
Abstract
Objectives
EndoAnchors have been used to address proximal aortic neck complications including type Ia endoleaks and endograft migration after endovascular aortic aneurysm repair (EVAR).
Methods
The study population included 100 patients with one-year follow-up in the ANCHOR study. A primary cohort (N = 73) comprised patients who underwent EndoAnchor implantation at the time of an initial EVAR and a Revision cohort (N = 27) included patients treated remote from EVAR. A hostile neck was defined for neck length <10 mm, neck diameter >28 mm, angulation >60°, conical configuration or significant mural thrombus or calcium.
Results
Baseline anatomy included neck length of 17 ± 14 mm, diameter of 27 ± 5 mm, and angulation of 35 ± 18°; 83% of patients had hostile necks. Over 18 ± 4 months of clinical follow-up, six patients (6%) underwent aneurysm-related reinterventions. There were no aneurysm ruptures. Over 13 ± 2 months of imaging follow-up, freedom from type Ia endoleak was 95% in the Primary Arm and 77% in the Revision Arm (P = .006). Aneurysm sacs regressed > 5 mm within one year in 45% of the Primary cases and in 25% of the Revisions. Aneurysm expansion > 5 mm occurred in one revision patient.
Conclusion
Despite a high frequency of hostile neck anatomy, proximal neck complications were relatively infrequent after EndoAnchor use.
Introduction
Endovascular aortic aneurysm repair (EVAR) has replaced traditional open surgery as the most commonly performed technique for repairing infrarenal abdominal aortic aneurysms.1,2 The procedure has proven to be safe, with reductions in perioperative morbidity and mortality compared to open surgical repair.3–7 Nevertheless, complications can and do develop at the proximal aortic neck, where adequate fixation and sealing must endure to prevent type Ia endoleak and endograft migration and thereby achieve long-term protection from aneurysm rupture.8–10 The risk of failure at the infrarenal aortic neck is, in part, dependent on its anatomic configuration. Complications are most common when the neck is short, angulated, of large diameter, conical in configuration, or contains significant mural thrombus or calcium.11–13
The Aptus Heli-FX EndoAnchor System (Aptus Endosystems, Sunnyvale, CA, USA) was developed to improve the performance of endograft fixation and seal to the aorta and, as such, holds potential to improve outcome in patients with challenging proximal aortic neck anatomy.14,15 The objective of the helically shaped EndoAnchors is to tack the endograft to the wall of the aortic neck, simulating a hand-sewn surgical stitch. Multiple, circumferential application of EndoAnchors within the neck can achieve the strength of a surgical anastomosis. 16 The Aneurysm Treatment using the Heli-FX Aortic Securement System Global Registry (ANCHOR) study was designed to evaluate clinical and imaging outcome after EVAR with EndoAnchors, deploying EndoAnchors prophylactically at the time of primary EVAR or therapeutically when proximal neck complications arise immediately after endograft deployment or over long-term follow-up. The early results of the Heli-FX system have been satisfactory. The ultimate clinical utility of the device requires longer-term assessment in this regard. This report details the outcome of the first 100 study patients with available one-year core laboratory imaging follow-up.
Methods
ANCHOR is a prospective multinational trial begun in 2012 and includes 43 US and European centers that comprise a mix of academic medical centers, teaching and non-teaching hospitals, and a variety of vascular specialties (Appendix 1). The study was registered on ClinicalTrials.gov (NCT01534819). Institutional Review Board or Ethics Committee approval was obtained at each site. The enrolled patients provided written informed consent, either prior to the index procedure or within 30 days thereafter if EndoAnchor use was not planned preoperatively. Patients were divided into two subsets; those treated at the time of an initial EVAR procedure (“primary arm,” 73 patients) and those treated for type Ia endoleak and/or endograft migration remote from endograft implantation (“revision arm,” 27 patients). Each treatment arm was further subdivided by indications for EndoAnchor use, and six subsets were analyzed; primary cases preformed prophylactically to prevent type Ia endoleak or endograft migration (62), primary cases with type Ia endoleak (10) or endograft distal misdeployment (1), and revision cases performed for endoleak alone (11), endoleak with endograft migration (8), or for migration alone (8).
Eligibility criteria were broad in spectrum and postoperative follow-up was left to the local standard of care to reflect current practice patterns and to allow a variety of surveillance techniques. Briefly, patients were eligible for inclusion in the study if they underwent implantation of a commercially available endograft constructed of fabric that passed testing to assure that it would not tear after EndoAnchor penetration. Details of the trial design have been described elsewhere. 17 For the current one-year report, patients were eligible for inclusion when core laboratory-assessed imaging studies were available within or beyond the one-year window (360 days ± 90 days).
