
Abstract
Objective
The mechanisms of contrast-induced nephropathy are not fully understood and sensitive biomarkers of contrast-induced nephropathy are yet to be found. We investigated whether urinary fibrinogen could be a potential biomarker for contrast-induced nephropathy.
Methods
To create a contrast-induced nephropathy model, mice received a prostaglandin synthesis inhibitor (indomethacin) and a nitric oxide synthase inhibitor (Nω-Nitro-L-arginine methyl ester) intraperitoneally followed by a different dose of iodixanol. In the control group, normal saline was administered. Urinary fibrinogen and serum creatinine were analyzed using enzyme-linked immunosorbent assay. Kidneys were used to quantify fibrinogen using qRT-PCR and Western blot and for histopathological examination.
Results
Histopathological examination demonstrated mild renal injury in the low-dose group, and moderate renal injury in the high-dose group. Urinary fibrinogen levels were significantly increased in an iodixanol dose-dependent manner (control vs. low-dose group, P < 0.05; control vs. high-dose group P < 0.01). Serum creatinine levels were only increased in the high-dose group (P < 0.01 compared to control), but not in the low-dose group. For fibrinogen-gene expression, in the low-dose group, Fgγ increased (qRT-PCR, Western blot, P < 0.05) in the high-dose group, Fgβ and Fgγ decreased (qRT-PCR, P < 0.01; Western blot, P < 0.05), and Fgα increased (qRT-PCR, P < 0.05; Western blot, P < 0.05).
Conclusions
We propose that urinary fibrinogen could be used as a potential biomarker for early contrast-induced nephropathy diagnosis.
Introduction
Contrast-induced nephropathy (CIN) is the third leading cause of hospital-acquired renal failure, which is a common complication following intravascular contrast imaging studies and endovascular procedures. The mechanisms of CIN are not fully understood. One of the main hypotheses is the potential direct cytotoxicity of intravascular contrast media (CM). It is suggested that the direct cytotoxicity of CM is mainly from its iodine component. 1 Some other properties, such as osmolality, viscosity, and ionic strength, may also contribute to the toxicity of the CM. Kidney tissue ischemia/reperfusion injuries secondary to renal vasoconstriction induced by CM is another possible cause of CIN.1–3 Serum creatinine (SCr) and blood urea nitrogen (BUN) are the most common biomarkers used for detecting kidney injury and dysfunction in the clinical settings, but there are significant limitations in terms of their sensitivity and specificity. 4 Fibrinogen (Fg) is a soluble plasma glycoprotein, which can be converted into fibrin by thrombin during blood clot formation. There are reports indicating that urinary fibrinogen (UFg) can be used as a biomarker of acute kidney dysfunction due to ischemia/reperfusion injury. 4 The objective of this study was to investigate whether UFg can serve as a potential biomarker for CIN in its early diagnosis and follow up.
Materials and methods
CIN animal model
Normal C57BL/6 J mice, JAX stock number 000664, were utilized. Seven-week-old male mice (urine specimen collection is much easier and accurate in male mice) were obtained (Jackson laboratory, Maine, United States) and accommodated in the central animal facility at our institution for one week before the experiments. They were caged with free access to food and water under conditions of 21 ± 1℃ and 50% to 80% relative humidity at all times in an alternative 12 h light-dark cycle. All animal maintenance and treatment protocols were in compliance with the guide for care and use of laboratory animals as adopted and promulgated by the national institutes of health (NIH), and were approved by the animal care and use committee at our centre.
