
Abstract
Thoracic aortic mural thrombus (TAMT) is a rare pathology and potential source of cerebral, visceral, and peripheral emboli. We present a 62-year-old male in a hypercoagulable state due to primary polycythemia vera (PV) developed TAMT and catastrophic thromboembolisms despite aggressive medical and surgical management. The outcomes and adverse events of endovascular exclusion of TAMT in the presence of PV are unknown. We would recommend proceeding with extreme caution when performing endovascular exclusion of TAMT, as PV may be a prohibitive risk.
Introduction
Thoracic aortic mural thrombus (TAMT) is a rare pathology and potential source of cerebral, visceral, and peripheral emboli.1–3 Due to the rarity, there are no treatment guidelines for, or a consensus on the management of TAMT. Endovascular exclusion with thoracic stent graft (SG) has been recently suggested as an alternative treatment for TAMT with promising short-term outcomes. We present an unusual case with primary polycythemia vera (PV) complicated by TAMT.
Case report
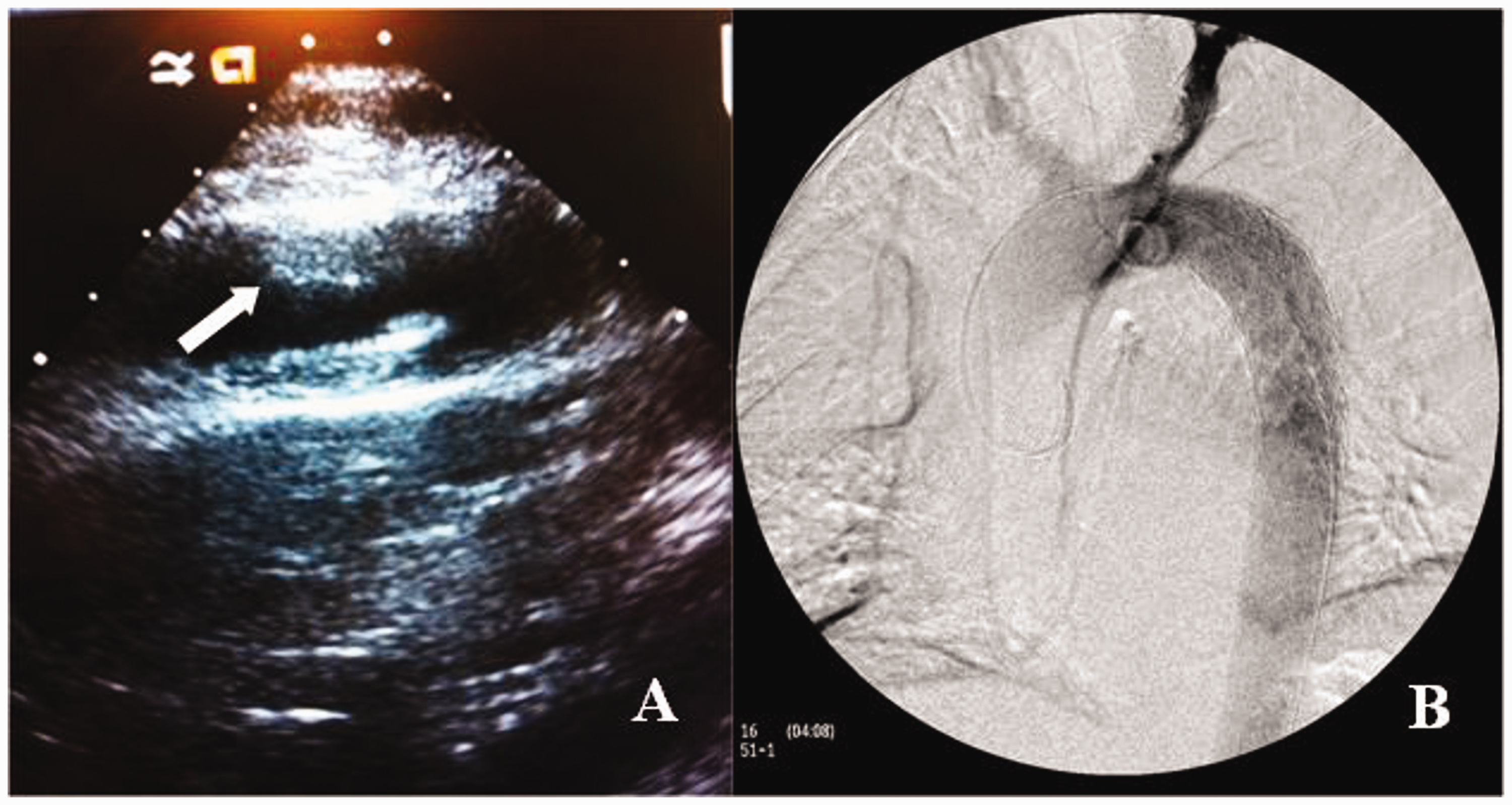
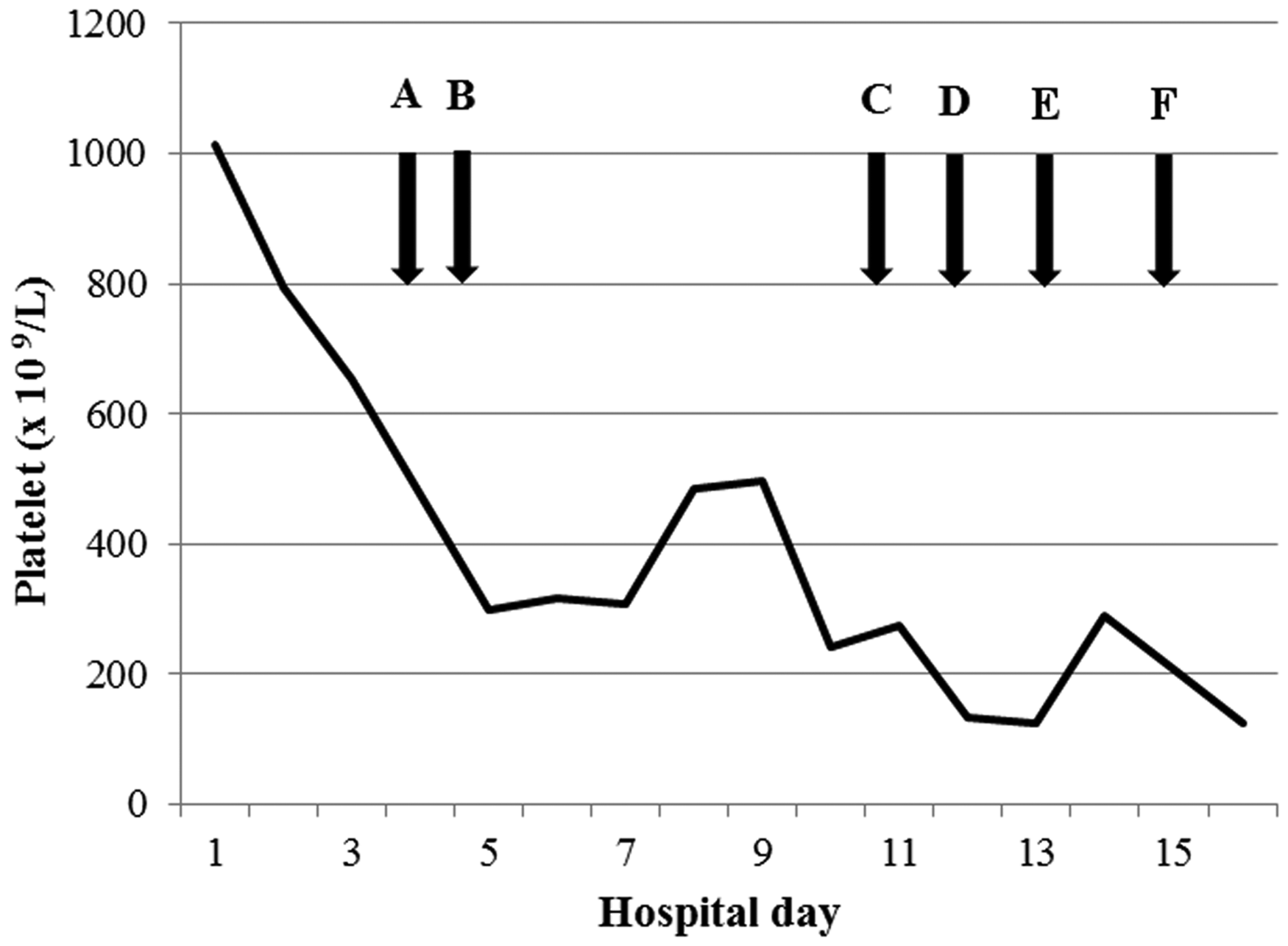
A 62-year-old male with primary PV and systemic mastocytosis under maintenance therapy with aspirin and steroids, presented with right leg ischemia. Vascular exam revealed palpable femoral and popliteal artery pulses, and non-palpable but biphasic Dopplerable posterior tibial and dorsalis pedis artery. Computed tomography scan revealed a focal filling defect in the distal aortic arch measured 1.6 × 1.6 × 1.1 cm consistent with a focal thrombus (Figure 1), and a non-occlusive filling defect within the right common femoral artery. There were no aortic wall calcifications, irregularities, or aneurysms. His white blood cell (WBC) and platelet count were 44.3 and 1013 × 109/L, respectively. The