate to reproduce the conditions of the disease in vivo. Animal models in which the pathophysiology of atherosclerosis can be reproduced are an established alternative to cell culture and are routinely used in preclinical research settings.
The ideal animal model of vulnerable plaque should develop advanced atherosclerosis lesions similar to those seen in humans, eventually leading to clinical events (myocardial infarction or stroke) in a reasonable time-frame. Atherosclerotic plaque development in preclinical animal models should be monitored with the same diagnostic tools that are used clinically.
In this current review we will present the different techniques to induce atherosclerosis in an animal model, the different animal models of vulnerable plaque and survey the MRI methods used to monitor the time course of the developing pathology.
Search methods
An electronic literature search of the US National Library of Medicine public domain database (MEDLINE) was performed for articles published from 1950 to present using the following keywords: animal models, mice, rabbit, pig, atherosclerosis, vulnerable plaque, MRI. The references of the retrieved articles were also manually searched for any additional relevant articles. These articles were supplemented with textbooks of animal models, atherosclerosis and imaging methods.
Part I. Animal models of atherosclerosis
Animal models of atherosclerosis started emerging in the literature at the beginning of the 20th century with rabbits being the first animal species to be described. Subsequently, a wide variety of birds, primates and non-primates (rodent, pig, dog, etc.) were characterized and since the 1990s transgenic strains of mice, rabbits and rats have been developed. Initially, studies focused on morphology, physiology and underlying causes of atherosclerosis. For a long period of time, animal models were developed to try to resolve technical intervention issues such as re-stenosis. Currently, most studies focus on the vulnerable plaque. Since many characteristics of the animal models are prescribed by the aim of the research, a large number of animal models have been reported. Our review will focus on animal models of atherosclerosis commonly used to study the evolution of atherosclerosis and the vulnerable plaque.
The choice of animal species
Experimental models of atherosclerosis are required to understand the natural history of the disease and the factors leading to plaque progression/rupture. Susceptibility to atherosclerosis varies not only between animal species but also between genetic strains within the same species. The ideal animal model does not exist, but it is critical that models mimic the human disease as closely as possible.
Animal models must meet a few general criteria such as size, docility, ease of handling, ease of breeding and housing, known genetic profile, analogies with humans (anatomic, physiological, metabolic and pathophysiological), reliable homologies with human diseases and cost.7–9 In addition to those criteria, animal models of atherosclerosis should present a progressive development of arterial lesions throughout life, from initial fatty streak to advanced complicated lesions (ulceration, thrombus, etc.) with shared histological features, and clinical events (myocardial infarction, stroke) similar to humans.10–12
Advantages and drawbacks of the most widely used non-primate mammal species for atherosclerosis model
CETP, cholesteryl ester transfer protein
Mice
Although mice do not develop spontaneous atherosclerosis, it is the most commonly used animal species to study the disease. Among all strains, the C57BL/6 mouse is currently the most used background to develop genetically modified atherosclerosis models, as it is also the most susceptible strain to diet-induced atherosclerosis. 13 The majority of mouse models are based on disturbance of lipid metabolism through genetic manipulation from the C57BL/6 strain. Among those, the ApoE − / − mouse is the most distributed worldwide. Arterial lesions observed in ApoE − / − are similar to lesions found in humans: from foam cell rich fatty streaks to atheroma with large necrotic core, and fibro-fatty nodules. The most advanced lesions have been described to be located in the innominate artery (brachiocephalic trunk). 14 Luminal thromboses are uncommon in Apo E − / − mice because of a spontaneous high fibrinolytic activity. Mice have a low level of plasma plasminogen activator inhibitor-1 and thrombin-activated fibrinolysis inhibitor.15–17
However, mouse models present major disadvantages. Firstly, mice are naturally resistant to atherosclerosis progression and therefore advanced genetic manipulation is required. 18 In addition, the lipid profile and metabolism are not similar to humans. Mice have high plasma levels of high-density lipoprotein (HDL) cholesterol and the cholesteryl ester transfer protein (CETP) is absent. 19 One other major limitation of transgenic mouse models is the non-physiological high expression level of hypercholesterolemia, which may not be similar to the more frequent human pathological form. 20 Also, the small size of the animal makes blood sampling as well as dissection of the vessels difficult. Moreover the size of the arteries makes it extremely difficult to image with sufficient resolution in clinical scanners used for humans, precluding the efficient translation of techniques from animal model to human scanning.
