
Abstract
Objective
To evaluate the feasibility and anatomical success of endovenous laser ablation (EVLA) of incompetent perforating veins (IPV).
Methods
All 135 consecutive patients with IPV treated with ELVA (intention-to-treat) from January 2008 to December 2013 were included. Up to the end of 2011, an 810-nm laserset (14 W) was used, and afterwards, a 1470-nm laserset (6 W) was introduced. Duplex ultrasound was performed at 6 weeks’ follow-up to assess anatomical success.
Results
Overall anatomical success at 6 weeks’ follow-up was 56%. Anatomical success was 63% after treatment with 810 nm and 45% with 1470 nm (p = 0.035). This difference in the success rate seems associated with the significantly higher amount of energy delivered in the 810 nm cohort (560 J) versus 1470 nm (186 J). Regardless of the type of laser, anatomical success was significantly higher after treatment with more than 400 J (66%) compared with 0–200 J (40%, p = 0.009) and 200–400 J (43%, p = 0.029). Complications were limited to two cases of transient paresthesia.
Conclusions
EVLA of IPVs is safe and feasible. The amount of energy is highly important in achieving anatomical success.
Keywords
Introduction
Varicose veins are among the top 10 most common problems for which patients consult their general practitioners. Epidemiologic studies show that some degree of varicose veins will develop in approximately 40% of women and in 20% of men.1,2 The incidence increases with age and several risk factors, including prolonged standing, pregnancy, and female gender. Clinical symptoms vary from cosmetic issues to therapy-resistant venous ulcers. Chronic venous leg ulceration will occur in approximately 1% of the general population. Venous insufficiency has a substantial effect, mostly associated with insufficiency of the great saphenous veins (GSVs), on patients’ health-related quality of life. 3
Insufficient perforating veins (IPVs) are frequently observed in patients with chronic venous insufficiency. Although the effect of IPVs on hemodynamics remains controversial, there is some evidence for the potential role for IPVs in the pathogenesis of advanced venous disease.4,5 An increasing number and diameter of calf IPVs are associated with deteriorating CEAP (Clinical, Etiology, Anatomy, and Pathophysiology) grade. 6 Treatment of IPVs in severe chronic venous insufficiency can result in improved rates of ulcer healing and lower recurrence. 7
Over the years, several treatment options for IPVs have been advocated. Surgical ligation or disconnection is considered the gold standard. However, the revolution of minimally invasive therapies for saphenous insufficiency also led to innovation in the treatment of IPVs. Subfascial endoscopic perforator surgery, ultrasound-guided foam sclerotherapy, and endothermal ablation, such as radiofrequency ablation and endovenous laser ablation (EVLA), were introduced. Although EVLA is widely used and well proven in insufficient GSVs, laser ablation of IPVs was only described in small series.8–13 This prospective single-center study was designed to evaluate the feasibility, safety, and anatomical success of EVLA as a minimally invasive therapy for IPVs.
Methods
Study design
This prospective study included all consecutive patients treated with EVLA for IPV during a 5-year period from January 2009 to December 2013. All patients underwent standardized clinical and physical examination and duplex ultrasonography (DUS) of the affected lower limb. Complete venous mapping of the saphenous veins, deep system of the calf and thigh, and perforating veins was performed. Insufficiency was defined as a retrograde flow >500 milliseconds after calf compression while standing. 14 The C of the CEAP classification was used to score the clinical severity of each affected limb. 15
In patients with combined long-segment saphenous insufficiency and concurrent IPV, the truncal insufficiency was treated first. In case of persistent complaints after adequate ablation of the superficial trunk or isolated perforator insufficiency, ELVA of the IPVs was offered.
All patients gave informed consent for prospective follow-up.
Intervention
All interventions were performed by one of three vascular surgeons with the assistance of a vascular laboratory technician. Before treatment, the IPVs were identified by DUS with the patient upright and marked on the skin. An elastic tourniquet was applied to maintain venous congestion, and the patient was placed supine. The importance of adequate ultrasound guidance during the entire procedure must be underlined. An experienced ultrasonographer is critical for the initial puncture of the IPV, advancement, and the correct positioning of the laser tip within the IPV lumen at a level below the fascia, without protruding into the deep venous system.