Sites entered trial data into a web-based electronic data capture system (MedNet Systems, Minnetonka, MN, USA). Data were remotely monitored (Syntactx, New York, NY, USA). Safety endpoints were assessed by an independent medical monitor and computed tomographic (CT) images were evaluated by an independent core laboratory (Syntactx, New York, NY, USA) using a three-dimensional centerline reformatted imaging application (TeraRecon, Foster City, CA, USA). Standard imaging definitions were employed. A conical proximal neck was one in which neck diameter increased 10% or more over the first 10 mm of length beyond the lowest main renal artery. A hostile proximal aortic neck was considered to be one where core laboratory measurements identified one or more of the following criteria: neck length less than 10 mm, neck diameter exceeding 28 mm, infrarenal angulation more than 60°, a neck conical in configuration or one that contained significant mural thrombus or calcium (>2 mm average mural thickness as measured on CT). 11
Type Ia endoleaks were tabulated on a cumulative basis rather than at the one-year snapshot. Patients with endoleaks on any CT or duplex ultrasound performed between the index procedure and one year were counted as having an endoleak, irrespective of whether it resolved at subsequent imaging studies. EndoAnchor-related reinterventions were defined as any reintervention performed for type Ia endoleak, endograft migration, EndoAnchor fracture or malfunction of any component of the Heli-FX system. Aneurysm-related reinterventions were defined as any reintervention performed to address complications that arose within 30 days of the index procedure or within 30 days of a prior aneurysm-related reintervention. Aneurysm-related interventions also included procedures performed for malfunction of the endograft, for any type of endoleak, for endograft migration, or for endograft thrombosis. Aneurysm-related death was defined as any death within 30 days of the index procedure or within 30 days of an aneurysm-related reintervention, or death from rupture.
Continuous variables are expressed as mean and standard deviation. Categorical endpoints are represented as the number of patients triggering the endpoint divided by the number of patients with the endpoint measurement available. Differences in continuous variables were evaluated with the Student’s t-test and categorical variables were assessed with Fisher’s exact test. Freedom from endoleak was calculated with Kaplan–Meier methodology using 95% confidence intervals (CI) and groups were compared with the log-rank test. P-values were considered to be significant when the two-tailed alpha was less than .05.
Results
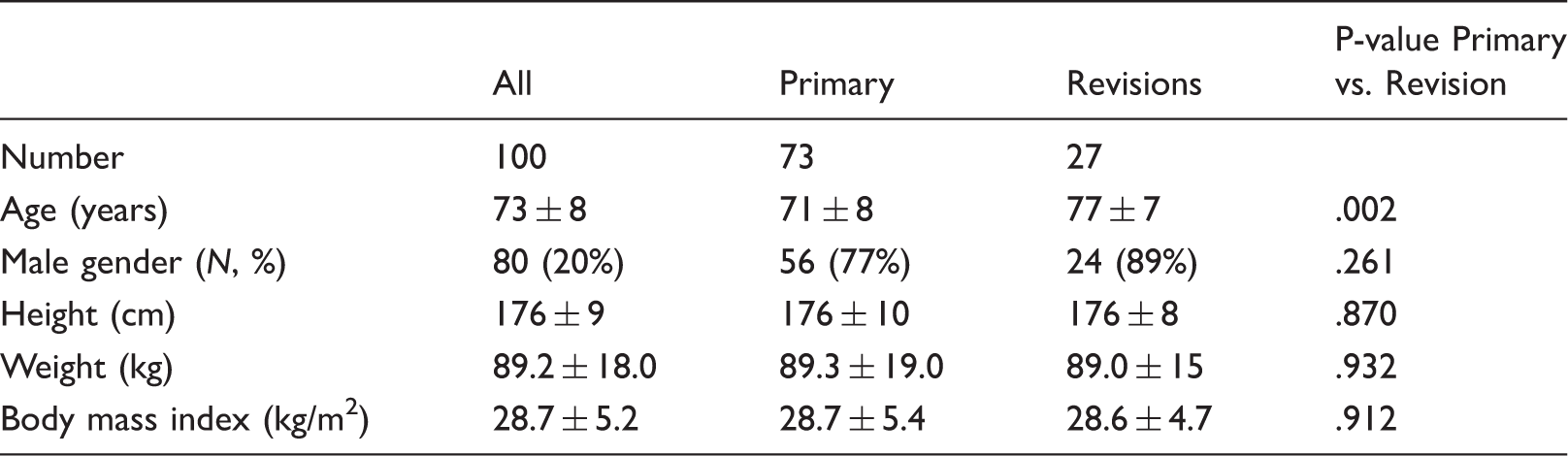
Baseline demographics by indication for EndoAnchor use.
Types of endografts.