The CIN animal model was induced by administration of the CM, iodixanol (IDX) (Visipaque) (GE Health Inc., Little Chalfont, Buckinghamshire, United Kingdom), following inhibition of prostanoids and nitric oxide synthesis, which has been widely used.5–8 Eight-week-old C57BL/6 J mice were injected with a prostaglandin synthesis inhibitor (indomethacin, 10 mg/kg) and a nitric oxide synthase inhibitor (Nω-Nitro-L-arginine methyl ester, L-NAME, 10 mg/kg) intraperitoneally (ip) within a 15-min interval of each other. After another 15 minutes, IDX was ip injected into the mice at the doses of 6.24 gI/kg (n = 7) (low-dose group) and 12.48 gI/kg (n = 9) (high-dose group). In the control group, normal saline (NS) solution, instead of IDX, was injected into the mice (n = 6). The animals were sacrificed 24 h after the administration of the CM. Kidneys were harvested and cut sagittally. The specimens were then placed into labelled cassettes with 10% neutral formalin fixation for 24 h at room temperature. Half of each kidney was then embedded into paraffin for histological examination. The other kidney halves that were supposed to be used for protein extraction were snap frozen in liquid nitrogen and stored in a−80℃ refrigerator. The rest of each kidney specimen was used for RNA extraction and was placed into an RNAlater (Ambion) at 4℃ overnight and subsequently stored in a −80℃ refrigerator.
Histopathology evaluation
Histopathology examination was performed as described by Hoffmann et al. 4 Briefly, the embedded tissues were cut into 5 µm sections and stained with Hematoxylin and Eosin (H&E) stain. The histopathological damage was evaluated under a light microscope by a pathologist, who was blinded to the study groups. Grading scales of 0–3 were used to grade the severities of histopathological damage in the kidneys: 0, normal to minimal tubular injury; 1, mild acute tubular injury (slight tubular distension, a low epithelial lining, and nonspecific degenerative changes of the epithelial cells); 2, moderate acute tubular injury (frequent single cell necrosis within the epithelial layer); and 3, severe acute tubular injury (presence of widespread epithelial cell necrosis, low epithelial lining, and accumulation of cellular debris in the tubule lumens).
SCr level analysis
Mice serum specimens were collected 24 h after the start of experiments (Day 1) and before the mice were sacrificed. SCr was measured using a creatinine assay kit (BioVision, Milpitas, CA). Results are represented as means ± standard deviation (SD).
Urine fibrinogen level analysis
Mice urine samples were collected on Day 1. Urine fibrinogen (Fg) levels were assessed by a mouse Fg enzyme-linked immunosorbent assay (ELISA) kit (Assaypro, Saint Charles, MS). Results are represented as means ± SD.
Quantitative real-time polymerase chain reaction
Kidney samples were taken out from the RNAlater, and a slice from each sample was cut off and weighed. The total RNA of the specimen was isolated using an RNeasy mini kit (QIAGEN, Valencia, CA). First-strand cDNAs were synthesized from total RNA by reverse transcription (1 µg total RNA in 20 µl of reaction volume) using the iScript cDNA synthesis kit (Bio-Rad Laboratories, Hercules, CA) primed with oligo dT and random hexamer primers. SsoFast EvaGreen Supermix (Bio-Rad Laboratories, Hercules, CA) was used for dye-based detection. Reactions were conducted in a CFX96 Touch™ real-time polymerase chain reaction (PCR) detection system (Bio-Rad Laboratories, Hercules, CA). Fluorescence was monitored during every PCR cycle at the annealing step. The primers for the adenosine receptors were: Fgα, 5′-TGT GGA GAG ACA TCA GAG TCA ATG-3′ (forward), 5′-CGT CAA TCA ACC CTT TCA TCC-3′ (reverse); Fgβ, 5′-CTA TGG CTG CTGCTG CTA TTG-3′ (forward), 5′-GGC TCT TCC TTT CTC CTG TCA AC-3′ (reverse); Fgγ, 5′-TGT GGC TAC CAG AGA TAA CTG TTG-3′ (forward), 5′-ATG TCT TCC AGC GTT CGG AG-3′ (re-verse); GADPH: 5′-GAG TCA ACG GAT TTG GTC GT- 3′ (forward), 5′-TTG ATT TTG GAG GGA TCT CG-3′ (reverse). PCR conditions were as follows: 95℃, 30 s; (95℃, 2 s; 55℃, 2 s) × 40 cycles; 60℃, 1 min; Melt curve: 65℃–95℃ in 0.5℃ interval, 2 s/step. Results were analyzed with a Bio-Rad CFX manager. Results for all experiments represent triplicate determinations, and are described as means ± SD.