In the period 2009 to December 2011, IPVs were treated with an 810-nm laser generator and a bare tip laserset (Angiodynamics, Queensbury, NY, USA). From December 2011 onwards, a 1470-nm laser generator with 400-µm perforator laserset (Angiodynamics, Queensbury, NY, USA) was used. The laserkit was changed following company recommendation. After adequate intraluminal access to the IPV with the puncture set, there were two options: direct insertion of the laser tip through the needle or placement of a sheath over a guidewire before insertion of the laser tip. Tumescent anesthesia was injected around the target vein before ablation. No sedatives were administered. According to instructions for use, the 810-nm laser delivered 14 Watts. The 1470-nm laser tip delivered 6 Watts. The procedure was performed under ultrasound guidance to confirm position and to guide laser fiber pull back. If necessary, ELVA of multiple IPVs was performed.
Patients were advised to wear 23 mm Hg compression stockings continuously for the first 48 h and during the daytime for the next five days. Patients were allowed to perform their daily activities immediately. No anticoagulants were prescribed. Over-the-counter analgesics were advised if necessary.
Outcomes and follow-up protocol
The primary outcome measure was anatomical success, defined as occlusion of the treated perforating vein on follow-up DUS at six weeks. Initial technical success was defined as the ability to cannulate the IPV, place the laser tip as planned, and ablate without technical problems. Treatment failure was defined as a nonoccluded or recanalized IPV with persistent flow on DUS. The other important outcome was the occurrence of major complications, including deep venous thrombosis (DVT), skin burns or nerve injury.
