
Abstract
Objective
Venous thromboembolism (VTE) is a potentially preventable complication following surgery. There is variation with regard to the most effective mode of prophylaxis. We sought to determine if an aggressive approach to VTE prophylaxis would reduce VTE rates on the inpatient vascular surgical service.
Methods
Vascular inpatients from a single institution from July 2010 to March 2013 were included in the analysis. A protocol for VTE prophylaxis was implemented on the inpatient vascular surgical service in November 2011. This included subcutaneous (SQ) heparin initiation within 24 h of admission unless deemed inappropriate by the attending, as well as intermittent compression devices (ICD) and compression stockings (CS). The rate of VTE was compared prior to and following the intervention. Patients were compared using AHRQ comorbidity categories, APR-DRG severity of illness, insurance status, and principle procedure. T-tests were used to compare continuous variables and chi-square analysis used to compare categorical variables.
Results
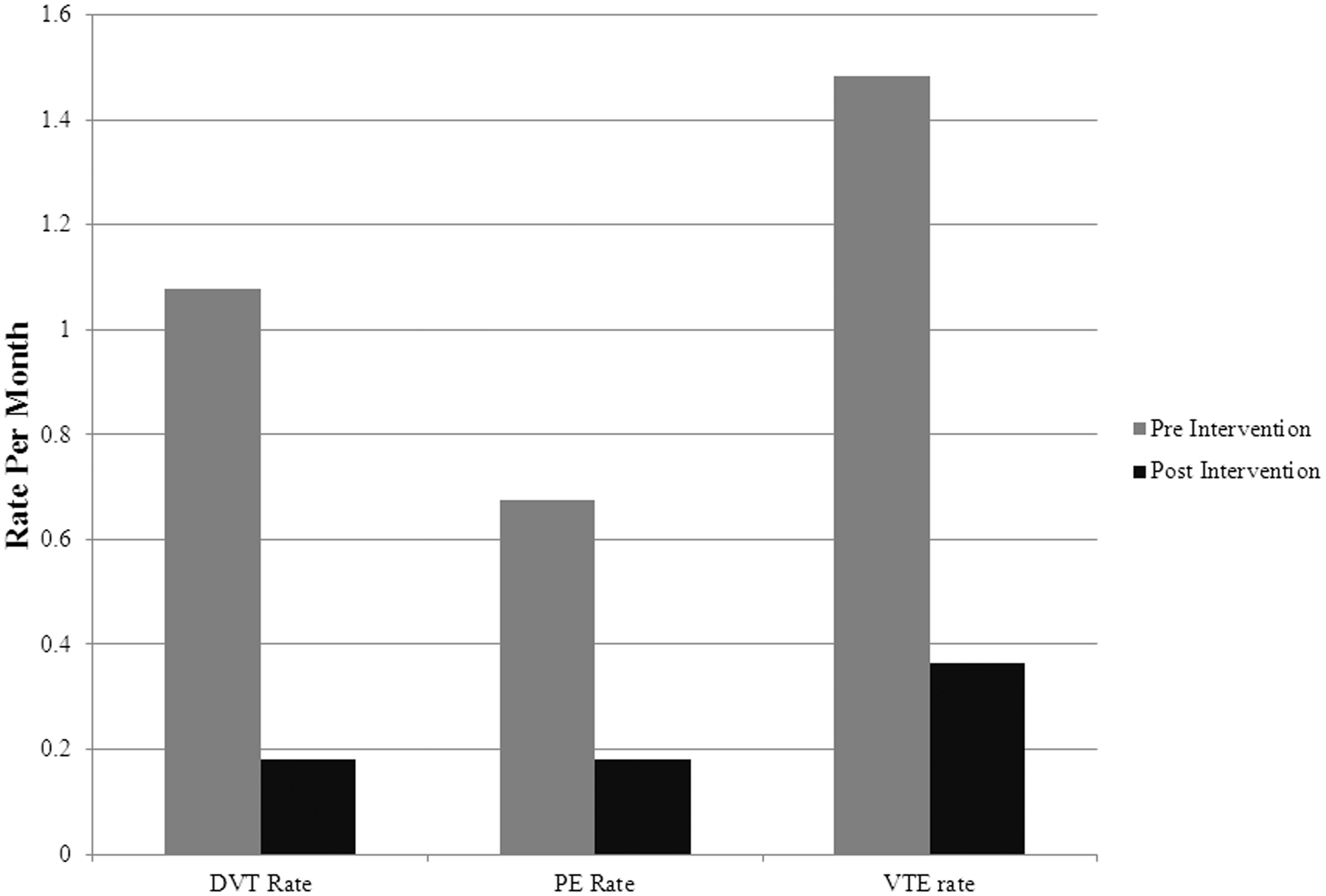
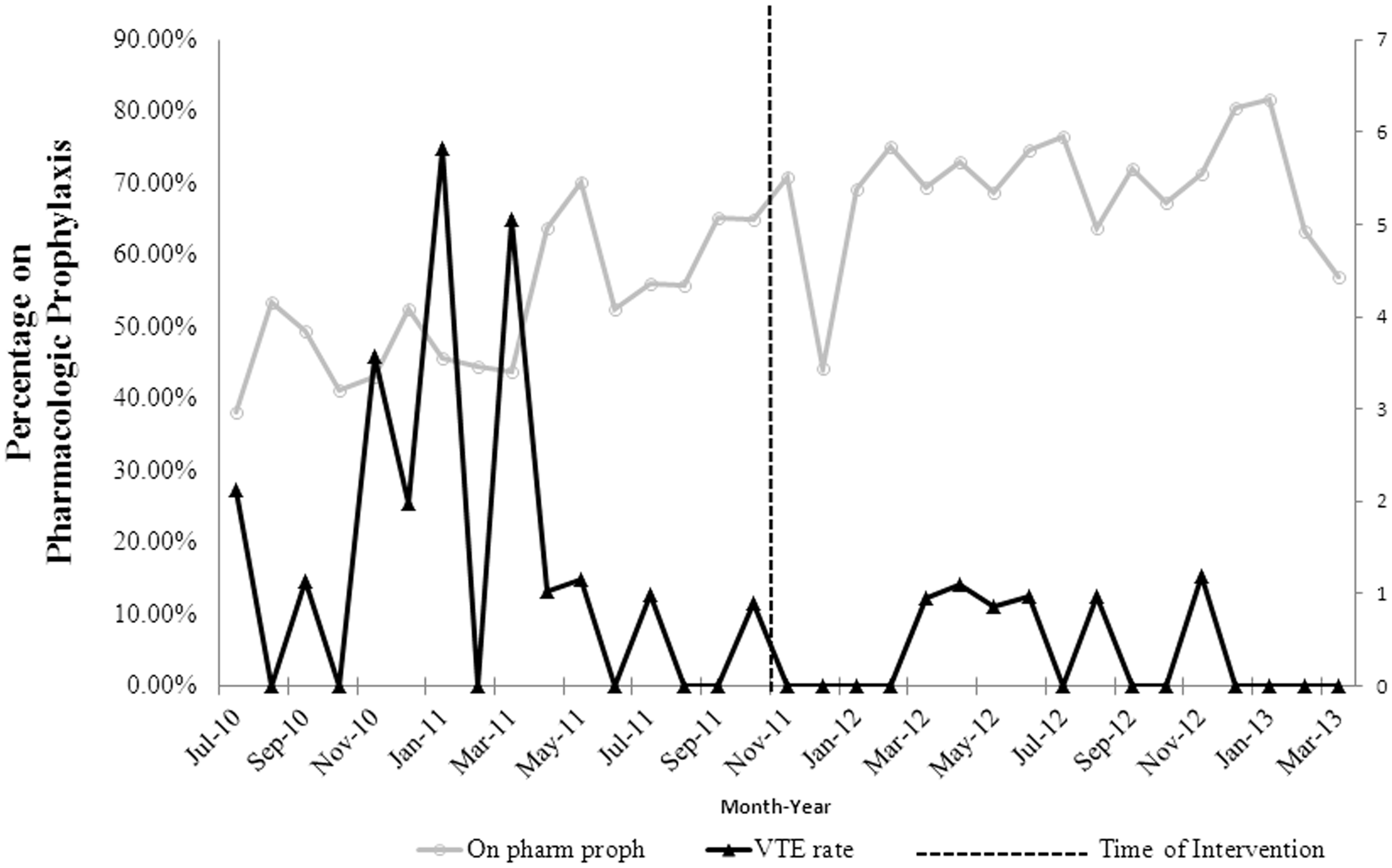
There were 1483 vascular patients in the pre-intervention group and 1652 patients in the post-intervention group. The rate of pharmacologic prophylaxis was 52.57% pre-intervention compared to 69.33% post-intervention (p < 0.001). The rate of pharmacologic or mechanical prophylaxis was 91.76% pre-intervention compared to 93.10% post-intervention (p = 0.54). The overall rate of VTE prior to the intervention was 1.49% compared to after intervention which was 0.38% (p = 0.033). The DVT rate prior to intervention was 1.09% vs 0.189% after intervention (p = 0.0214). The rate of pulmonary embolism trended towards a significant reduction with the intervention (0.681% vs 0.189%, p = 0.095). There were no statistically significant differences in patient groups based on gender, comorbidity category, severity of illness, or insurance type.