Rabbit
Rabbit models of atherosclerosis have also been widely described. Being herbivorous, the rabbit is not inherently prone to the development of atherosclerosis. Among all rabbit strains, the New Zealand White (NZW) is commonly used. 21 Rabbits have low total cholesterol concentration in the plasma, and HDL is the predominant lipoprotein. 22 Similarly to humans, Apo A-II is absent and hepatic lipase activity is low.23,24 These animals show Apo B levels and high CETP activity comparable to humans.23,25,26 The NZW rabbit rarely shows spontaneous lesions and induction of vascular lesions necessitates high-fat high-cholesterol diet.11,27
The NZW also serves as a background for two genetically altered rabbit models: the Watanabe Heritable Hyper Lipidemic (WHHL) rabbit and the St Thomas’ Hospital strains, which present genetic abnormalities in their lipid metabolism.28,29 The WHHL rabbits develop spontaneous hypercholesterolemia and atherosclerosis at five months of age. These rabbits have an abnormal low-density lipoprotein (LDL) receptor responsible for pathological changes in cholesterol metabolism, leading to atherosclerosis development.11,30
The St Thomas’ Hospital rabbits have a familial dysbeta-lipoproteinemia responsible for an overproduction of VLDL and LDL. They have xanthomatous arterial lesions similar to those of species subject to atherogenic diets. 31
Transgenic rabbits are widely distributed. The different models of hyperlipidemia have been created to study atherosclerosis and its correlation with lipid metabolism.32–34
Microscopically, the lesions observed are thick fatty streaks with most of the lipid localized within the foam cells. Advanced lesions such as fibrosis, hemorrhage, ulceration and thrombosis are rarely observed. Lesions are preferentially localized in the aorta, iliac and coronary arteries.
One major advantage of this model is the animal's size: small (easy to feed, care for, handle and inexpensive) but large enough to monitor physiological changes. Imaging techniques such as ultrasound (US) or MRI can be effectively applied to determine the plaque composition and its vulnerability.35,36
One limitation of this animal model remains the absence of hepatic lipase and the lack of Human Apo A-II. Arterial lesions observed are more fatty and macrophage-rich compared with human plaques and also differ in location. 37
Pig and mini-pig
With the requirement to obtain close-to-clinical models, large animal models, such as the mini-pigs have become increasingly popular. 38 However, many options have been described and the best model is still a matter of debate.
Available evidence indicates that the pig is an optimal model for atherosclerosis because of the many important similarities with humans. The pig genome is highly similar to humans. Its chromosome structure is comparable to that found in humans. 39 The similarity with humans in cardiovascular anatomy and physiology,40–42 in lipid profile and lipoprotein metabolism have also been demonstrated. 43 In addition, arterial structure and its response to hypercholesterolemia and platelet aggregation resembles humans. 44 Moreover, unlike mice, rabbits or rats, pigs develop spontaneous atherosclerosis. 19 Lesions observed are characterized by necrotic cores, calcification, neovascularization and intraplaque hemorrhage (IPH) that closely mimics advanced human atherosclerosis.45,46 Atherosclerotic lesions are preferentially localized in the aorta, coronary and iliac arteries.
The major drawback of the domestic pig model of atherosclerosis is its large size resulting in management difficulties. To overcome this limitation, development of downsized pig and mini-pigs resulting from selection and crossing between different strains has been described. Different strains of mini-pigs such as Yucatan, Hanford, Göttingen, Sinclair Hormel and Ossabaw are already in use for preclinical research in atherosclerosis. These animals present different susceptibility to diet-induced hypercholesterolemia, as well as to accelerated atherosclerosis development; differences are observed between strains and often in the same strain.47,48 Among published studies, very few accurately described the origin of mini-pig strains and their corresponding lipoprotein profile. 12
Recently, a down-sized pig model was obtained by a crossing between a Rapacz farm pig (R84C LDL receptor mutation) a smaller pig (Chinese Meishan) and a French minipig. 49 Even more recently a novel micro-minipig model of atherosclerosis was described in Japan, illustrating the growing importance of the minipig model. 50
Others animal models have been developed using avian, hamster, guinea pigs, rats and non-human primates.
Strategies to induce experimental atherosclerosis in animal models
Only few animals spontaneously develop atherosclerosis and often these lesions are rare, not advanced and not similar to those seen in humans. 19 Moreover, they require a long time, typically many years, to develop. An experimental atherogenesis strategy is necessary. To approach the ‘ideal’ model, the intervention should lead to the development of atherosclerosis lesions similar to those seen in humans, and in a reasonable time frame of a few months.
Atherogenesis involves many systemic factors, such as hypertension, hyperlipidemia, diabetes mellitus and smoking. 51 Local hemodynamic perturbations or ‘traumatic’ factors are also implicated. We will summarize the two main categories of inducing accelerated atherosclerosis: systemic or local intervention.
Systemic intervention
The systemic intervention approach is dominated by atherogenic diets, which are described among the major risk factors of atherogenesis. This results in hyperlipidemia (hypercholesterolemia and hypertriglyceridemia), diabetes mellitus (hyperglycemia) or metabolic syndrome depending on the diet composition and the individual susceptibility.
The role of hypercholesterolemia (LDL-Cholesterol) in atherogenesis is well established.