Western blot analysis
Kidney samples were homogenized in RIPA buffer (150 mM NaCl, 1% Triton X 100, 0.5% Sodium deoxycholate, 0.1% SDS, 50 mM Tris-Cl pH 8.0 supplemented with 2 µg/mL of aprotinin, 2 µg/mL of leupeptin, 40 µg/mL of phenylmethylsulfonyl fluoride). Protein in the samples was extracted. A total of 10–20 µg of proteins were separated on a 10% SDS-polyacrylamide gel and transferred to a polyvinylidene difluoride membrane (Bio-Rad Laboratories, Hercules, CA). The membrane was incubated for 1 h at room temperature in a block buffer (TBS containing 0.03% Tween 20 and 5% fat-free milk power). The blots were probed with antibodies specific to Fg full length (Abcam, Cambridge, MA) or GAPDH (Santa Cruz Bio-technology, Santa Cruz, CA) at 4℃ overnight, respectively. Membranes were washed three times at 10 min per washing with 0.03% Tween 20 in TBS, and then incubated with the secondary antibody for 1 h at room temperature. Following this, membranes were washed three more times and developed using ECL Western Blotting Substrate (Thermo Scientific, Waltham, MA).
Statistical analysis
The changes in RNA and protein expression of the Fgs were statistically analysed with Student’s t-test using Prism software (GraphPad Software, Inc., La Jolla, CA). A P value of < 0.05 was considered statistically significant. Data are expressed as means ± SD.
Results
Histopathology results
H&E stain demonstrated mild renal injury in the low-dose group (scoring 1–2) and moderate renal injury in the high-dose group (scoring 2–3), based on histopathological grading scales from 0 to 3 as described earlier (Figure 1). Mild vacuolar degeneration in the proximal tubule epithelial cells was found in the low-dose group, and extensive vacuolar degeneration was visualized in the high-dose group. Cell flattening and mitosis, which occurs during cell repair, were not found in either group. This indicated that the damage was acute.