Conclusions
The overall rate of VTE was reduced by 75% after the initiation of a standard protocol for pharmacologic VTE prophylaxis. These findings justify an aggressive approach to VTE prophylaxis in vascular surgery patients.
Introduction
Venous thromboembolism (VTE) is a preventable complication associated with surgery and is a common cause of increased hospital length of stay, cost, and death.1–3 Incident VTE occurs in about 100 people per 100,000 every year in the USA, 24% of whom are attributable to hospitalization for surgery, with about one-third of cases manifesting as PE, and two-thirds of patients with DVT alone. VTE also causes 100,000 deaths per year, 4 and approximately 6% of DVT and 12% of PE cases result in the patient’s death within 1 month of diagnosis, while survivors often experience serious and costly long-term complications. 5 Patients who develop a post-operative VTE often are admitted to the intensive care unit and have a two-fold increase in their length of stay compared to those patients who do not have a VTE.4,6 It is estimated that VTE costs between $10,000 and $15,000 initially and re-hospitalization as a result of VTE and its sequelae can cost anywhere between $12,000 and $15,000. 6 Although the incidence of VTE following general and orthopedic procedures has been well described, there are limited data on the occurrence of VTE following vascular surgery. 7
Deep vein thrombosis (DVT) in the perioperative period can remain clinically silent. Located in proximal and distal deep veins, DVTs can lead to PE. The incidence of VTE varies greatly, depending on the type of operation, patient comorbidities, and functional status. In surgical subpopulations, the risk of DVT varies from 0.4% to 80%, depending on the site of deep veins involved, nature of underlying operation, and patient comorbidities.7,8
VTE has been targeted by the Centers for Medicare and Medicaid Services, the National Quality Forum, and others as an area for quality improvement. The key proposed procedure to accomplish this goal is appropriate VTE prophylaxis. As a result of this, the authors of this study sought to determine if an aggressive approach to VTE would reduce VTE rates on an inpatient vascular surgical service.
Methods
From July 2010 to March 2013, 3135 inpatients from the vascular surgical service were admitted to a dedicated vascular surgical unit at a single institution and studied in accordance with the University of Pennsylvania IRB. Beginning in November 2011, an aggressive approach towards intervention for VTE prophylaxis was instituted which included pharmacologic as well as mechanical prophylaxis. Meetings were held with attendings, nursing staff, advanced care practitioners, and trainees as the VTE prophylaxis strategy was rolled out. A discussion of VTE prophylaxis was incorporated into daily unit rounds such that patients were placed on pharmacologic and or mechanical therapy compression stockings (CS) and intermittent compression devices (ICD) unless there was a contraindication or this was obviated by the presence of a perceived prohibitive bleeding risk. The patients were divided into two groups, pre- and post-intervention. Pharmacologic prophylaxis in the form of subcutaneous (SQ) unfractionated heparin three times a day (TID) or Enoxaparin (QD) was instituted within 24 hours of admission pre-operatively and on post-operative day 1 unless deemed inappropriate by the attending surgeon. A VTE event was defined as a deep venous thrombosis affecting the lower extremity veins or pulmonary embolism. Venous duplex was typically ordered in the presence of unilateral leg swelling, and a chest CTA was performed in the presence of shortness of breath or chest pain symptoms. Patient demographics, VTE prophylaxis data, VTE event rate as well as procedural data were collected and analyzed. Patients in both cohorts were compared using the Agency for Healthcare Research and Quality (AHRQ) comorbidity categories, All Patient Refined Diagnosis Related Groups (APR-DRG) Severity of Illness, Insurance status and Principle procedure. Student’s t-tests were used to compare continuous variables and chi-square analysis used to compare categorical variables.