2
A strong association between certain types of dyslipidemia including hypercholesterolemia, hypertrygliceridemia, and combined hyperlipidemia and the development of atherosclerotic lesions has been documented by numerous clinical trials, as well as epidemiological and experimental studies. High cholesterol and high-fat diets lead to atherosclerosis lesions development in mice, rabbit and pig. However results of numerous studies report that stable high LDL cholesterol plasma level is not easily reproducible even with the same animal species and with the same diet. There are qualitative differences of the atherogenecity of various dietary fats.
52
Coconut oil is more atherogenic than other saturated, non-saturated and polyunsaturated fats.
53
The modified diet called the Paigen diet, the most used for mouse models, contains 50% sucrose, 15% fat, 1% cholesterol and 0.5% cholic acid.
54
Diabetes is a well-recognized independent risk factor of atherosclerosis.55,56 Diabetes can be induced by sugar-enriched diet to maintain constant and regular hyperglycemia or by injection of β-cell cytotoxic chemicals resulting in a greater than 80% reduction in β-cells and an increase in plasma glucose, such as with streptozotocin or alloxan.43,57,58 The dose of these agents required for inducing diabetes depends on the animal species, route of administration and nutritional status. Diabetes mellitus combined with a diet-induced hypercholesterolemia leads to increased development of atherosclerosis lesions compared with hypercholesterolemia alone.43,58
Metabolic syndrome (hypertension or HTA, associated to diabetes, dyslipidemia and/or obesity) is known to accelerate atherosclerosis lesions in human.
59
It has been reported in Ossabaw pigs with HF/HC diet.12,60,61 Unfortunately, induction of atherosclerosis lesions was disappointing.
Hypertension is clearly associated with an increased risk of cardiovascular diseases and accelerated atherosclerosis. Sekhara Rao and co-workers
62
demonstrated that Carneau pigeons selected for increased blood pressure are more susceptible to moderate hypercholesterolemia acting as a stimulus for atherosclerosis progression. Sugiyama et al.
63
reported an acceleration of atherosclerotic lesions in transgenic mice with hypertension by the activated renin–angiotensin system. Hypertension can be induced in mice by Angiotensin II injection,64,65 Deoxycorticosterone acetate salt administration,
66
or clipping of the renal artery.
67
Such models have also been developed in rabbits.68,69
Others risk factors like tobacco or stress were studied but none of these solely led to a reproducible animal model of atherosclerosis.
70
General infection seems to be involved in atherogenesis related to inflammatory and immunological reaction. Chlamydia pneumoniae, Helicobacter pylori, Cytomegalovirus, herpes simplex virus, Streptococcus sanguis and Porphyromonas gingivalis have been detected in human atheroma. Many models have been proposed with intravenous inoculation.71,72
Local intervention
The creation of local lesions is proposed by many authors to accelerate atherosclerosis development. Even if theses kinds of models are not completely representative of spontaneous atherosclerosis, they reduce the time required for the development of advanced plaques as well as the associated costs. Another advantage is the possibility to increase the total number of available lesions and pick their location.
There are two main approaches for local intervention: direct arterial injury or indirect mechanism reproducing hemodynamic conditions favourable for atherosclerosis development.
Endothelial denudation by balloon injury: Different methods are described. The most used and described is the endothelial denudation with a balloon injury. Experimental studies in various animal models have consistently shown that arterial wall injury leads to smooth muscle cell proliferation and migration into the intima that eventually provokes luminal stenosis and thrombosis.73–76 However, lesion progression is characterized by fibrosis and rather stable lesions on histology. Balloon injury leads to smooth muscle cell proliferation in the intima with formation of extracellular matrix in response to mechanical intimal-to-medial injury in virtually any site within the vascular tree in any species.
11
This approach was primarily designed for the re-stenosis experimental model.
44
A combined injury induced by balloon angioplasty in the setting of hypercholesterolemia causes both intimal smooth muscle cell proliferation and intense macrophage infiltration in the intima, media and adventitia, with severe impairment of endothelial vasodilator function resulting in atherosclerotic lesions.
Endothelial denudation can be performed with compliant or not compliant balloons and can be associated with medial injury. With concomitant dietary hypercholesterolemia, more advanced atherosclerotic lesions can be observed.77,78 According to Thim, 78 degree of injury seemed easier to control with non-compliant balloon injury compared with compliant balloon.
Drawbacks of this method are the rate of acute arterial thrombotic occlusion and the inability to analysis disease progression. It has been proposed that endothelial dysfunction plays a role in initiating atherosclerosis through alterations in expression of adhesion factors and inflammatory mediators. 79 More recently Turk et al. 80 in a high-fat cholesterol diet-induced porcine model report that early stage disease development may precede the development of endothelial dysfunction. However, because of the disruptive nature of mechanical injury, the role of endothelial function has been difficult to assess.
