
Abstract
Purpose
To present a case of inadvertent collapse of the contralateral limb gate caused by misorientation during the deployment of the Ovation Abdominal Stent Graft System in a narrow aortic lumen and the bailout conversion to aortouniiliac modification, using a covered stent to exclude the orifice of the internal iliac artery (IIA).
Technique description
Despite the repeated efforts from the femoral and brachial site, the collapsed/occluded contralateral limb gate could not be catheterized. In order to exclude successfully the orifice of the IIA, an oversized stentgraft was placed immediately at the common-to-external iliac artery (CIA-EIA) transition followed by peripheral ligation of the latter. The procedure was completed with crossover femorofemoral bypass.
Conclusion
Occlusion the IIA orifice with an oversized stentgraft in the CIA-EIA transition can be considered as a safe, simple, fast, and efficient bailout maneuver, followed by EIA ligation and crossover bypass.
Keywords
Introduction
The Ovation Abdominal Stent Graft System (TriVascular, Santa Rosa, CA, USA) System is a trimodular endoprosthesis recently introduced for the endovascular aneurysm repair (EVAR) of abdominal aortic aneurysms (AAA). Its main characteristic is the dissociation of the suprarenal fixation from the infrarenal sealing mechanism, which is accomplished by a network of compliant, inflatable rings that are filled with a low-viscosity radiopaque polymer. 1
The uncoupling of the fabric material from the presence of a Nitinol skeleton enables significantly lower delivery catheter profiles of 14 F (outer diameter), but render Ovation’s iliac limb gates prone to collapse in cases of a narrow aortic lumen, making the catheterization challenging or impossible.2–4 The present report addresses this technical challenge and describes the successful conversion into an aortouniliac modification, facilitated by exclusion of the unilateral internal iliac artery (IIA) via a covered stent, peripheral ligation of the external iliac artery (EIA) and completion with crossover bypass.
Technique description
An 80-year-old man was admitted with an infrarenal AAA of 5.5 cm. The patient’s age, his status of heart failure and chronic obstructive pulmonary disease excluded the option of open repair. The preoperative evaluation with contrast-enhanced computed tomography (CT) imaging revealed an infrarenal neck with excessive amount (>50%) and irregular, eccentric shape of neck thrombus (Figure 1(a)), precluding the safe use of a nitinol-based self-expandable bifurcated or aortouniiliac graft.
5
Therefore, the Ovation stentgraft with the sealing mechanism of the polymer-filled sealing rings capable of adjusting to the thrombus irregularity was deemed as the only eligible device for this AAA.