All patients were invited for a follow-up assessment by a vascular surgeon at six weeks. This assessment included an interview, a physical examination, and DUS by a vascular laboratory technician. Any complications immediately after the procedure and during the follow-up were noted. All data were gathered prospectively and stored in a computerized database.
Statistical analysis
Variables are presented as mean with standard deviation (SD) or range for parametric continuous outcomes, as a median with interquartile range (IQR) for nonparametric continuous outcomes, and as frequencies and percentages for categoric variables. Kaplan–Meier survival analysis was used to assess the anatomical success rate. Statistical analyses were performed using SPSS 19.0 software (SPSS Inc., Chicago, IL, USA). A value of p < 0.05 was considered significant.
Results
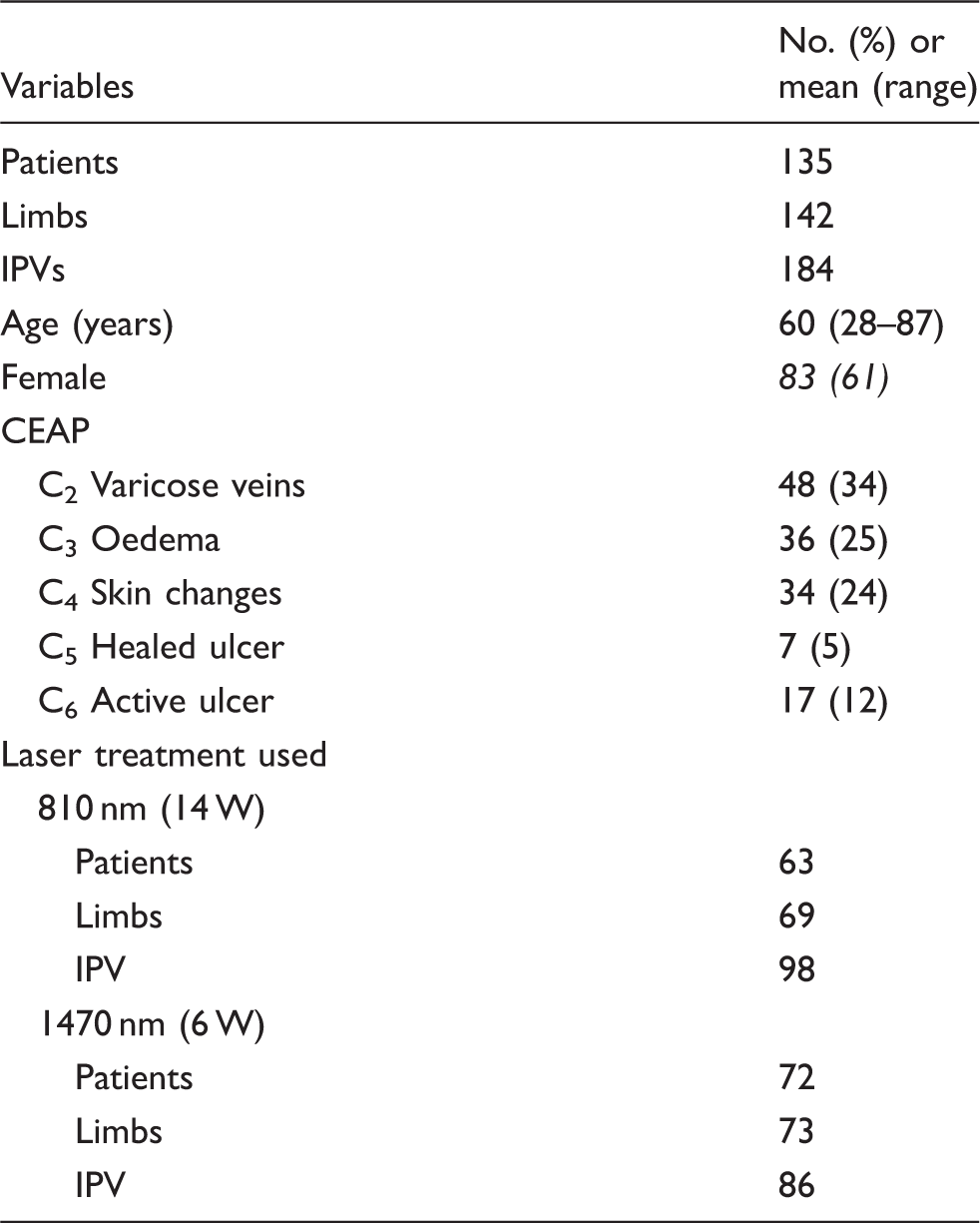
Patient demographics and treatment characteristics.
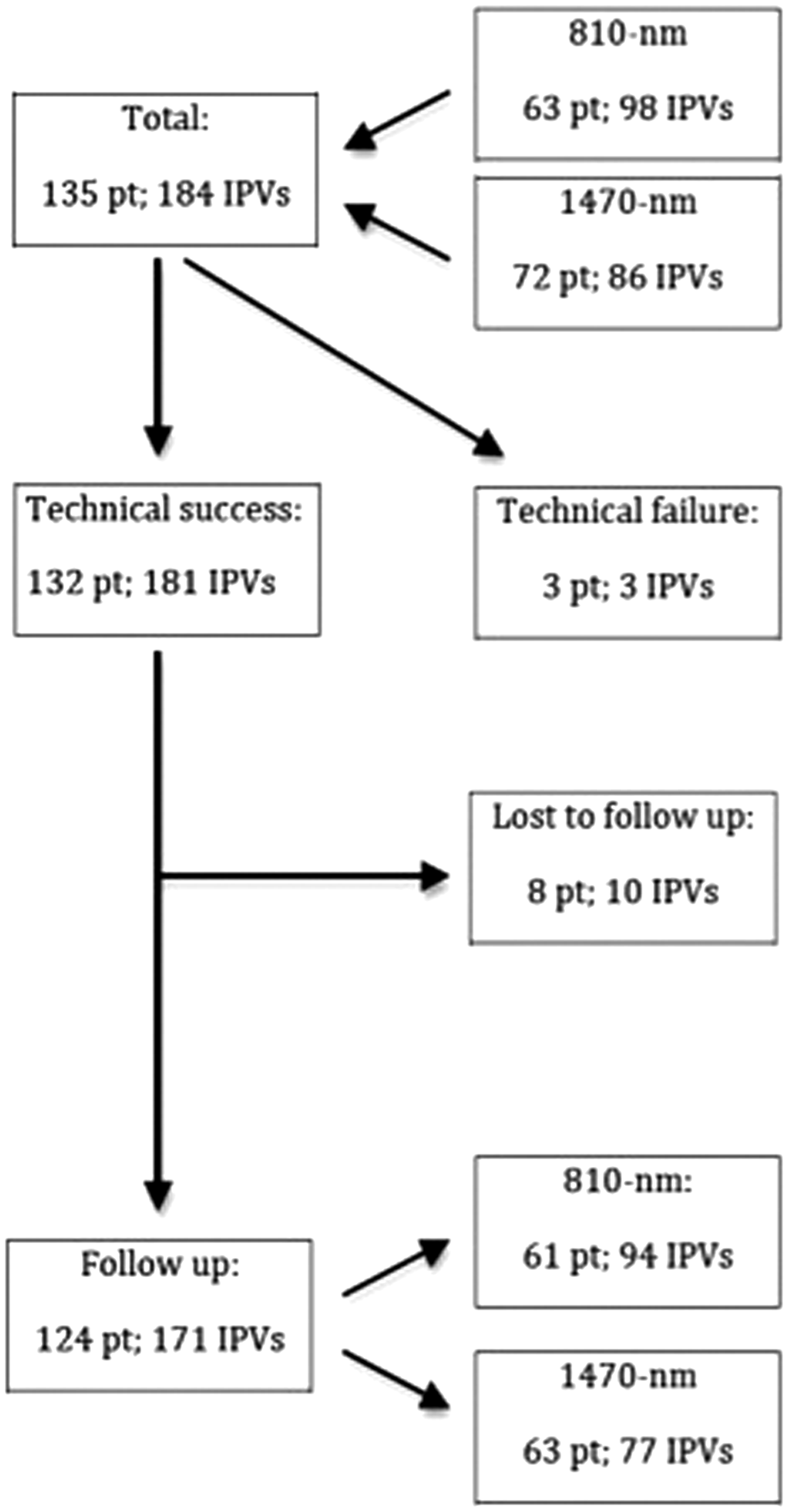
Flow diagram.
Initial technical success
A total of 184 IPVs were treated during 135 procedures. In three cases, we failed to cannulate the IPV, and the treatment was aborted. The overall initial technical success was 98%. There were no significant differences in initial technical success between the different lasers.
Anatomical success