coagulation profiles were within normal limits except for the slightly elevated fibrinogen of 554 mg/dL. His electrocardiogram revealed normal sinus rhythm. Further workup included a transthoracic echocardiogram which revealed no evidence of intracardiac thrombus with normal left and right ventricular size and function without any structural abnormalities. Phlebotomy, hydroxyurea, and systemic heparin were initiated. Nevertheless, his symptoms progressed with appearance of more prominently mottled right foot with loss of the distal Doppler signals. On the third hospital day, he was taken to the operating room. A bidirectional thrombectomy through the right common femoral artery was performed and tan-pink organizing fibrosed material was removed. Intraoperative transesophageal echocardiography (TEE) did not show intracardiac tumor or thrombus. After confirmation of frozen section of this material, which did not show any evidence of aortic wall neoplasm, a thoracic aortic SG (GORE TAG 2.8 × 15 cm) was deployed immediately distal to the origin of the left subclavian artery. A completion angiogram showed good positioning of the SG with exclusion of thrombus (Figure 2(b)). Anticoagulation and maintenance therapies for PV were resumed postoperatively. On the first postoperative day, partial paralysis of the bilateral lower extremities occurred. Spinal cord ischemia (SCI) was suspected and the mean arterial pressure was augmented by phenylephrine to greater than 90 mmHg. Cerebrospinal drain was immediately inserted postoperatively. Over the course of the treatment and rehabilitation, significant neurological recovery was achieved. He was able to stand and walk with assistance. Anticoagulation was maintained by switching heparin to warfarin. On the seventh postoperative day, he suddenly developed acute rest pain of the