Others types of injury: Other localized vascular injuries have been proposed to accelerate atherosclerosis formation: external radiation, 81 electric injury,82,83 thermal balloon injury, 84 photochemical injury and cold injury.85,86
Intramural delivery of lipids has also been proposed to initiate the process of atherosclerotic disease.87,88
Although the entire vasculature is exposed to the atherogenic effect of systemic risk factors, atherosclerotic lesions form at specific regions of the arterial tree: near bifurcations, bends and branch ostia. Local hemodynamic factors, in particular low endothelial shear stress, play a fundamental role in the localization of atherosclerotic plaques.89–91 Cheng et al.
92
report large variations in absolute wall shear stress levels along the arterial tree within one species and between species. Wall shear stress is inversely related to the vessel diameter.
Reproduction of these hemodynamic perturbations in animal models exposed to systemic factors (hypercholesteremia, diabetes, hypertension) leads to the acceleration of atherosclerosis. Different techniques have been proposed.
Vein graft: The purpose of this technique was to understand aortocoronary vein graft bypass failure.93–97 Rapid atherosclerosis observed in vein bypass leading to thrombosis was not similar to atherosclerosis observed in the arteries. Vein graft atherosclerotic lesions are more diffuse, concentric and friable with a poorly developed or absent fibrous cap, whereas native vessel atheroma are proximal, focal, eccentric and non-friable with a well-developed fibrous cap.98,99 Accelerated atherosclerotic lesions contain more foam cells with varying degrees of lipid accumulation and macrophage/mononuclear and inflammatory cell infiltration than native atherosclerotic lesions. 100 Therefore, vein graft is not a good model for human arterial atherosclerosis.
The blood flow cessation model with a total ligation of the artery: This model consists of total ligation of the common carotid artery near the bifurcation in the mouse model.101,102 It is characterized by rapid and reproducible arterial remodelling with the development of significant intimal thickening. The lesions observed consist of intimal hyperplasia. Such models seem to be interesting in arterial remodelling analysis.
Partial ligation of the artery: This model consists of partial ligation of a straight arterial segment inducing hemodynamic perturbation. Ishii et al.103,104 described this model in the common carotid artery of Yucatan mini-pigs also undergoing a high-fat diet. They obtained advanced atherosclerotic lesions comparable to those observed in humans.
Stenosis collar: Perivascular collar placement offers the advantage of maintaining the structural integrity of the endothelium while inducing rapid, site-controlled lesion formation.105–108 The neointima observed within the collar is generally fibroproliferative, with limited foam cell formation and extracellular lipid deposition.109–111
Cholesterol feeding or local (oxidized) LDL application in conjunction with the placement of a perivascular Silastic collar has been shown to promote the development of more atherosclerosis-like lesions in the rabbit carotid artery and more recently in LDL r − / − mice.90,106,107,112
Atherosclerosis induced by ligation or stenosis collar can also be explained by local ischemia secondary to the adventitial vasa vasorum occlusion, direct media injury resulting in smooth muscle cell proliferation and migration to the intima, local inflammatory reaction and endothelial NO synthesis inhibition.
In our opinion, the ideal technique to induce atherosclerosis similar to humans is the systemic approach, which exposes the animals to well known risk factors. However, the level of exposure and development of hyperlipidemia and hyperglycemia should be as close as possible to the levels observed in humans. The major limitation of this approach is the time necessary to obtain atherosclerosis, particularly advanced lesions. The major drawback of the local intervention approach is the direct disruption of the arterial wall leading to difficulties interpreting the resulting lesions and the underlying causes of the normal lesion etiology. Reproduction of the hemodynamic conditions leading up to atherogenesis appears to be the best method, accelerating atherosclerosis development without direct mechanical endothelial injury.
Part II. Animal models of vulnerable plaque
Human vulnerable plaque
Human vulnerable plaque is an atherosclerotic plaque prone to rupture, thrombosis and emboli leading to the occurrence of cardiovascular events. Coronary and carotid vulnerable plaques have been extensively described through histopathological analysis and autopsic studies.3–5
Morphological criteria of human vulnerable plaque are the following:
Large lipid rich-necrotic core associated with thin fibrous cap; Intraplaque hemorrhage; Fibrous cap rupture; Plaque ulceration; Inflammation with the presence of macrophages. Develop atherosclerotic plaque and look for spontaneous complications; Develop atherosclerotic plaque and induce a complication.
The underlying mechanisms of plaque vulnerability remain unknown. Preclinical animal models are essential to improve our understanding of the processes that influence the development of vulnerable plaque. There are two ways to develop such animal models of advanced atherosclerotic lesions:
Animal models of induced vulnerable plaque
This approach ignores the complexity of the mechanism of destabilization. They are rather models of rupture and athero-thrombosis than models of vulnerable plaque. After atherosclerotic plaque has been obtained, different methods are available to induce advanced lesions.