Baseline anatomic characteristics
Baseline anatomic characteristics (core laboratory analysis) by indication for EndoAnchor use.
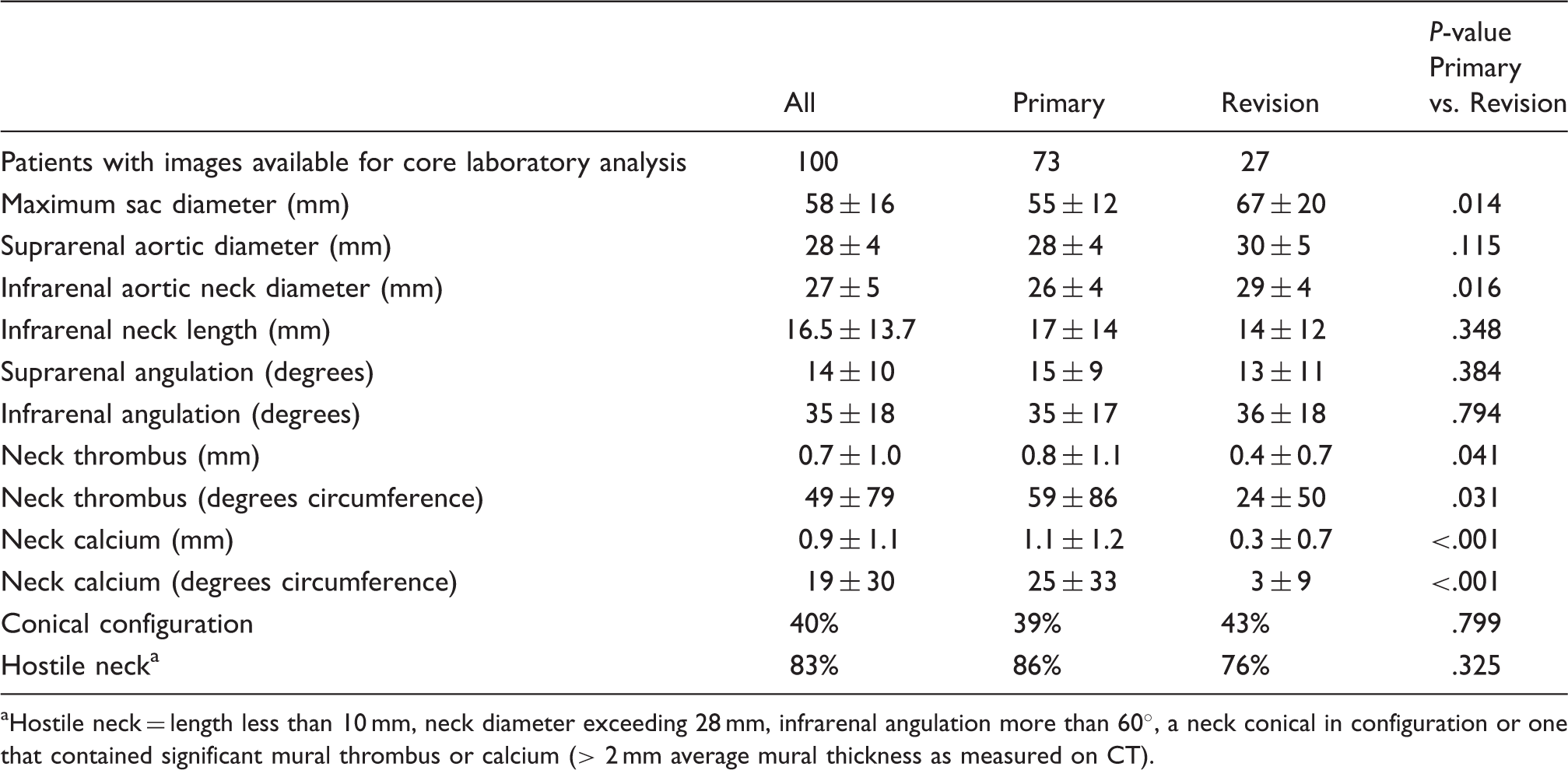
Hostile neck = length less than 10 mm, neck diameter exceeding 28 mm, infrarenal angulation more than 60°, a neck conical in configuration or one that contained significant mural thrombus or calcium (> 2 mm average mural thickness as measured on CT).
Index procedure and hospitalization
Details of the index procedure and the initial hospitalization.
