
Abstract
Objectives
This study was conducted to investigate the progression of lower extremity ischemia following kidney transplantation to iliac artery in patients with peripheral arterial disease.
Methods
A retrospective chart review of all renal transplant patients completed at a university teaching medical center from January 2006 to December of 2011 was performed. A total of 219 patients underwent successful kidney transplantation to the common, external, or internal iliac artery. Pre- and post-transplantation ischemic changes in the ipsilateral lower extremity were reviewed and analyzed.
Results
Thirty-eight of the 219 patients had ipsilateral peripheral arterial disease and seven of them were symptomatic. Six of the seven symptomatic patients remained stable and one patient’s rest pain improved, postoperatively. Eight patients developed new symptoms of ischemia 12 months later, including four with claudication, two with ischemic ulcers, and two with gangrene toes. The ulcers were healed following superficial femoral artery stenting and wound care. Toe amputation was performed in two patients with gangrene. No major amputation was required up to 48 months of follow-up.
Conclusions
Transplanted kidney to iliac artery does not significantly deteriorate ischemia in adults with ipsilateral lower extremity peripheral arterial disease. Late developed ischemic complications may be due to the progression of underlying arterial disease.
Introduction
Peripheral arterial disease (PAD) among patients with end-stage renal disease is common and its prevalence may be as high as 30% reportedly.1,2 One of the clinical concerns is the possibility of ischemia deterioration of the lower extremity with PAD due to blood diverting by a kidney transplanted to the iliac artery. 3 Acute limb ischemia due to steal phenomenon by graft kidney has been reported in pediatric patients. 4 The clinical significance of this “blood steal” phenomenon in adult patients with PAD has not been well documented, although it has been one of the main concerns during pre-transplantation evaluation.3,5,6 Current guidelines of the evaluation of renal transplant candidates with PDA recommend surgical intervention if the PAD is symptomatic, but do not comment on patients with symptomatic PAD who are not candidates for revascularization because of diffuse distal arterial disease. 5 Therefore, the question arises whether renal transplantation will deteriorate limb ischemia, especially in symptomatic patients, and whether those patients should be excluded from the transplant waiting list.
Our study investigates and discusses the progression of lower extremity ischemia following renal transplantation in a group of patients with preexisting PAD.
Patients and methods
A retrospective chart review of all renal transplant patients completed at a university teaching medical center from January 2006 to December 2011 was performed. Patients were excluded if the renal artery was anastomosed to the aorta. A total of 219 patients underwent successful kidney transplantation to the common, external, or internal iliac artery. Data including pre- and post-transplantation limb ischemic changes, conventional angiography, CT angiography (CTA), and MR angiography (MRA) of the ipsilateral lower extremity were collected and analyzed.
Results
Changes of ipsilateral lower extremity ischemia following kidney transplantation.
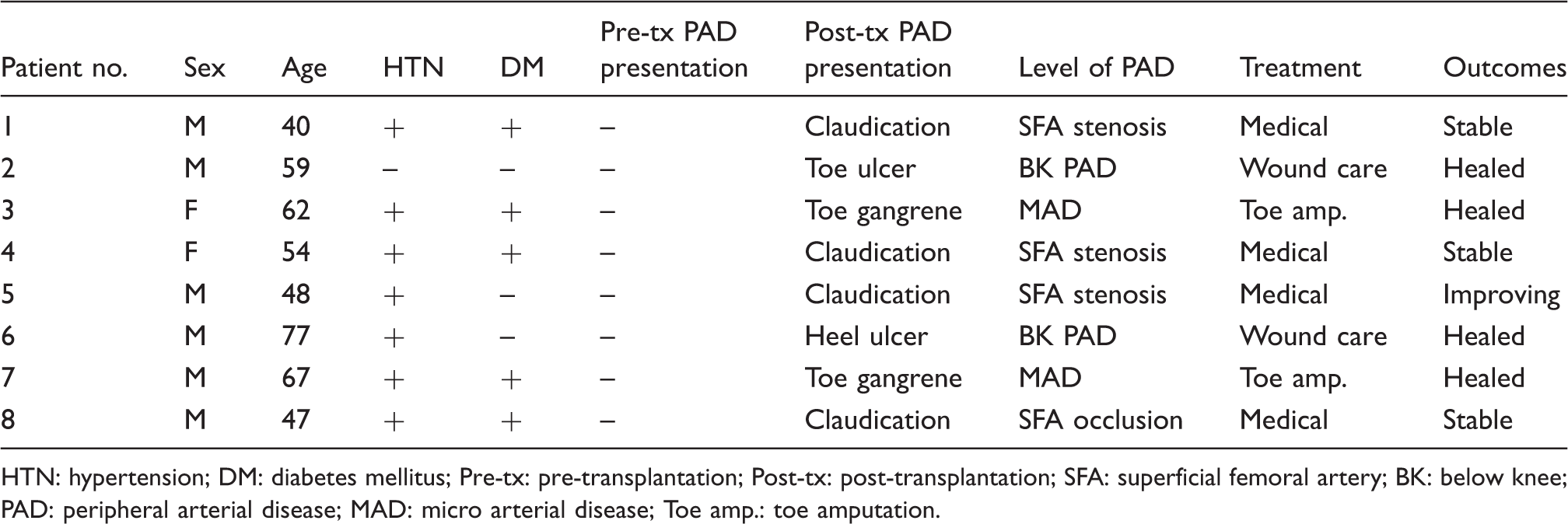
HTN: hypertension; DM: diabetes mellitus; Pre-tx: pre-transplantation; Post-tx: post-transplantation; SFA: superficial femoral artery; BK: below knee; PAD: peripheral arterial disease; MAD: micro arterial disease; Toe amp.: toe amputation.