Pharmacological triggering with procoagulant Russel's viper venom and vasopressor histamine (Constantinides model)
This method was developed by Constantinides 40 years ago. 113 Intraperitoneal injection of Russel's viper venom (RVV) (procoagulant with endothelial toxin) followed by intravenous injection of histamine (vasopressor) in high-fat diet rabbits led to plaque rupture and thrombosis. This model was reproduced by Abela and Chen.114,115 Nakamura used serotonin or angiotensin II combined with RVV. 116 Plaque rupture and luminal thrombosis are frequently observed and resemble human lesions. However the triggering process is not physiological and does not reproduce human pathophysiology.
Direct mechanical injury to plaques
Plaque rupture can be obtained by inflating an angioplasty balloon into the plaques or by directly squeezing the plaques with forceps.117–119 Cold induced endothelial injury, 86 perivascular electrical injury 120 or radiation are also described to obtain vulnerable plaque in NZW Rabbits.121,122 Erythrocyte injection into existing plaque has been reported to lead to vulnerable plaque.123,124 Increased lipid content and augmentation of oxidative stress and inflammation in the plaque are the probable pathological mechanisms.
Such models are complex to perform, far from human physiology and expensive.
Histological analysis of arterial lesions that have been induced by pharmacological or mechanical intervention is difficult to interpret.
Transgenic destabilization of atherosclerotic plaque
Some studies propose a transgenic approach to promote plaque destabilization using inflammatory or apoptosis effects. Gene transfection has been reported directly in atherosclerotic plaque with the p53 gene or the MMP-9 gene or in systematic transfection with the IL-18 gene.106,125,126
These models are complex, expensive and difficult to reproduce.
Exposure to stress
Rekther et al. 127 induced a central stress by intracerebral injection of corticotropin releasing factor in ApoE − / − mice. They observed plaque rupture and thrombosis. The signal pathway involved remains unknown.
Exposure to hypertension or Angiotensin II
Mazzolai et al. 128 showed that Angiotensin II, beyond its hemodynamic effect, modulates the atherosclerotic phenotype from stable to vulnerable in ApoE − / − mice.
Exposure to a modified wall shear stress
Ishii et al. 103 reported an animal model of vulnerable carotid atherosclerotic plaque. Carotid atherosclerotic models were performed in Yucatan mini-pigs by using a combination of partial ligation and high cholesterol diet. Typical features of vulnerable plaque (necrotic core with thin fibrous cap, IPH) were observed three months after surgery. Distal embolism in rete mirabile were identified and correlated with advanced plaques.
Cheng et al.90,129 obtained vulnerable plaque with a constrictive collar around carotid arteries in ApoE − / − mice.
Animal models of spontaneous vulnerable plaque
Animal models of spontaneous vulnerable plaque
IPH, intraplaque hemorrhage
Transgenic mice models of spontaneous vulnerable plaque
Rosenfeld et al. 130 described advanced lesions in the innominate artery of chow-fed Apo E − / − mice aged 42–54 weeks. Advanced arterial lesions were characterized by large necrotic core, fibrotic conversion of necrotic zones accompanied by loss of the fibrous cap and calcifications. A high frequency of IPH was observed. The hemorrhage occurs at all stages of atherosclerosis and leads to fissures of lateral fatty streaks that form adjacent to or on top of the established plaques. There was no plaque rupture as observed in human lesions (rupture of a well formed fibrous cap) but rather plaque disruption (fissures of fatty streak). Moreover, no thrombus was observed in association with this disruption while occlusive thrombus is the predominant marker of plaque rupture in human lesions. This model has to be considered as a model for studying vascular fibrosis and calcification and not for studying vulnerable plaque. Johnson and Jackson have also reported advanced lesions in the innominate arteries of Apo E − / − mice fed a high-fat high-cholesterol diet which died after 46 ± 3 weeks (range 37–59). 131 They report a high frequency of IPH associated with plaque rupture and luminal thrombus formation. The plaque rupture was characterized by fragmentation and loss of elastin in the fibrous cap of relatively small and lipid-rich plaques overlying large complex lesions.132–134 According to Jackson and in contrary to the Rosenfeld hypothesis, this is a model for studying events leading to plaque rupture in humans. 135 Other mice models of advanced atherosclerotic plaque have been published with the low-density lipoprotein deficient mouse (LDL R(−/−)). LDL R(−/−) mice under a high-fat diet present similar lesions in the innominate arteries in size and composition to those described by Rosenfeld in chow fed Apo E −/− mice. 136
Calara et al. 137 reported, in 2001, IPH, deep plaque ruptures (or erosions reaching necrotic core areas) and large thrombus originating from the core of a disrupted atherosclerotic lesion in aorta and coronary arteries of Apo E (−/−) and LDL R (−/−) mice (9–20 months old). Lesions were rare and the frequent absence of a clearly defined single fibrous cap limits their usefulness as a model of fibrous cap rupture.
Large-animal models of spontaneous vulnerable plaque
Advanced atherosclerotic lesions were reported in a female rhesus monkey with spontaneous hypercholesterolemia related to a genetically determined LDL receptor deficiency which died at 22 years of age. 138 Lesions observed were multifocal in the aorta and coronary arteries and were characterized by heavy lipid deposition, fibrous cap, necrotic core, fibrinogen/fibrin in plaques and spontaneous rupture. This animal model published in 1993 has never been reproduced.