DUS and clinical consultation was obtained in 131 limbs of 124 patients during a median follow-up of 46 days (IQR, 42–58 days). Three patients were excluded from follow-up due to initial technical failure. A total of eight patients were lost to follow-up: five indicated that they were freed of complaints and refused follow-up, two did not respond to repeated invitations for the follow-up assessment, and one died of an unrelated cause.
In the entire group of 124 patients, 131 limbs, and 171 IPVs with completed follow-up, DUS showed an overall anatomical success rate of 56%. The anatomical success of treatment with the 810-nm laser (61 patients, 67 limbs, 94 IPVs; median energy delivery, 560 J) was 63%. After treatment with the 1470-nm laser (63 patients, 64 limbs, 77 IPVs; median energy delivery, 186 J), the anatomical success was 45%. The difference in anatomical success between these two groups was significant (p = 0.035).
Regardless of the type of laser used, cohorts were compiled according to the amount of energy delivered. The cohorts were formed with 200-J intervals: 0–200 J, 200–400 J, and more than 400 J. The anatomical success in these groups was respectively 40%, 43%, and 66%. The anatomical success rate after treatment with more than 400 J seems to plateau. Univariate logistic regression analysis showed a significantly higher anatomical success after treatment with more than 400 J compared with, respectively, 0–200 J (p = 0.009) and 200–400 J (p = 0.029). The difference in anatomical success among the three vascular surgeons was not significant. There was no significant difference in anatomical success between the different CEAP groups.