left leg with ischemic appearance of the foot and absence of peripheral pulses, despite his therapeutic prothrombin time/international normalized ratio of 2.3. The platelet count was 235 × 109/L, which was one-fifth of the admission baseline (Figure 3). Disseminated intravascular coagulation was unlikely given the increased fibrinogen levels as well as the minimal rise in D-dimer. Argatroban was empirically started suspecting heparin-induced thrombocytopenia (HIT), although subsequently sent serotonin release assays had been consistently negative. Other laboratory values revealed protein C and S activities of 123% (75–133) and 62% (52–151), and antithrombin III activity of 82% (81–113). In addition, factor V Leiden mutation analysis and antiphospholipid antibody panel were both negative. An emergently performed selective angiogram showed a complete occlusion of the left popliteal artery, which was thrombectomized through popliteal cut down. Simultaneously, it was noted that his right leg and left arm were ischemic. Subsequent angiograms revealed right popliteal and left brachial artery occlusion, which were also thrombectomized. Intraoperative TEE did not reveal any evidence of thrombus in the left-sided cardiac chambers or the thoracic aorta. Six hours later, he suddenly developed diffuse abdominal pain, which required an emergent exploratory laparotomy. Although the superior mesenteric artery pulses were intact, a segment of ischemic ileum was identified and resected with primary anastomosis. After laparotomy, he became comatose and a head CT revealed diffuse ischemic anoxic injury, which eventually caused diffuse cerebral edema with herniation. The patient expired thereafter, 5 days after the abdominal surgery and 12 days after his original intervention. The family declined to have an autopsy performed.