Prescott et al.45,46 reported advanced atherosclerotic lesions similar to those found in humans in inherited hypercholesterolemia pigs at 39–54 months. Lesions were observed in coronary, iliac and femoral arteries and were characterized by fibrous cap, necrotic core, IPH, neovascularization, plaque rupture and rare luminal thrombosis. Necrotic core and eccentricity of lesions are very similar to those observed in humans, but media destruction is less pronounced. Gerrity et al. 58 developed a pig model (Yorkshire) of advanced atherosclerotic lesions in coronary, femoral arteries and aorta with hypercholesterolemia induced by high-fat diet and diabetes induced by intravenous injection of the β cell cytotoxin streptozotocin. Advanced lesions occurred in a relatively short time (9 months) and were characterized by fibroatheroma, IPH and severe calcifications. No rupture and no luminal thrombosis were described. Chatzizisis et al. 89 reproduced this model with success. The time necessary to obtain lesions and the rapid growth and size of the domestic pig limit the use of these models (90–120 kg at six months; adult body weight > 300 kg). To overcome size-related problems, models of spontaneous vulnerable atherosclerotic plaque in downsized, mini or micropigs are under development. Thim 78 recently generated a mini-pig with familial hypercholesterolemia by crossing the Rapacz pig (inherited hypercholesterolemia pigs) with a smaller pig and then with an even smaller mini-pig. After 18 weeks of atherogenic diet, body weights were between 30 and 50 kg. Spontaneous atherosclerotic lesions were found at 18 weeks in the proximal segments of the coronary arteries. These lesions were typically eccentric and characterized by necrotic core, thin and inflamed fibrous cap, IPH, expansive remodelling and calcifications. However plaque rupture or luminal thrombosis was not observed.
Part III. MRI and animal models of atherosclerosis
Post mortem histological analysis of atherosclerotic plaque in animal models is fundamental to validate the model and remains the gold standard. However, one of the major endpoints of animal models is to obtain a better knowledge of the mechanism of destabilization of the atherosclerotic plaque. Thus direct visualization of plaque in situ and in vivo over time could bring valuable insights into the processes involved.
Morphological and functional imaging of atherosclerotic plaques in animals must satisfy many constraints. These constraints are related to the animals themselves: the need for anesthesia, the difficulty of handling (animal size and weight) and the size and location of the arteries in question in relation to the geometry and sensitivity of the imaging coils available to achieve the necessary spatial resolution to characterize the lesion.
MRI: the imaging modality of choice in atherosclerosis assessment
Different non-invasive imaging modalities to evaluate atherosclerosis in animal models have been described. Ultrasound imaging techniques have been widely used for atherosclerotic plaque detection in the animal models of atherosclerosis. Recent advances with contrast enhanced techniques allow detection of neovascularization in atherosclerotic plaque.139,140 Determination of plaque composition is based on tissue echogenecity. However precise plaque characterization (lipid core, intraplaque hemorrhage or fibrous cap rupture) is not possible. Image acquisition is complex and operator dependent.
The use of computed tomography (CT) has also been described in this field. The main advantages of CT include its high spatial resolution and short scan time but its major disadvantage for atherosclerotic plaque characterization is the limited discrimination of soft tissue. Micro and nano-CT allow higher spatial resolution but are limited for in vivo imaging. 141 Recent experimental studies on animal models of atherosclerosis using CT report fused CT and positron emission tomography (with 18F Fluoro deoxyglucose [18FDG]) imaging which gives anatomic and metabolic assessement of atherosclerotic plaque.142,143
MRI is well known to be a reliable tool for the analysis of atherosclerotic components in human carotid arteries.144,145 It allows precise description of plaque: lipid-rich-necrotic core, fibrous cap, calcification and fibrosis. Vulnerability criteria such as ulceration, cap rupture and IPH are also easily identifiable. Furthermore, contrast agents (gadolinium, USPIO) give information on the inflammatory activity and the presence of macrophages in the plaque. In brief, the main advantages of MRI include its high spatial resolution, great soft-tissue contrast, lack of radiation exposure, good clinical translatability and the ability to combine functional, anatomic and molecular information. Moreover, anesthesia can be performed with continuous gas inhalation through a mask without invasive maneuver and without close monitoring allowing a long scan time. Thus MRI is well-suited to monitor atherosclerotic plaque formation and destabilization in preclinical animal models.