Discussion
PAD is very common in the patients with end-stage renal disease (ESRD), and the incidence of PAD may be as high as 30%, especially in those with diabetes mellitus.1,2,5,7,8 Previous reports demonstrated that blood steal from the iliac artery by a transplanted kidney may result in acute limb threatening ischemia in pediatric patients. 4 Transplant and vascular surgeons are concerned whether the blood flow diverting phenomenon occurs in adults following kidney transplantation, and subsequently causes deterioration of the limb ischemia in the patients with preexisting PAD.3,5 As vascular surgeons, we are often consulted to perform peripheral vascular evaluation in renal transplant candidates for two main purposes: (1) To rule out significant aorto-iliac occlusive disease (AIOD) and reduce the risk of ischemia of a transplanted graft; (2) To assess the severity of lower extremity PAD and the possibility of ischemia deterioration due to blood steal by transplanted kidney.
It has been documented and well accepted that symptomatic AIOD should be treated before or during transplantation if the iliac artery is planned to serve as the inflow,5,9 or the donor kidney should be anastomosed to a different location above the stenosis if iliac disease is not correctable. Current American clinical practice guidelines recommend endovascular or surgical intervention for symptomatic lower extremity PAD before transplantation. 5 However, the guidelines did not address what we should do for the ESRD patients who have symptomatic PAD, but are not candidates for revascularization because of diffuse distal PAD. This leaves an unanswered question: are those patients precluded from kidney transplantation?
Natural history of PAD following kidney transplantation remains unclear. Snyder et al. reviewed a Medicare database including 132,625 patients with ESRD. This important study compared the incidences of PAD in 43,427 kidney transplant recipients versus that in 53,309 adult ESRD patients on the renal transplant waiting list. The data demonstrated that the incidence of PAD is higher on the waiting list than after transplantation. 7 However, the patients with diagnosed PAD before transplantation were excluded from this study. In our 219 patients, seven had symptomatic PAD before kidney transplantation. Ischemic symptoms and/or signs remained the same in six patients and improved in one patient. Acute limb ischemia has been reported in adult patients following kidney transplantation, but all resulted from acute arterial thrombosis. 10 Our eight patients with known history of lower extremity PAD became symptomatic after transplantation. Since the symptoms/signs occurred at least six months later, ischemia is likely due to the progression of underlying PAD, but not acute steal phenomenon. None of the eight patients required major amputation, which is similar to the previous findings that frequency of lower limb amputation in diabetic renal transplant patients is not higher than that in non-transplanted diabetic patients. 11 This suggested that blood steal by a transplanted kidney in adult patients is not as significant as we used to worry, although it may cause limb threatening ischemia in pediatric patients. 4
We agree that symptomatic PAD patients on the kidney transplant waiting list should undergo endovascular or surgical revascularization prior to transplantation. 5 It may decrease the risks to transplanted kidneys if the endovascular or open revascularization can be done before transplantation. Our data show that kidney transplantation can be performed safely in ESRD patients with symptomatic PAD, without deteriorating lower extremity ischemia. This finding supports the Scandling’s 9 suggestion that a history of PAD including limb amputation should not be precluded from the kidney transplantation.
One major limitation of our study is the lack of PAD incidence in the group of ESRD patients who are not treated with kidney transplantation. We cannot conclude that kidney transplantation reduces the risk of PAD in ESRD patients, which was documented by Snyder et al. 7 But our longitudinal comparisons before and after renal transplantation demonstrate that transplanted kidney to iliac artery does not cause “steal syndrome” nor deterioration of ipsilateral limb ischemia. Comparison of PAD incidences in patients on a transplant waiting list and in renal transplant recipients will be conducted.
Noninvasive vascular lab examination was only performed in less than 20% of the patients in this group. It is another limitation of this retrospective chart review study. Pre- and post-transplantation vascular lab data are very useful for the follow-up of lower extremity ischemia.
In summary, the current American clinical practice guidelines recommend endovascular or surgical intervention for symptomatic lower extremity PAD before transplantation. 5 Our study demonstrates that renal transplantation does not cause deterioration of ipsilateral lower extremity ischemia, even in the patients with symptomatic chronic limb ischemia but not candidates for revascularization.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.