Computed tomography scan of the chest revealed a filling defect measured 1.6 × 1.6 × 1.1 cm in the non-atherosclerotic, non-aneurysmal distal aortic arch consistent with a focal thrombus: (a) axial view and (b) coronal view. (a) Intraoperative transesophageal echocardiogram showing a non-mobile sessile thrombus (arrow) and (b) an angiogram demonstrates the stent graft (GORE TAG 15 × 2.8 cm) implanted right distal to the origin of the left subclavian artery. Platelet count and hospital course: (a) endovascular exclusion of the aortic thrombus, (b) spinal ischemia, (c) thromboembolic events of all extremities, (d) mesenteric ischemia, (e) cerebral ischemia, and (f) death.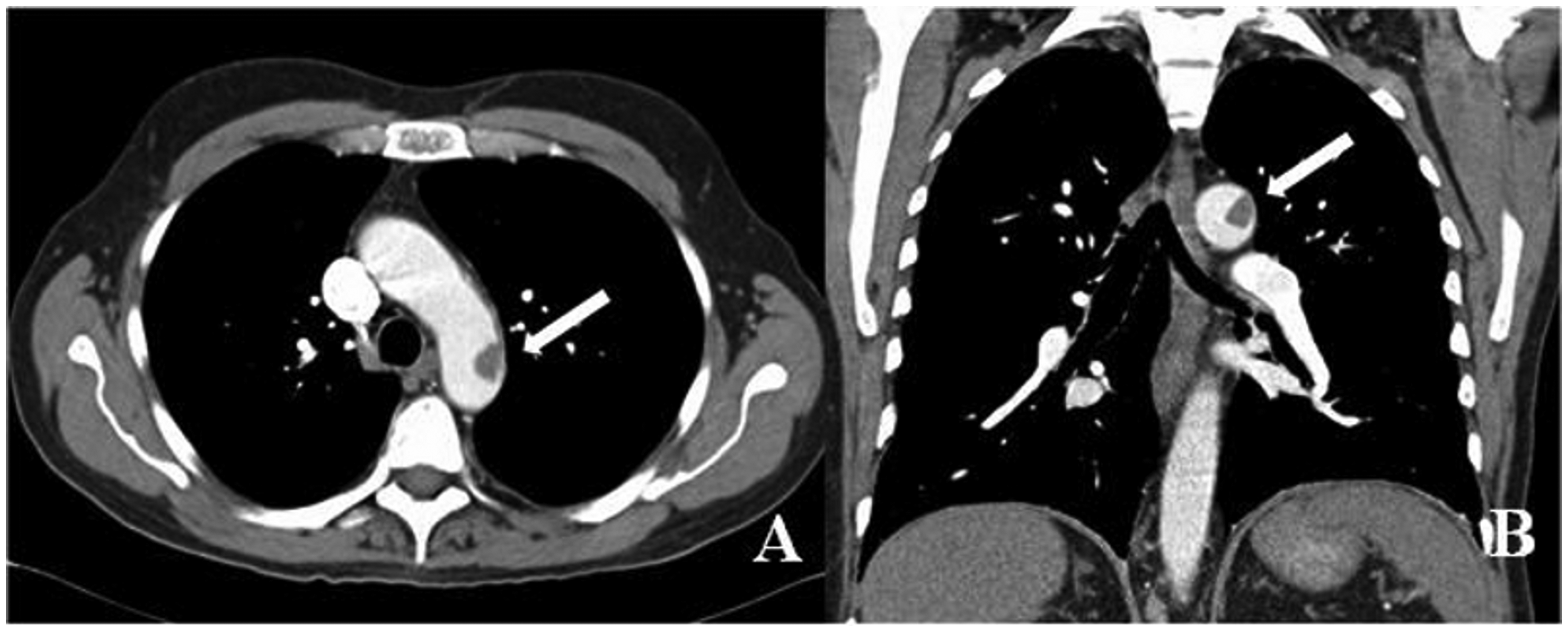
Discussion
Suggested pathogeneses of TAMT include underlying malignant disease, hematologic disorders, exogenous steroid and estrogen use, and primary endothelial disorders. 2 Our patient was at high risk for TAMT, due to both PV and steroid usage. PV is a myeloproliferative disorder associated with a variety of clinical sequelae. Thrombosis of veins or arteries, manifested by overproduction of erythrocytes, granulocytes, and megakaryocytes, is a major cause of morbidity and mortality, accounting for 35–45% of the causes of death. 4 In a large study of patients with PV, age over 65, and a history of previous thrombosis were known to be the most powerful predictors of recurrent thrombosis and cardiovascular events. 5 Another large study identified arterial thrombosis at the time of diagnosis, age over 60, and a WBC >15 × 109/L as independent predictors of inferior survival. 6 Today, low-dose aspirin, phlebotomy, and platelet-lowering agents (hydroxyurea or interferon alpha) are the treatment of choice in patients with PV complicated by thromboembolism. 7 While thrombosis of the cerebral, coronary, and peripheral vessels is common in patients with PV, TAMT is an extremely unusual event. 7 Only one other case has been reported so far in the literature. 8
The treatment choice for TAMT still remains controversial. Several therapeutic options are previously described including anticoagulation, thrombolysis, thromboaspiration, open thromboendarterectomy, prosthetic replacement, and endovascular exclusion.1–3 Endovascular interventions are advantageous due to less associated morbidity and shorter hospital course compared with open procedures. Furthermore, a peripheral thromboembolectomy can be done through the same surgical access. This approach also treats the potential underlying cause of the thrombogenic aortic wall by exclusion. Even though the short-term outcomes of endovascular approaches are promising, recurrence is still a major concern. 3 In addition, SG exclusion possesses a greater risk for recurrent embolization potentially due to the intraluminal manipulation of guide wires. Further studies with long-term follow-up will be necessary to assess its safety and efficacy. In contrast, complete resolution or reduction in the size of the thrombus has also been reported with anticoagulation alone. 2 After performing a retrospective review of similar cases, we believe anticoagulation and thromboembolectomy for limb ischemia, without performing definitive surgical intervention, may be a better treatment strategy in the present case considering the underlying uncontrolled thrombophilia.