After failure of the primary intervention, 15 patients, 15 limbs and 17 IPVs were treated a second time with EVLA of the persistent IPV. In this group, 10 patients with 11 IPVs underwent follow-up DUS. The anatomical success after the second treatment was 55%, which was similar to primary treatment. No significant differences between the different lasers were seen in this group.
The three patients (three limbs, three IPVs) in whom the initial procedure was unsuccessful underwent retreatment with EVLA. In only one patient did retreatment lead to initial technical success and anatomical success at follow-up DUS. In the remaining two patients, cannulation of the IPV was not technically feasible due to difficult angle.
Complications
No DVT or skin burns were seen. Transient paresthesia of the sural or saphenous nerve was observed in two patients, one in each laser wavelength group. Minor complications, including pain and ecchymosis, were common but did not require additional treatment.
Discussion
The most remarkable finding of this study is the significantly higher anatomical success after treatment with increased energy deliverance. This explains the difference we found in the anatomical success rate of the two different lasers used in this study. Because there is no evidence that the laser wavelength has any effect on the outcome, 16 the significant difference in anatomical success seems to be caused by the higher energy deliverance in the cohort treated with the 810-nm laser. Previous studies have shown that linear endovenous energy density values up to 400 J/cm in IPV ablation seem associated with improved results.8,13 Further increasing linear endovenous energy density in the ablation of IPV with their characteristic high pressure gradient and short ablation tract can be advocated. These findings led to changes in treatment strategy in our clinic using increased energy.
Overview on reported series of endovenous laser ablation in insufficient perforating veins.
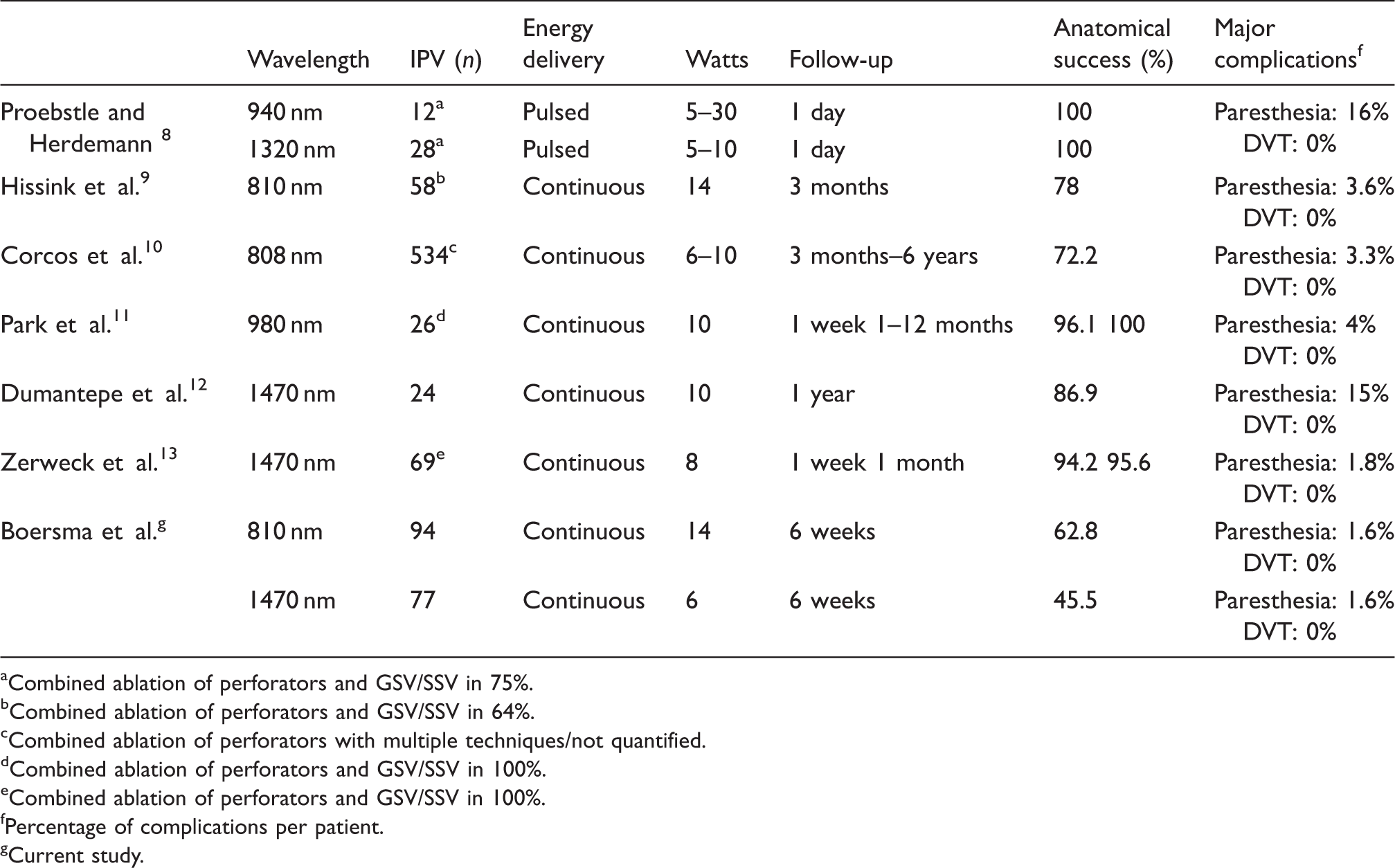
Combined ablation of perforators and GSV/SSV in 75%.
Combined ablation of perforators and GSV/SSV in 64%.
Combined ablation of perforators with multiple techniques/not quantified.
Combined ablation of perforators and GSV/SSV in 100%.
Combined ablation of perforators and GSV/SSV in 100%.