Representative images of H&E-stained kidney histology sections of sham, low-dose, and high-dose groups.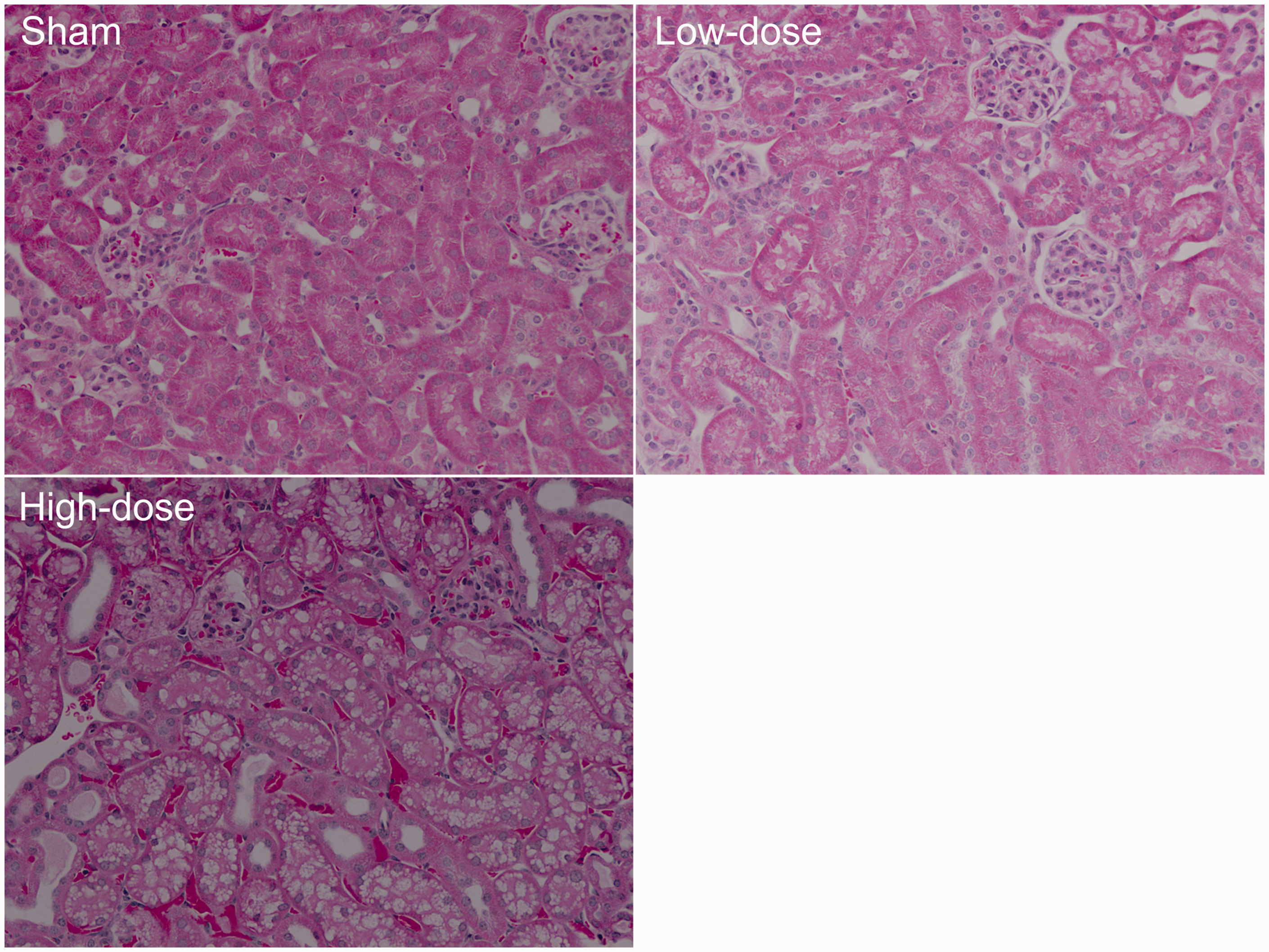
UFg and SCr level
Urine fibrinogen (µg/mg Cr) of low-dose and high-dose iodixanol-treated mice.

Blood creatinine level (mg/dL) of low-dose and high-dose iodixanol-treated mice.

Tissue Fg gene expression results
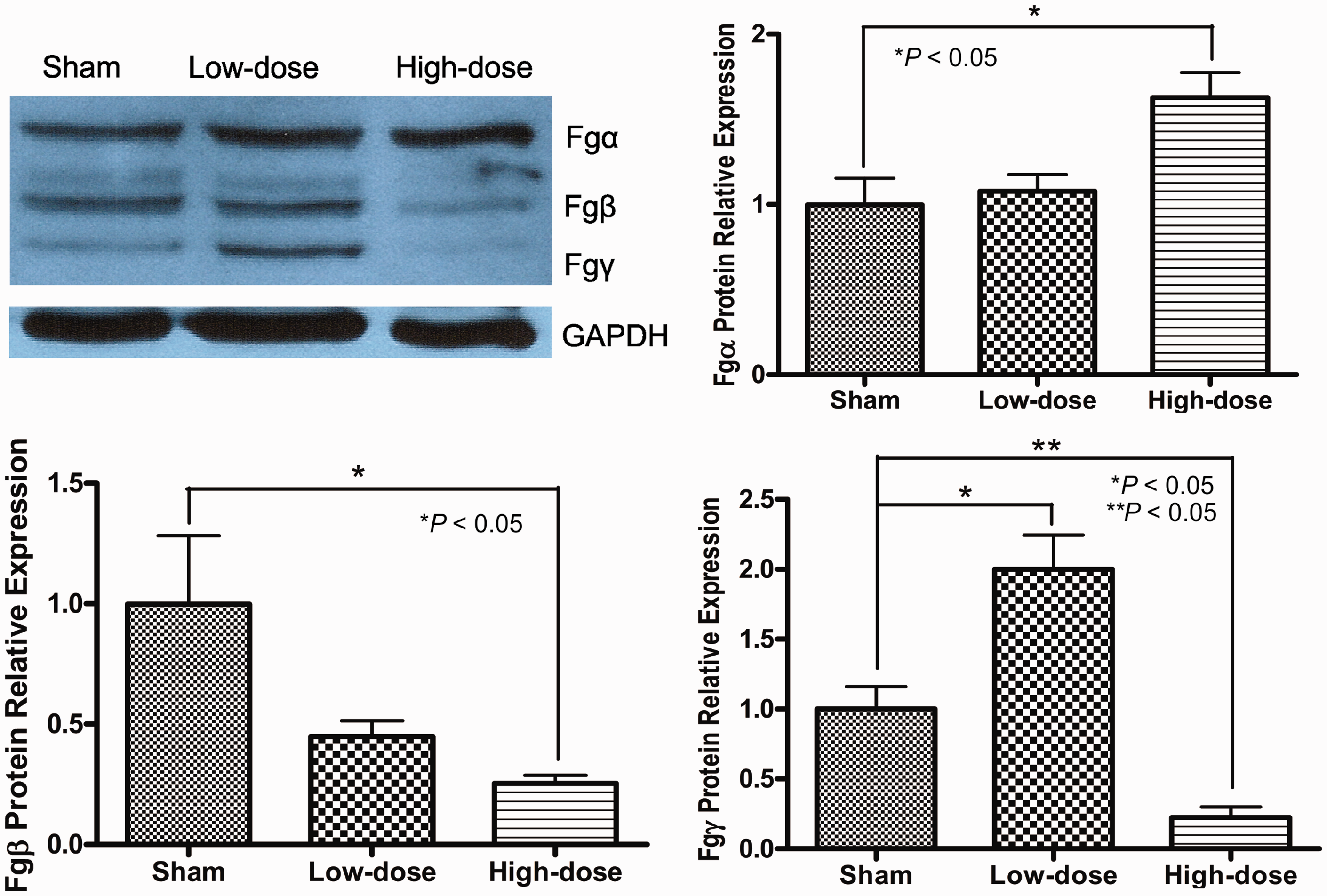
qRT-PCR (Figure 2) and Western blot (WB) (Figure 3) results were consistent and are described as follows: in the low-dose group, Fgγ increased significantly (qRT-PCR, P < 0.05; WB, P < 0.05), with no significant changes of Fgα, Fgβ levels; however, in the high-dose group, both Fgβ and Fgγ decreased significantly (qRT-PCR, P < 0.01; WB, P < 0.05), and Fgα slightly increased (qRT-PCR, P < 0.05; WB, P < 0.05).