(a) Transverse plane of the infrarenal aortic neck 13 mm below the inferior left renal artery (IR), where the Ovation’s first inflatable ring is anticipated to seal. The irregular configuration of the neck thrombus causes an asymmetrical lumen (23 × 29 mm) where the cylindrical shape of a self-expandable Nitinol stentgraft cannot be sufficiently adjusted. Moreover, the tight aortic lumen diameter 80 mm below the left renal artery poses a certain difficulty in the optimal deployment of both iliac limb gates of the Ovation, if this occurs in the narrowest diameter (18.3 mm) due to false orientation of the device (b).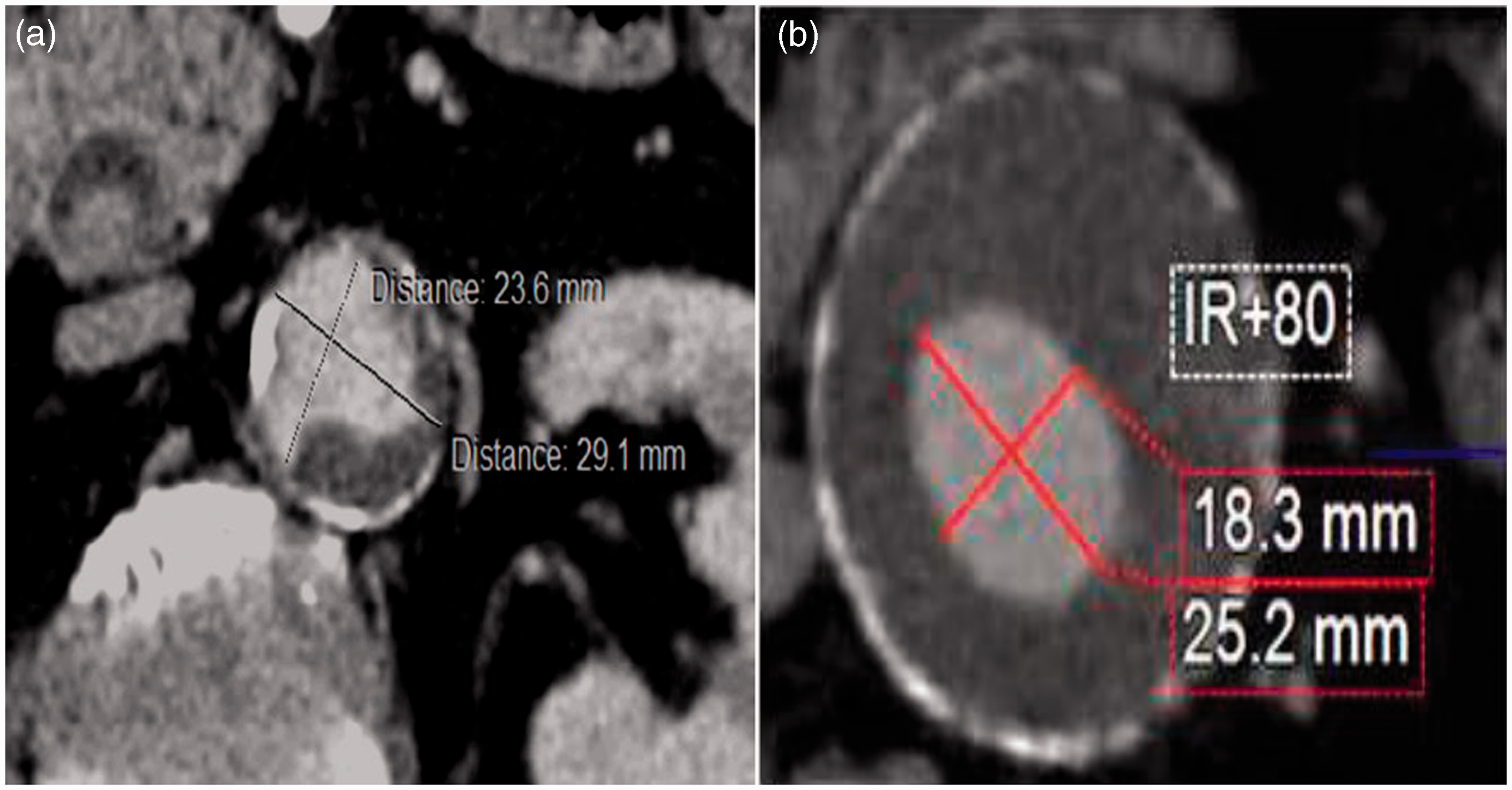
The distal ends of the Ovation’s iliac gates expand at a level of 80 mm below the inferior renal artery. Hence, the narrow aortic lumen diameter at 80 mm below the inferior renal artery posed a certain difficulty for the sufficient completion of both iliac limb gates’ deployment, in case the latter inadvertently occurred in the narrowest diameter (18.3 mm) due to false orientation of the device (Figure 1(b)).
After navigation, advancement and positioning of a 34-mm Ovation endograft to the level just below the inferior renal artery, the suprarenal stent was deployed. The polymer managed to fill the entire tube network to the last caudal ring of the contralataral limb. An excellent neck sealing at the infrarenal level was performed, with complete adjustment of the inflatable rings to the irregular geometry of the thrombus (Figure 2(a)). However, visualization of the inflatable rings of the endograft’s contralateral limb with the radiopaque polymer revealed a collapse of its iliac gate against the intraluminal thrombus, rendering the retrograde catheterization from either femoral site unsuccessful, despite repeated attempts using multiple combinations of diagnostic catheters and guidewires. Accordingly, the left brachial route was recruited in order to attempt anterograde catheterization of the compromised iliac limb via means of a 5Fr 120 cm-long selective catheter and a 0.035′ hydrophilic 260 cm Terumo soft guidewire, supported by a long 6Fr × 90 cm Arrow sheath.
3
Unfortunately, this manipulation proved also unsuccessful, whereas anterograde angiography from the long, brachial sheath whose tip reached the upper end of the Ovation device revealed complete absence of visualization of the collapsed contralateral limb immediately from the level of its conjugation with the main body, referring to complete occlusion of this limb.
(a) Postoperative cross section of the aneurysm neck at the level of the sealing ring in a computed tomography prior to administration of intravenous contrast. The inflatable ring filled with radiopaque polymer ensures perfect sealing, at the expense of a flow lumen reduction. (b) The conversion to aortomonoiliac mode. The intravenous contrast is visualized within the lumen of the limb extension. No signs of endoleak are detected.