Percentage of complications per patient.
Current study.
Owing to their specific anatomy, a percutaneous approach of perforating veins can be challenging, and especially, cannulation of small diameter veins is associated with a significant learning curve.9,12 Although several studies mentioned technical feasibility, only Park et al. 11 quantify technical success in 76.5%. All procedures in our study were performed by 1 of 3 experienced vascular surgeons, which might have contributed to the technical success in 98% of IPVs.
EVLA has been repeatedly shown to be a safe procedure. Especially in GSV ablation, the data on safety are abundant. In both insufficient perforating veins and SSVs, the treating physician should be well aware of anatomical proximity of nerves in the lower leg. Despite careful administration of tumescent anesthesia, transient paresthesia was seen in two patients. In our series, no cases of skinburn/-necrosis occurred, which is especially of great importance in treating C5 and C6 patients. DVT remains a feared complication after venous ablation or surgery. Neither in previous publications nor in our series did DVTs occur.8–13 Minor complications, such as local bruising, pain, induration, and superficial phlebitis, are common.
The indication for treatment of isolated perforator insufficiency remains up to discussion, especially in C2 and C3 varicosities. 14 In our opinion, the indications to treat IPVs might be stretched due to minimizing surgical trauma, possibility of repetitive treatment and improvement of anatomical success. The clinical success and potential quality-of-life improvement after IPV ablation needs further investigation.
Important limitations of series on ELVA of IPVs are the small cohorts and the simultaneous treatment of saphenous veins. For example, Zerweck et al. 13 describe in their series that concomitant ablation of the GSV or SSV is performed in all patients with IPVs treated by EVLA. The major limitation to our study is the length of follow-up of only six weeks.
Conclusion
EVLA of IPVs is a safe and feasible technique that can be considered a valuable alternative to open vascular surgery, especially in severe venous disease. An increased amount of energy delivered to the IPV is highly important in achieving anatomical success.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.