Morphological imaging: atherosclerotic plaque composition
Several authors have already used MRI to study atherosclerotic lesions in animal models, such as mice, rabbit or pig. Skinner et al. 146 have demonstrated the usefulness of high resolution MRI to show atherosclerosis progression and to determine composition of atherosclerotic lesions in the rabbit abdominal aorta. Fayad et al. 147 developed a non-invasive MR microscopy technique to study in vivo atherosclerotic lesions in ApoE −/− mice with an excellent correlation between MRI and histopathology. Another study demonstrates aneurysm development over atherosclerotic lesions in the abdominal aorta of ApoE −/− mice. 148 Helft et al. 149 used in vivo MRI to quantify atherosclerotic components in the thoracic and abdominal aorta of rabbits. There was a significant correlation for plaque composition (P < 0.05) between MRI and histopathology for the analysis of lipidic and fibrous components. Johnstone et al. 150 reported in vivo MRI of thrombus formation after pharmacological triggering of plaque disruption in the modified Constantinides rabbit model of plaque disruption. MRI data correlated with the histopathology regarding aortic wall thickness (R = 0.77, P < 0.0005), thrombus size (R = 0.82, P < 0.0001), thrombus length (R = 0.86, P < 0.005) and anatomic location (R = 0.98, P < 0.0001). More recently Phinikaridou et al. 151 demonstrated that in vivo MRI at 3.0 T detects features of vulnerable plaques in NZW rabbits aorta. It has been also demonstrated that MRI is a useful tool in pig models to determine arterial wall thickness and area, wall hematoma and thrombus in carotid and coronary atherosclerotic lesions.152–155
Intraplaque neovascularization and inflammation can also be assessed with gadolinium enhanced MRI in animal models.152,156,157 Furthermore, the ability of dynamic contrast enhanced (DCE) MRI to detect neovessels has recently been reported in atherosclerotic lesions of rabbit abdominal aorta.158,159 DCE-MRI consists in repeated MRI acquisitions of the same imaging slice/volume serially with high temporal resolution after the injection of a Gd-based contrast agent.
Molecular imaging
In addition to morphological characterization obtained with MRI, several novel molecular enhancers have been developed in animal models targeting different cells, molecules and biological process which allow a more detailed characterization of biological process at play in atherosclerosis. Molecular targets for macrophages, elastin, fibrin and HDL have been tested in animal models. Ultra-small iron oxide particle enhanced MRI has been developed for macrophage imaging in animal models of atherosclerosis with a good correlation with histology.35,160,161 MRI of coronary wall using an elastin-binging contrast agent in a swine model of coronary atherosclerosis has been recently reported. 162 The authors demonstrated the ability of this agent to detect and quantify the vascular remodeling. Botnar et al. 163 demonstrated the feasibility of in vivo molecular MRI for the detection of acute and subacute thrombosis using a fibrin-binding MRI contrast agent in an animal model of atherosclerosis. HDL-based MRI contrast agent in atherosclerotic mice have been also reported. 164 This contrast agent which enhances macrophage-rich areas of atherosclerotic plaque allows a more detailed plaque composition description.
Multimodality and functional imaging
Myeloperoxidase, a central inflammatory enzyme secreted by activated macrophages is involved in multiple stages of plaque destabilization in human atherosclerotic plaques. 165
A myelopreoxydase-activatable contrast agent has been reported in atherosclerotic rabbits with a good histological correlation with myeloperoxidase-rich areas infiltrated by macrophages. 166
Promising combined MR-PET (18F Fluoro deoxyglucose) is under development. By combining the excellent anatomical (MRI) with functional information (PET), these advancements may allow a more comprehensive and accurate quantification of inflammation in atherosclerotic plaques.
Imaging of plaque biomechanics
Analysis of biomechanical features of atherosclerotic plaques revealed the role played in atherosclerotic plaque development and destabilization. MRI with specific sequences can provide information on flow velocity and wall shear stress in the arterial tree. Thus, some authors report the use of MRI to assess the biomechanical process of atherosclerosis development in animal models of atherosclerosis induced by partial ligation or stenosis collar.167–170
Technical aspects
Vessel wall MRI imaging in these animal models requires high spatial resolution and high signal-to-noise ratio and with minimal acquisition time. The luminal diameter and the wall thickness of the mouse aorta are around 0.5 mm and 40–200 μm (Figure 1). Visualization of such small features requires very high field strength magnets, high-spatial and temporal resolution three-dimensional imaging, respiratory and cardiac gating and continuous anesthesia administration to allow longer imaging. A number of groups have developed high-field MRI microscopy studies of atherosclerosis in mice at 9.4 and 17.6 T,147,171,172 and at 4.7 and 7 T.