Since the sole operative choice dictated the conversion to aortomonoiliac configuration, we performed so from the left side (Figure 2(b)) accompanied by a femorofemoral crossover bypass from left-to-right, as a bailout procedure. Normally, this is performed either by occlusion of the contralateral common iliac artery (CIA) with plug or coiling of the IIA and interruption of retrograde flow from the EIA with ligation of the latter. Moreover, a reverse-U stentgraft from the EIA-to-the IIA can be applied to accomplish simultaneously the abovementioned tasks.
Since an occluder plug was unavailable at the time of operation, we chose to place a stentgraft extending from the CIA to the EIA, thus covering the orifice of the IIA. The stentgraft (Fluency plus, Angiomed GmbH & Co, Karlruhe, Germany) 13.5 mm × 6 cm was oversized with respect to the maximum diameter (11 mm) of the caudal segment of the right CIA, i.e., adjacent to the orifice of the IIA. The IIA exclusion was confirmed with angiographic absence of retrograde flow. The operation was completed with placement of two iliac extensions (120 mm × 12 cm and 80 mm × 12 mm, respectively) to the caudal end of the left CIA, causing abrupt absence of pulpable right femoral pulses. Accordingly, the right EIA was ligated at the level of the inguinal ligament and the crossover bypass was conducted.
The postoperative CT angiography showed occlusion of the right CIA with complete absence of endoleak Type II (Figure 3) from the IIA orifice and the EIA and preservation of the left IIA (arrow).
Three-dimensional CT reconstruction, anterior view. The sealing rings of the Ovation device are seen on top. The crossover femorofemoral bypass and the stentgraft in the right iliac axis can be seen, as described in the manuscript. Complete absence of any endoleak is ensured, while the left hypogastric artery (arrow) remains patent, contributing to the pelvic perfusion.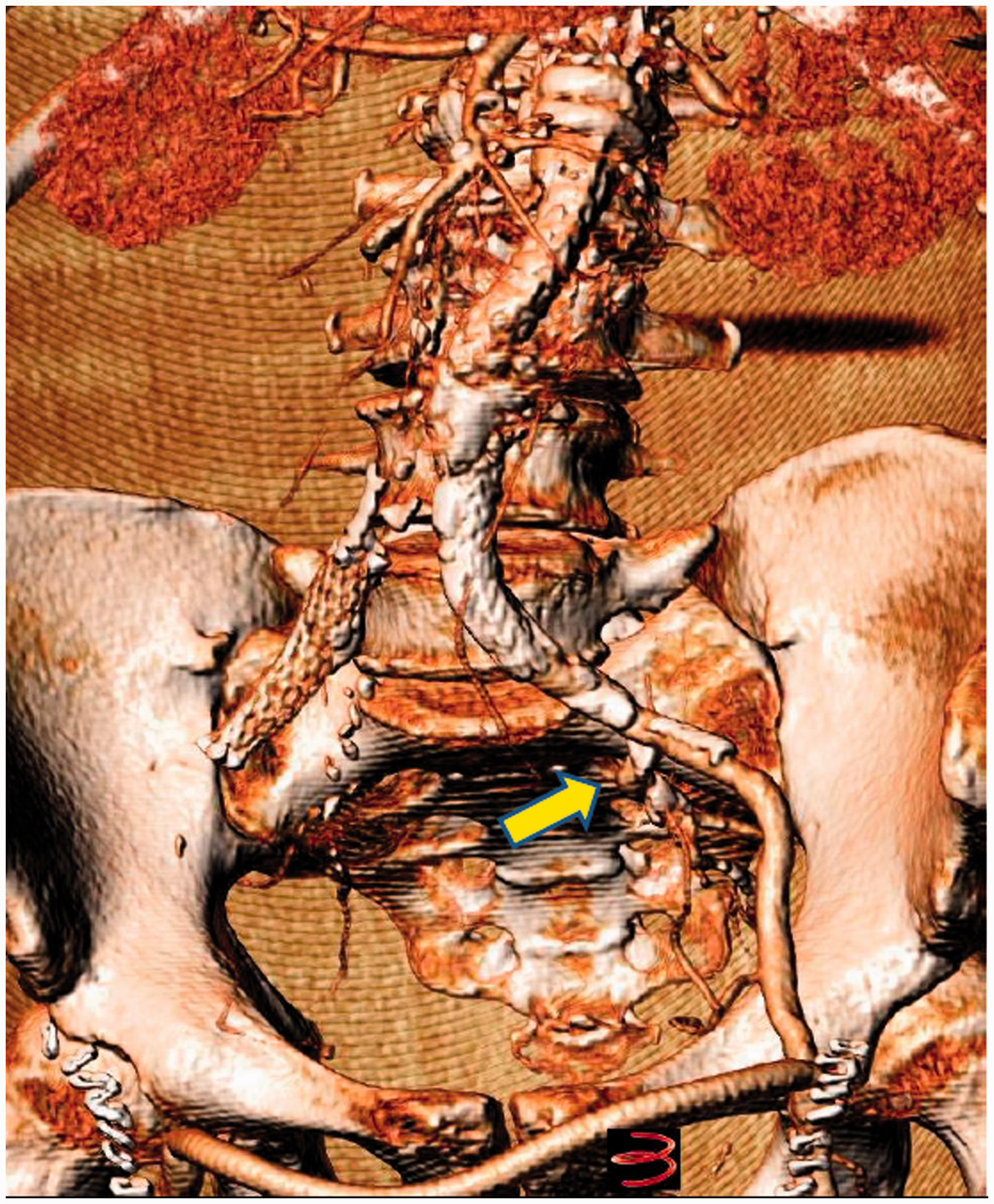
Discussion
Our case represents a most challenging scenario where the irregular shape and the excessive amount of neck thrombus precluded the safe use of an aortic endograft based on a cylindrical self-expandable Nitinol mechanism, either in the bifurcated or the aortouniiliac mode. 5 On the contrary, the system of inflatable rings adjusted perfectly to overcome this anatomical burden. The reduction of the flow lumen caused by the inflation of the sealing ring has been recently described, identifying no significant hemodynamic consequence with respect to the limbs perfusion. 6