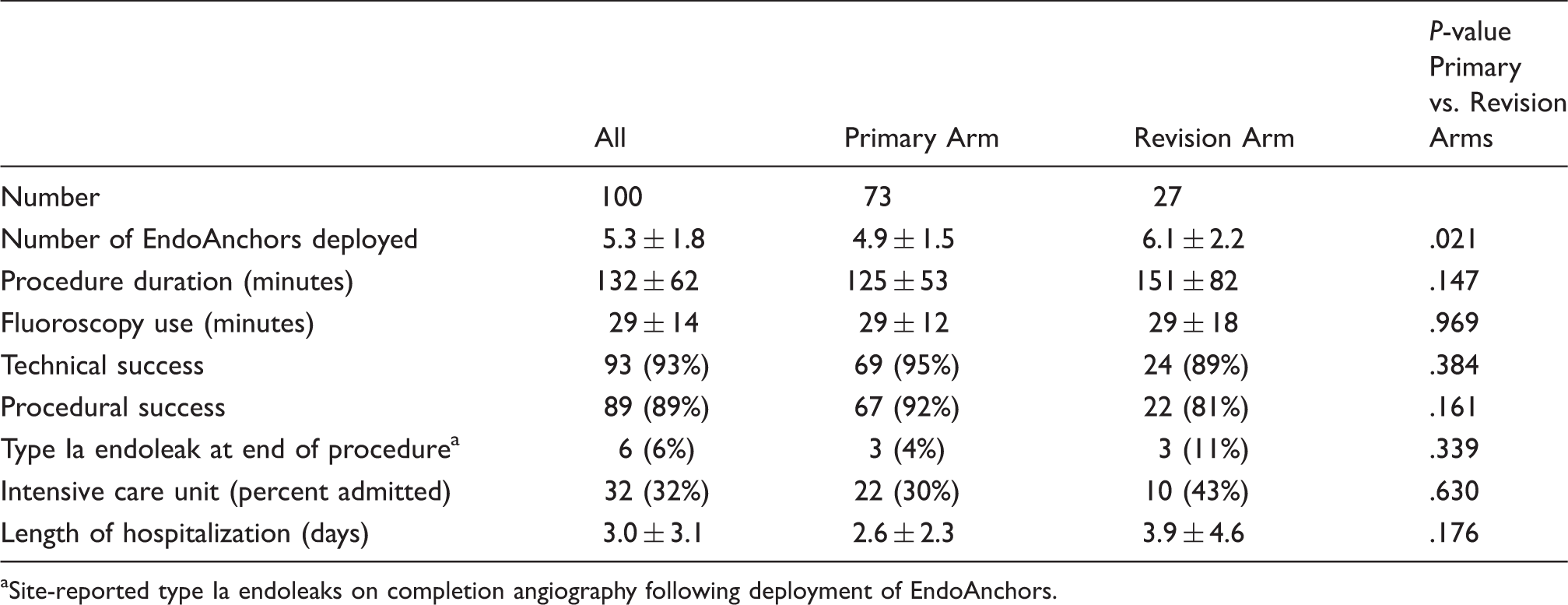
Site-reported type Ia endoleaks on completion angiography following deployment of EndoAnchors.
Technical success for EndoAnchor deployment was reported by the operators in 93 patients (93%); 69/73 (95%) and 24/27 (89%) in the Primary and Revision cases, respectively. Inadequate EndoAnchor penetration into the aortic wall accounted for six of the seven technical failures and one patient had failure of EndoAnchor deployment. The mean number of EndoAnchors with inadequate penetration was 2.0 ± 1.5 (range 1–5) in the six patients. At the same time, these patients had satisfactory aortic penetration of 5.7 ± 2.1 (range 3–9) EndoAnchors.
Site-reported type Ia endoleaks were evident at completion angiography in six patients (6%). The frequency of type Ia endoleaks appeared lower in Primary cases (3/73, 4%) compared with Revisions (3/27, 11%) but this difference did not attain statistical significance (P = .339). The 30-day mortality in the 424 patients enrolled in the series was 7/424 (1.7%). None of the deaths occurred from an EndoAnchor or endograft-related complication. Comparing the current 100-patient cohort to the 324 patients enrolled in ANCHOR who were not followed for one year, there were no differences in the rates of procedural success, technical success, type Ia endoleaks at completion angiography, or aneurysm-related reinterventions through 30 days.
One-year outcome
Clinical outcome over follow-up.