173
Magnetic resonance imaging and animal models of atherosclerosis. (a) Mouse aorta (Apo E−/−), internal diameter = 0.5 mm and arterial wall thickness = 40–200 μm. (b) Rabbit aorta (Watanabe), internal diameter = 5 mm and arterial wall thickness = 0.4–1.3 mm. (c) Minipigs carotid artery, internal diameter = 6 mm and arterial wall thickness = 1 mm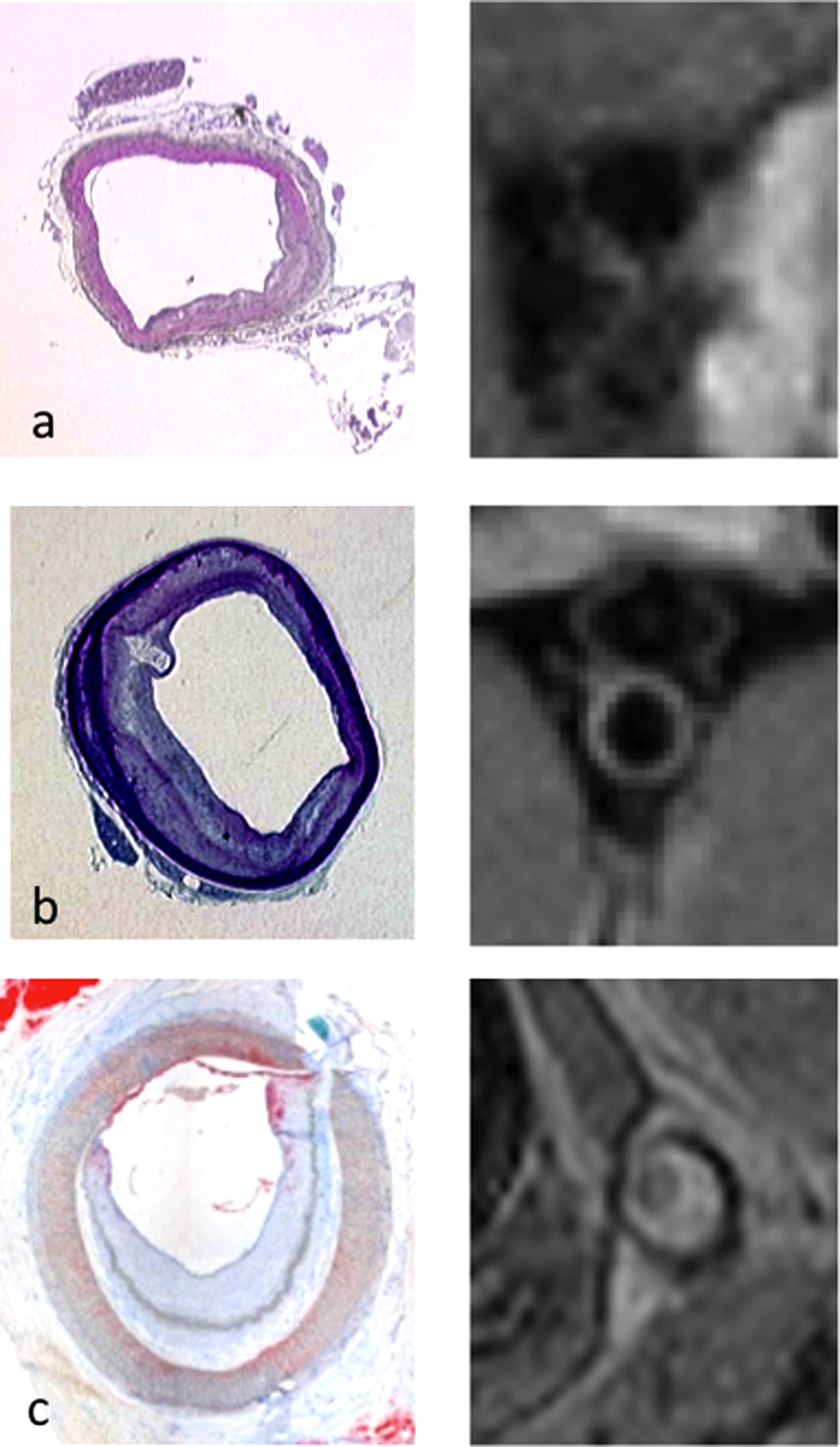
The use of rabbit or pig models, with their larger arteries, has permitted the use of clinical MRI imagers (1.5 or 3 Tesla), which are more readily available and allow for translation of imaging protocols to studies in humans (Figure 1).
Future directions
Vulnerable atherosclerotic plaques are responsible for triggering critical cardiovascular events. Clinical imaging of patients can provide much useful information, for example the identification of the lipid-rich necrotic core, and we have gained much knowledge from such studies in humans, but imaging of the development of disease from the early stages of stable plaque through the time the plaque becomes vulnerable and presents with clinical events is lacking and it is hard to imagine such a study. In vivo imaging studies of animal models of atherosclerosis provide valuable opportunities to investigate the pathophysiological etiology of plaque. The non-invasive nature of many imaging modalities, particularly MRI, allows frequent assessment enabling intensive monitoring of plaque formation and progression, and may provide critical information on the processes involved in vulnerable plaque development and rupture. Going forward, in both preclinical and clinical settings, the combination of multiple imaging modalities, including high resolution MRI, PET, duplex US and biological markers may be useful and complementary tools in the understanding of vulnerable atherosclerosis and cardiovascular disease.