Results
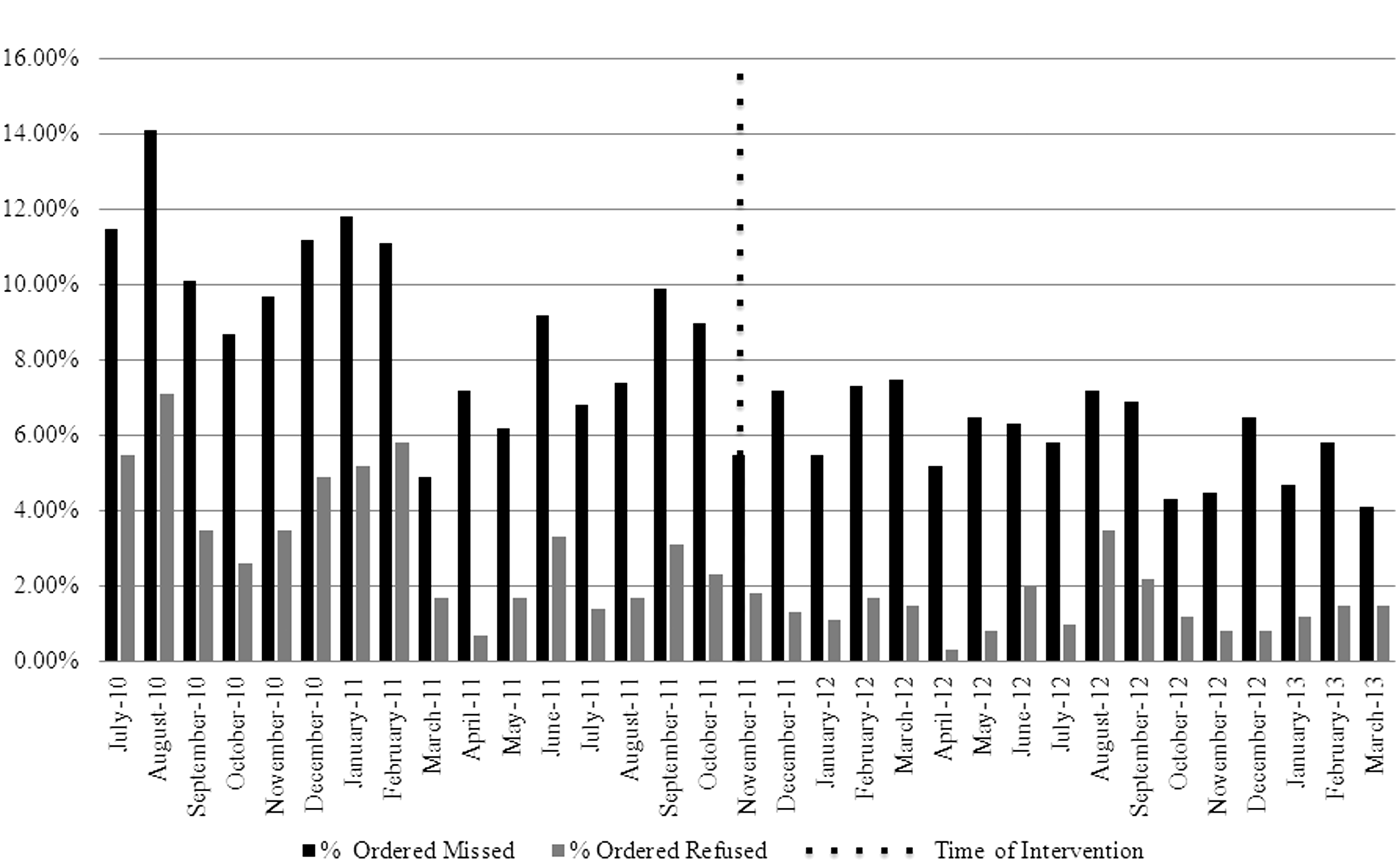