Relative mRNA levels of Fgα, Fgβ, and Fgγ of sham, low-dose, and high-dose groups. Representative Western blot results of Fgα, Fgβ, and Fgγ of sham, low-dose, and high-dose groups.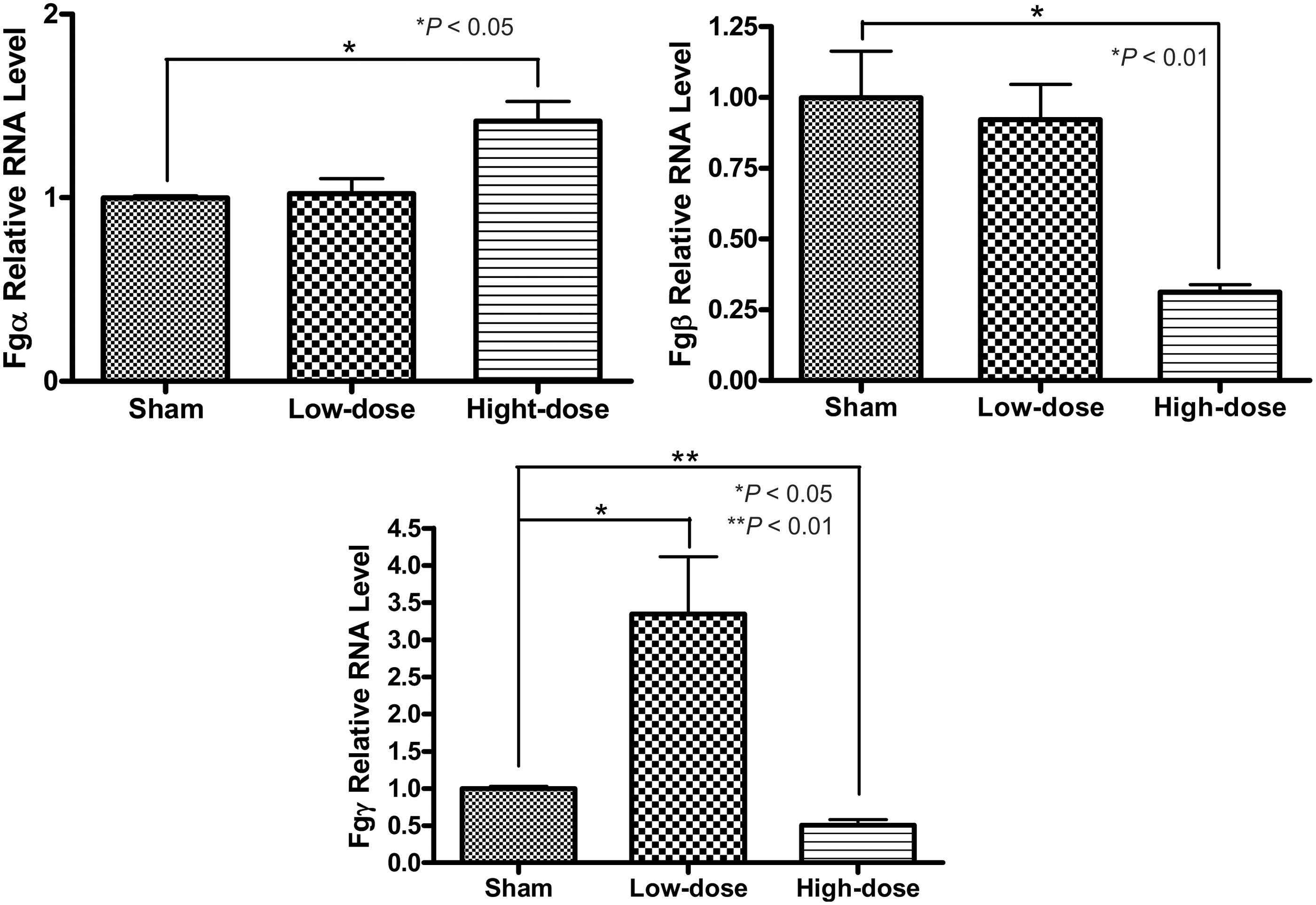
Discussion
CIN is an acute renal insufficiency following the administration of CM. The diagnosis of this disease is mainly based on SCr and BUN levels. Currently, renal function deterioration in CIN is referred to as an increase of SCr concentration of >0.5 mg/dL (44 µmol/L) or 25% above baseline, within 48 h after CM administration. 9 However, elevation of BUN and SCr is a late response, which usually takes 48–72 h to reach the peak levels. It may subsequently delay the diagnosis and management of CIN and result in significant late complications and permanent renal failure.4,10–13 Therefore, it is very important to find a reliable biomarker for early diagnosis and treatment of CIN in real clinical practice.