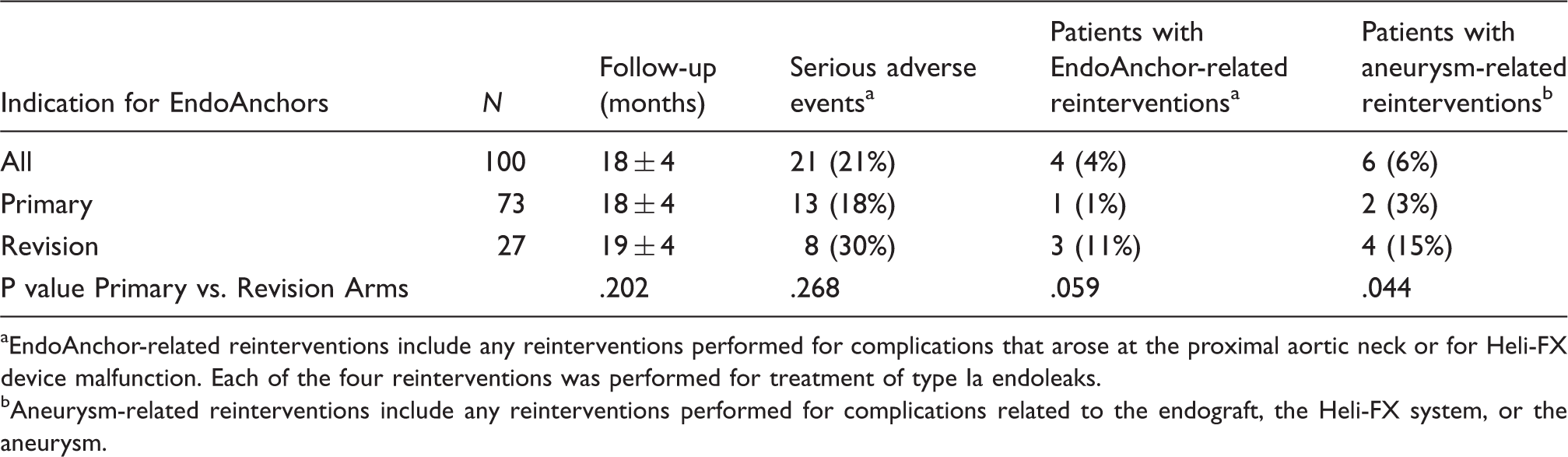
EndoAnchor-related reinterventions include any reinterventions performed for complications that arose at the proximal aortic neck or for Heli-FX device malfunction. Each of the four reinterventions was performed for treatment of type Ia endoleaks.
Aneurysm-related reinterventions include any reinterventions performed for complications related to the endograft, the Heli-FX system, or the aneurysm.
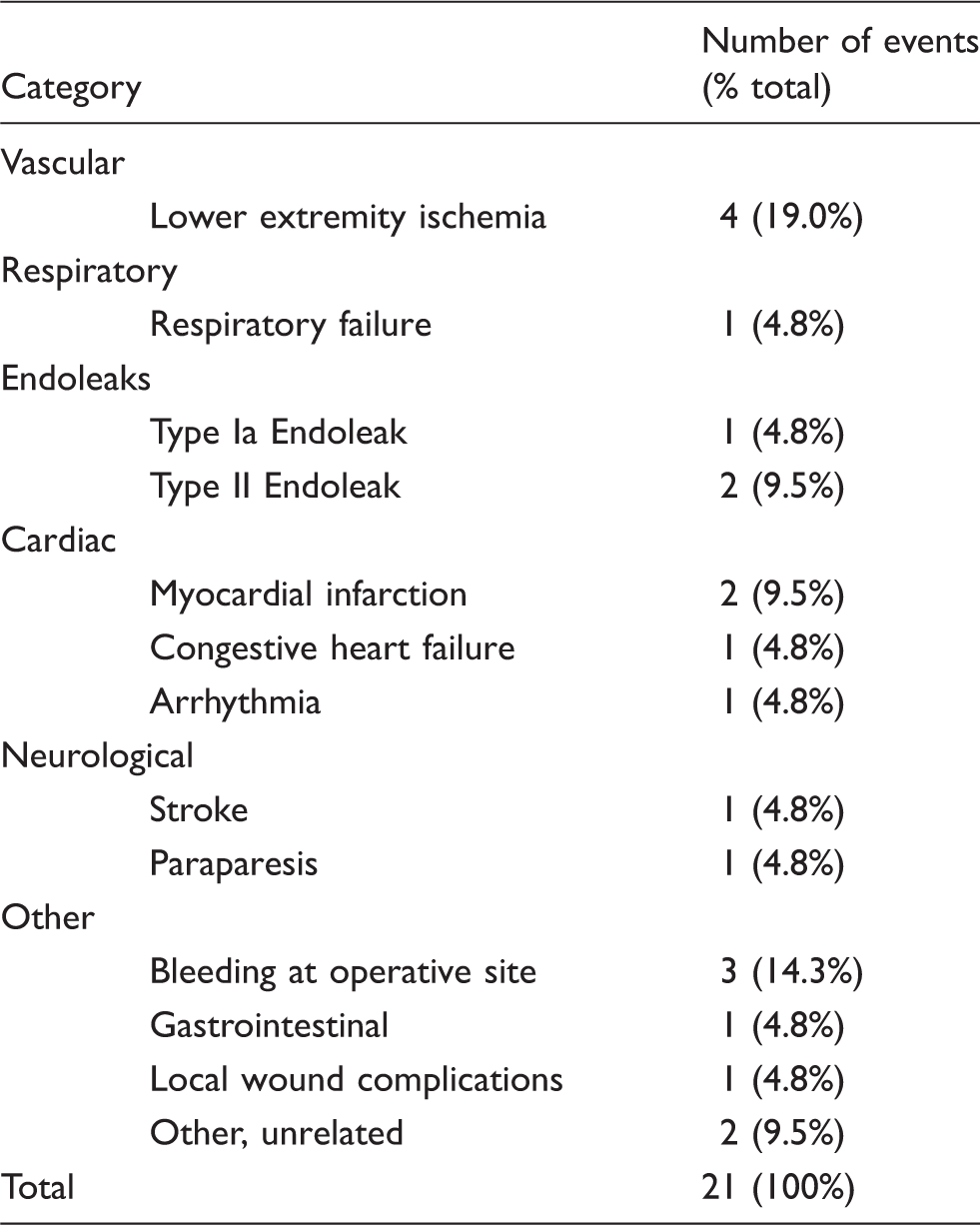
Site-reported serious adverse events over follow-up.