The polymer infusion in the contralateral rings takes place lastly, only after the filling of the previous segments has been completed. As can be seen in Figure 1(b), meticulous orientation of the endograft was warranted for adjustment at the large lumen diameter (25 mm) instead of the narrow (18 mm). Unfortunately, a malrotation during this adjustment must have occurred, leading to adaptation of the narrow dimension. Therefore, by the time the polymer reached the contralateral limb, the ipsilateral one was already inflated to its maximum diameter (12 mm), occupying most of the narrow luminal space and leaving a very limited space (if any) for filling and expansion of the contralateral limb and predisposing to its compression and occlusion.
When such a scenario is highly anticipated or suspected based on the preoperative measurements and planning, our experience suggests that an anterograde catheterization via the brachial access is not to be delayed in order to prevent the contralateral “collapsed fixation.” Otherwise, the aortouniiliac conversion is deemed as the only bailout option.
The aortouniliac conversion necessitates the unilateral CIA exclusion by coiling or plugging, provided that the salvage of the IIA for maintenance of retrograde perfusion is of essence. 5 Alternatively, the selective occlusion of the IIA coupled with exclusion of the ipsilateral EIA can be performed.7–10
The lack of coils and occluder devices needed to encounter the need of aortouniiliac conversion led us to using a stentgraft in the CIA-EIA transition in order to seal effectively the orifice of the IIA. This maneuver was performed easily and fast, obviating the need of oblique projections and multiple angiographies in order to detect the IIA orifice or to catheterize it, especially in cases of severe iliac angulation and tortuosity. Based on these, it is our strong impression that a single occlusion of the IIA orifice with a CIA-EIA stentgraft followed by crossover bypass encompasses an efficient, safe, and fast bailout maneuver for aortouniiliac conversion in case of limb gate collapse and occlusion.
It should be stressed out that our example should by no means be misinterpreted as a technical failure of the specific aortic endograft. On the contrary, our case exemplifies clearly the unique characteristics of the Ovation abdominal stentgraft that render it irreplaceable to extremely challenging AAA cases, which would be otherwise considered ineligible for EVAR.
Conclusion
Malrotation or misorientation of the Ovation device in a narrow lumen can lead to collapse and occlusion of the iliac gate, necessitating an aortouniiliac conversion. In such cases, occluding the IIA orifice with an oversized stentgraft in the CIA-EIA transition can be considered as a safe, simple, fast, and efficient bailout maneuver, followed by EIA ligation and crossover bypass.
Footnotes
Authors’ note
Patient informed consent to this manuscript has been received. All measures have been taken to exclude identifying details and ensure the patient’s anonymity.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgments
None declared.