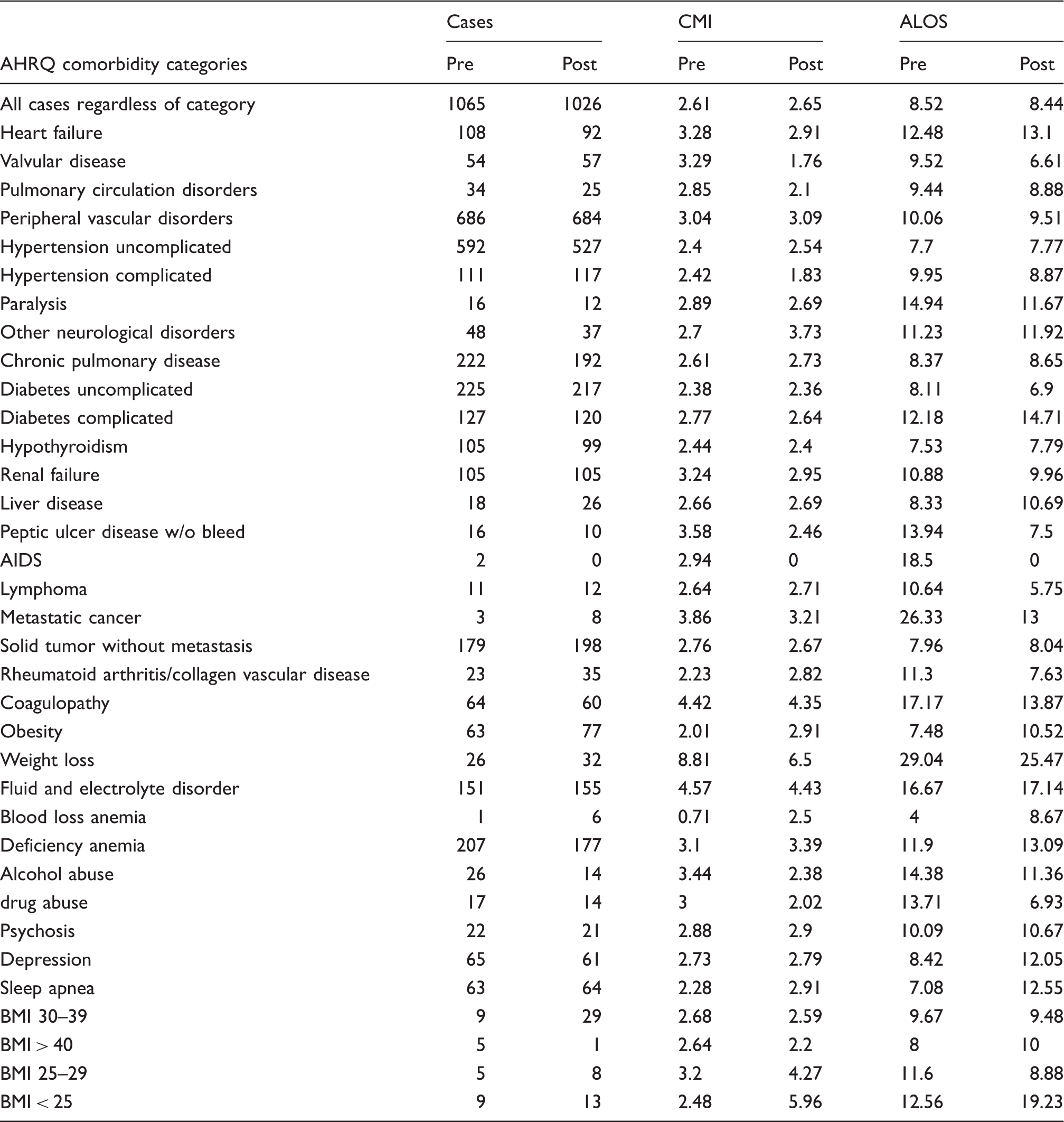
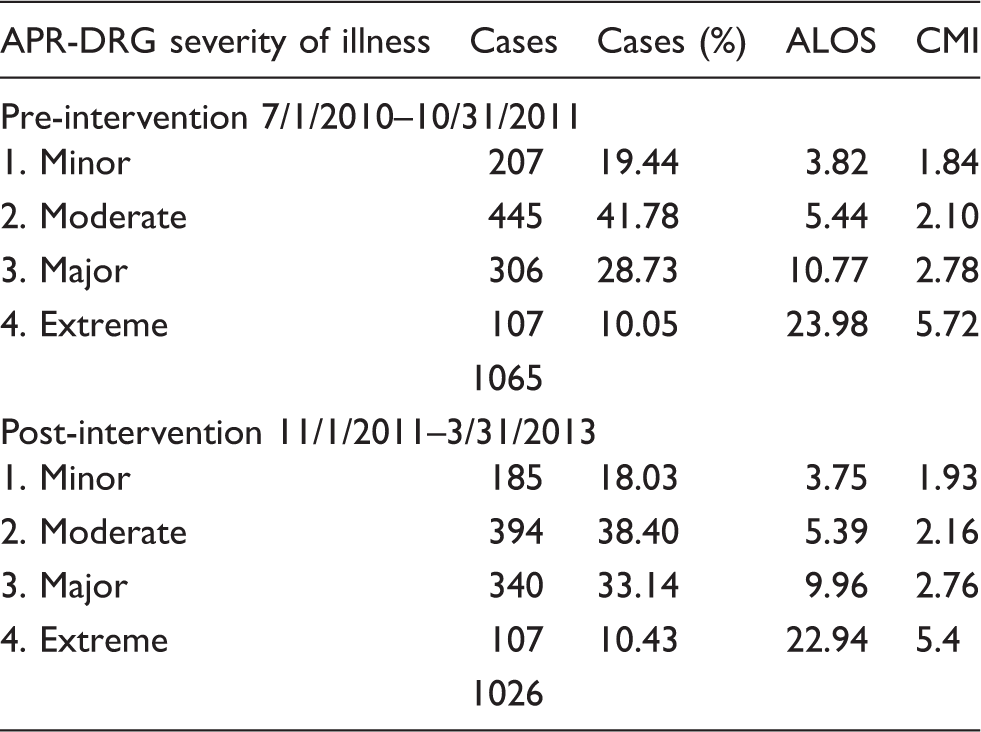