Imaging outcome (core laboratory reported).
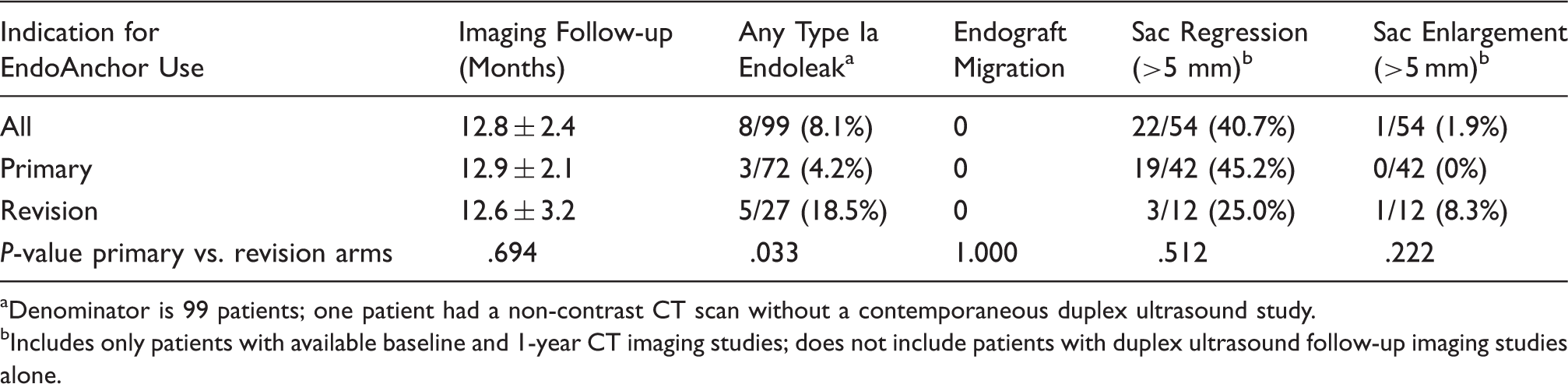
Denominator is 99 patients; one patient had a non-contrast CT scan without a contemporaneous duplex ultrasound study.
Includes only patients with available baseline and 1-year CT imaging studies; does not include patients with duplex ultrasound follow-up imaging studies alone.