It has been documented that CIN is not likely to be induced in healthy people, neither in healthy animals.14,15 We used a CIN mouse model based on the idea of inhibiting prostaglandin and nitric oxide syntheses before CM, IDX in our study, administration.6–9 This mimics the real patients with underline renal disease, as the patients with pre-existing kidney insufficiency, which is a major risk factor for CIN, usually have low prostaglandin and nitric oxide levels.16–19
The low and high doses of IDX, 6.24 gI/kg and 12.48 gI/kg, were chosen based on the body weight ratio and skin area ratio extrapolated from human studies, respectively. The 6.24 gI/kg and 12.48 gI/kg doses are equal to 150 ml and 300 ml of IDX applied to a human with an average body weight, respectively. These are the commonly used dosages of IDX in the clinical practice. Although the dosages are significantly higher (when calculating the doses based on Iodine/kg) than that used by others in animal studies, which tends to be 1–3 g iodine/kg, the other researchers used iohexol or iopromide, which are typically considered more nephrotoxic.
The standpoint that IDX is less nephrotoxic is still controversial in the field of CIN studies, but our animal study supported this standpoint; we failed to induce CIN in our animal model when using those low iodine dosages, while other CMs such as iohexol or iopromide could induce CIN. The reason we chose to study IDX was due to the fact that this CM is a new generation iso-osmolar CM which is very popular and most commonly used in clinical practice, but still does not protect the patients from CIN. Future studies revealing the exact mechanism of CIN caused by IDX will be important in establishing CIN animal models and human studies using this agent and will bring more benefits to the clinical practice.
CIN was successfully induced in both low-dose and high-dose CM treatment groups, and dose-dependent severities of renal tubular cell injury were demonstrated. UFg significantly increased in both low-dose and high-dose CM groups in a dose-dependent manner. The level of UFg elevation was consistent with the severity of renal histopathological damages.
Our data also showed that a significant increase of SCr was only detected in the high-dose group, but not in the low-dose group. These findings suggest that UFg, as a potential biomarker, may be more sensitive than SCr in diagnosis and follow-up of renal dysfunction secondary to CIN.
We also performed kidney tissue Fg gene expression analysis. UFg level increased significantly in our CIN model. It was important to find out if Fg gene expression in kidney tissue also increases. Fg has three subunits. Real time PCR and WB results showed that Fgγ significantly increased in low CM dose group from the baseline compared with the control group. Interestingly, in high CM dose group with extensive renal tissue damages, both Fgβ and Fgγ were significantly decreased comparing to that in the control group. We hypothesize that significantly decreased Fgβ and Fgγ in the high-dose group may be due to severe kidney injury, which subsequently decreases the production of Fg. Another finding is that total fibrinogens in kidney tissue are not significantly different and not sensitive enough to serve as a CIN biomarker, while UFg is a good CIN marker. The possibility is that the Fg in CIN is easily released to urine, but not stored in the tissue.
Conclusions
UFg level is significantly increased in CIN murine models, and the degrees of Fg elevation are consistent with the pathological severities of kidney damage. These results suggest that UFg may be a useful biomarker for early diagnosis and follow-up of CIN in the patients with underline renal diseases, who undergo diagnostic angiography or endovascular surgery. Further investigations in the clinical settings are required to validate our findings.
Authors’ contributions
Luyu Yao and Honglin Dong contributed equally to this work and should be regarded as joint first authors. All the authors have contributed towards performing the study and preparation of the manuscript and they all have approved the latest version of the article.
Footnotes
Acknowledgements
The authors would like to thank Ms. Talicia Tarver who provided us editorial assistance. The article was presented at the Society for Vascular Surgery Annual Conference (SVS-2014), 5–7 June 2014, Boston, MA.
Disclosure
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.