Our patient manifested SCI in the form of paraparesis and achieved near-complete neurologic recovery. The SG length and underlying thrombophilia are also suggested to be important predictors for SCI. The SG used in this patient was 15 cm, which is considered to be extent A coverage. 9 Although the patient had a relatively short segment of thoracic aortic coverage, his uncontrolled thrombophilia may have led to a compromised collateral network of blood supply to the spinal cord, contributing to SCI. Therefore, we believe that all measures proven to prevent SCI, including perioperative somatosensory evoked potential monitoring, earlier arterial pressure augmentation, and preoperative cerebrospinal fluid drainage insertion, 10 should be strictly utilized in such patients.
This is in fact the first reported case of aortic SG placement in the presence of PV, despite being a well-known and relatively common hematologic neoplasm. The true cause of these unprecedented catastrophic thromboembolic events after TEVAR remains unclear. Development of TAMT perhaps indicates the presence of a hypercoagulable state in patients with PV. HIT was initially suspected, however, HIT panels were consistently negative. The high baseline and the abrupt decline in platelet count (Figure 3) obviously confused the clinical picture. Thus, in particular circumstances, such as the present case, shorter usage of heparin and earlier empirical use of a direct thrombin inhibitor should be considered. One theory hypothesizes that these catastrophic thromboembolisms resulted from a significant inflammatory response induced by SG. While this is a controversial assumption, the SG might have induced a coagulation cascade and exacerbated the thrombophilic state, resulting in catastrophic thromboembolic events despite successful surgical exclusion of the TAMT and continued anticoagulation. It has been shown that endovascular aortic repair might induce an inflammatory response, which may be explained by a release of IL-6 from the intramural thrombus, causing WBC stimulation and production of TNF-α. 11 Furthermore, inflammation is thought to play a significant role in the thrombotic risk of myeloproliferative neoplasms mainly through blood cell activation. 12
Conclusion
We report a 62-year-old male with PV and TAMT. Anticoagulation and surgical thrombectomy to solve peripheral ischemic complications seem to be an appropriate strategy; however, definitive surgical treatment of TAMT should be reserved for patients with contraindications to conservative treatment or end-organ ischemia. TAMT in the presence of underlying PV is exceedingly rare and may pose recurrent thromboembolic risk after endoluminal procedures, possibly due to stimulation of coagulation cascade. We would recommend proceeding with extreme caution when performing endovascular exclusion of the thrombus as PV may be a prohibitive risk.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.