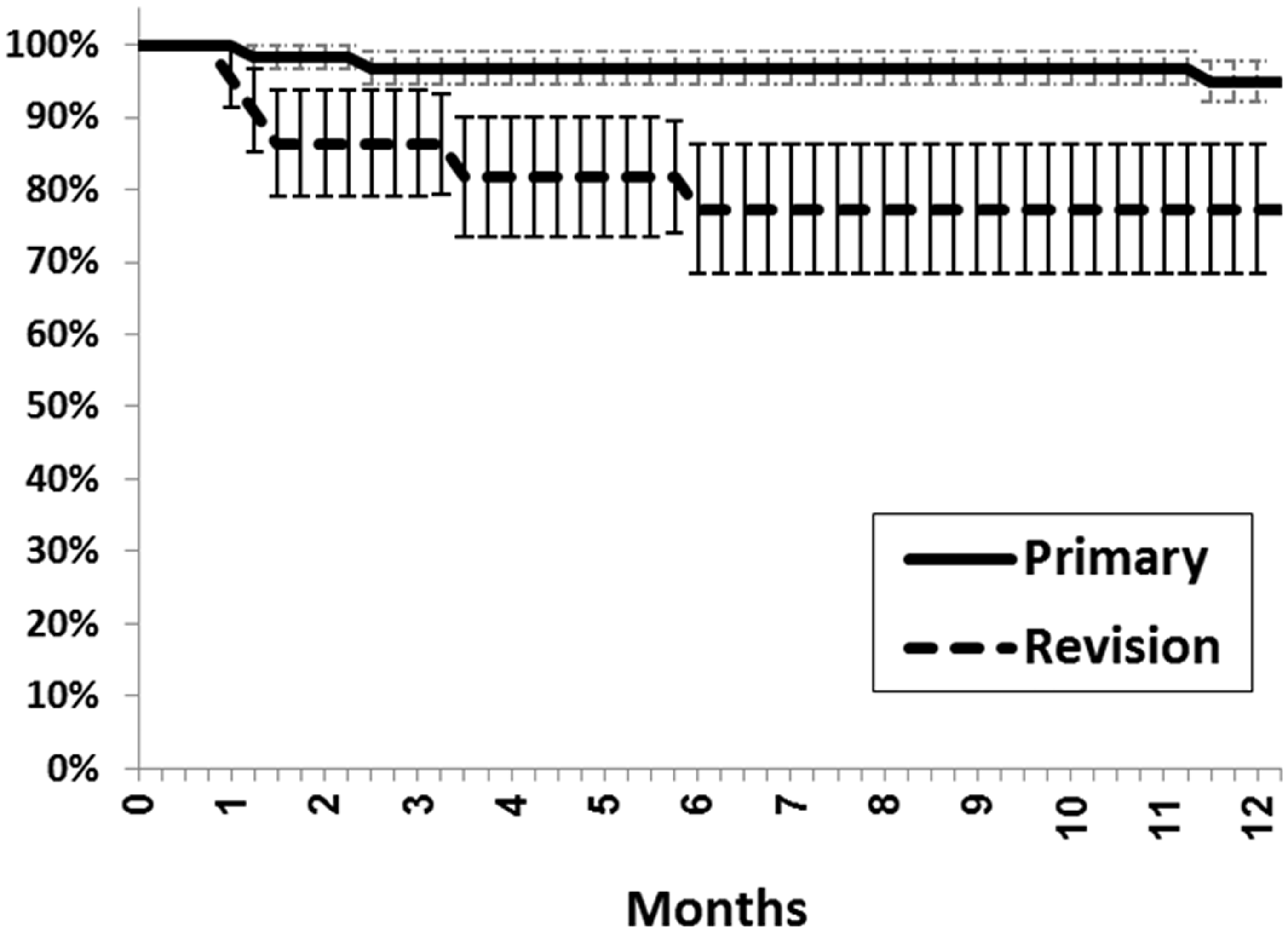
Kaplan–Meier estimates of freedom from type Ia endoleak after the index procedure. Bars indicate the standard error of the estimate. The P-value of the difference between the two curves is .006.
Aneurysms regressed more than 5 mm in diameter in 41% of patients with CT imaging at a suitable baseline time point and at one year. The one-year rate of sac regression was 45% in the Primary Arm and 25% in the Revisions (P = .512). Aneurysm sac enlargement greater than 5 mm through one-year of follow-up was observed in one patient (1.9%). This patient was in the Revision Arm and had a type Ia endoleak with a 4 mm gap between the endograft fabric and the aortic wall that precluded penetration of EndoAnchors at this location. The one year CT and angiography images confirmed inadequate EndoAnchor penetration of the aortic wall at the location of the endoleak.
Infrarenal aortic neck diameter increased more than 3 mm in 10/76 (13.2%) patients with assessable CT images at baseline and follow-up. Suprarenal neck dilatation more than 3 mm occurred in a single patient (1.3%). There was a mild negative correlation between the baseline infrarenal neck diameter and the change over time (r = −.196). Smaller diameter necks trended toward a greater increase in neck diameter over time, but this relationship did not attain statistical significance (P = .090). Infrarenal neck dilatation was unrelated to the frequency of type Ia endoleaks over follow-up.
Discussion
While endovascular aneurysm repair has surpassed traditional open surgery as the preferred method for treating infrarenal abdominal aortic aneurysms,1,2 challenging proximal aortic neck anatomy remains a limiting factor.11,12 Identification of unfavorable neck anatomy during preoperative imaging evaluation may preclude the use of endovascular solution, forcing the clinician to consider an invasive open surgical strategy.18,19 Clinical outcome may be compromised when endovascular repair is performed in the presence of challenging neck anatomy, with a higher rate of early and late type Ia endoleak and, 11 in at least one review, aneurysm-related mortality. 12
With recognition of the difficulties imposed by hostile aortic neck anatomy, endograft designs have been modified over the years in an effort to better adapt to anatomic variability.20–22 Suprarenal bare stents, attached barbs and hooks, and polymer-injected sealing rings have been employed alone and in combination to decrease the risk of aortic neck-related complications. The Heli-FX system with EndoAnchors represents a unique device quite different from other strategies. Noting the long-term durability of open surgical hand-sewn anastomosis and recognition of the necessity to place sutures into the adventitial layer, EndoAnchors were designed to fully penetrate through the intimal and medial layers of the aortic wall to reach the adventitia.14,16
Like most new technology, the initial studies of active endograft fixation devices were anecdotal. 23 The publication of data from relatively small, single center retrospective studies appeared next,24,25 followed by the acquisition and dissemination of short- and mid-term results from prospective, multicenter investigations.15,26 As is often the case, patient follow-up was limited in the first publications. Nevertheless, the available data documented early success of EndoAnchors, alone or in combination with aortic extender cuffs, for the treatment of existing endoleaks, endograft migration, and endograft distal maldeployment. Better documentation awaited the availability of longer-term follow-up data, particularly imaging studies.
The current analysis comprises one-year clinical and core laboratory imaging follow-up on 100 patients. One limitation of the current analysis relates to the possibility that the smaller 100-patient subset of ANCHOR patients is not entirely representative of the larger study as a whole. While the ultimate value of EndoAnchors will require long-term data on the larger study population, these data provide some evidence of clinical utility. Treatment of existing problems, particularly type Ia endoleaks, appears durable at least through one year of follow-up. Importantly, the current data provide more robust evidence for the value of EndoAnchors for prophylactic indications. Early data in this subgroup were less compelling, noting the time-dependence of proximal neck complications. The one-year results furnish data that may be more comparable to that from published reviews on the natural history of endovascular repair in patients with unfriendly aortic neck anatomy. Comparison of the published historical control data-sets is more appropriate with respect to similarities of the study populations as well as similar lengths of patient follow-up. The use of a core laboratory in the ANCHOR, however, may impart increased sensitivity for detecting therapeutic failures, particularly related to the identification and classification of post-procedure endoleaks.
The current study documents absence of type Ia endoleak in the majority of patients treated with EndoAnchors. Predictably, outcome was related to the indication for EndoAnchor use and was best in patients in the Primary Arm. It is also axiomatic that patients who presented with very short aortic neck length had a higher frequency of type Ia endoleak over follow-up. Absent a concurrent control data-set, the results of the ANCHOR study can only be compared to prior published data. There are two systematic reviews that summarize the results of endovascular repair in patients with hostile neck anatomy. The review of Antoniou and colleagues reported a 10% type Ia endoleak rate at one year, 12 while the review of Stather et al. found a rate of 12.6%; 5.8% prior to 30 days, and 6.8% thereafter. 27 The 4.2% point estimate and the 4.8% Kaplan–Meier estimate at one year in the ANCHOR data-set appear lower than prior published data. These differences, however, should be considered in the context of the ANCHOR trial design which differs from that of the retrospective published reviews. ANCHOR included prospective enrollment, core laboratory analysis, and remote site monitoring on one hand, with exclusion of intraoperative angiographic endoleaks and, in some cases, shorter follow-up on the other.
One of the failure modes of endovascular repair is endoleak or graft migration from postoperative aortic neck dilatation.28–33 Neck dilatation may be related to the radial force of a self-expanding stent, but neck dilatation is also observed after traditional open surgical repair. The current data provide evidence that neck dilatation is related to the intervention, since infrarenal neck dilation was unaccompanied by suprarenal aortic diameter enlargement. Intuitively, EndoAnchors may decrease the degree of neck dilatation to the extent that might progress beyond the nominal diameter of the endograft. The 13% frequency of neck diameter dilatation in ANCHOR compares favorably with data from the literature with reported rates of 17–28%.29,30,32 The negative correlation between neck diameter and neck dilation contrasts with data from Illig in patients undergoing open repair. In that series, neck dilation was most common in necks larger than 27 mm. 34 The current study results may reflect a greater degree of endograft oversizing in patients with smaller necks, but a definitive explanation is not possible with the available data.
Conclusion
In summary, the one-year results of the ANCHOR registry suggest that EndoAnchors can be beneficial in patients undergoing primary endovascular repair or when proximal neck complications arise postoperatively. Outcome was better in the Primary cases but 77% of Revision cases remained free from type Ia endoleaks through one year. While further conclusions await the availability of long-term data, the observation that few failures occur beyond the first month of follow-up imparts optimism for the ultimate value of the therapy.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Ouriel is an employee and shareholder of Syntactx which received research fees from Aptus Endosystems.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Aptus Endosystems, the manufacture of the study device.