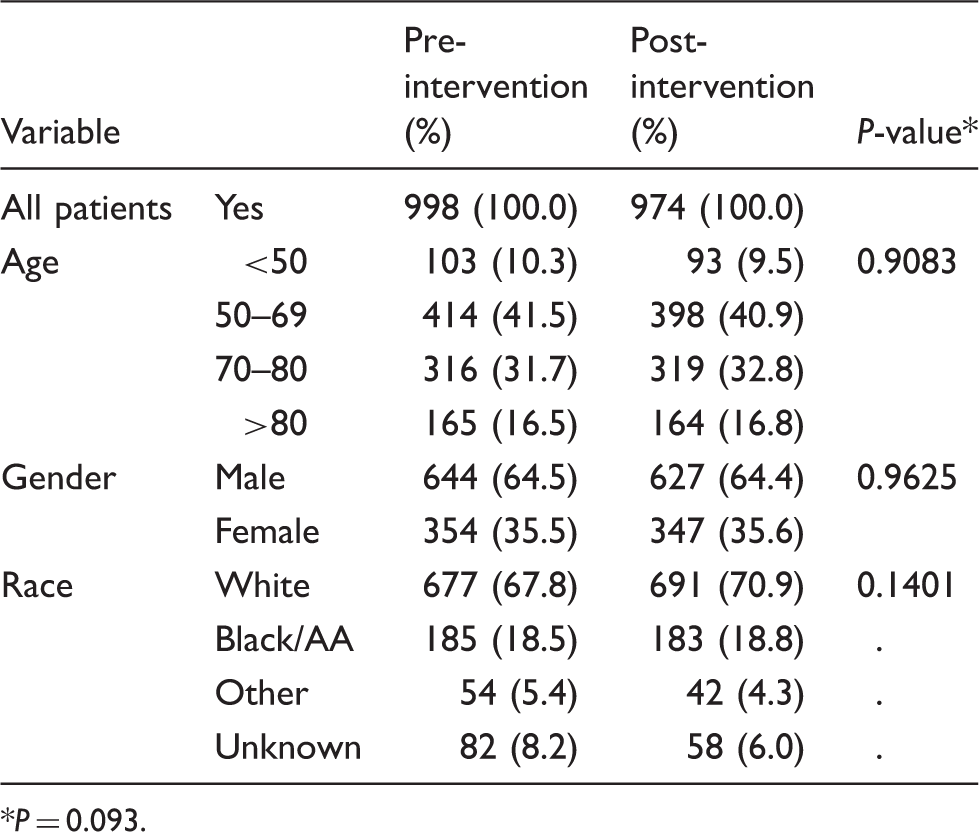
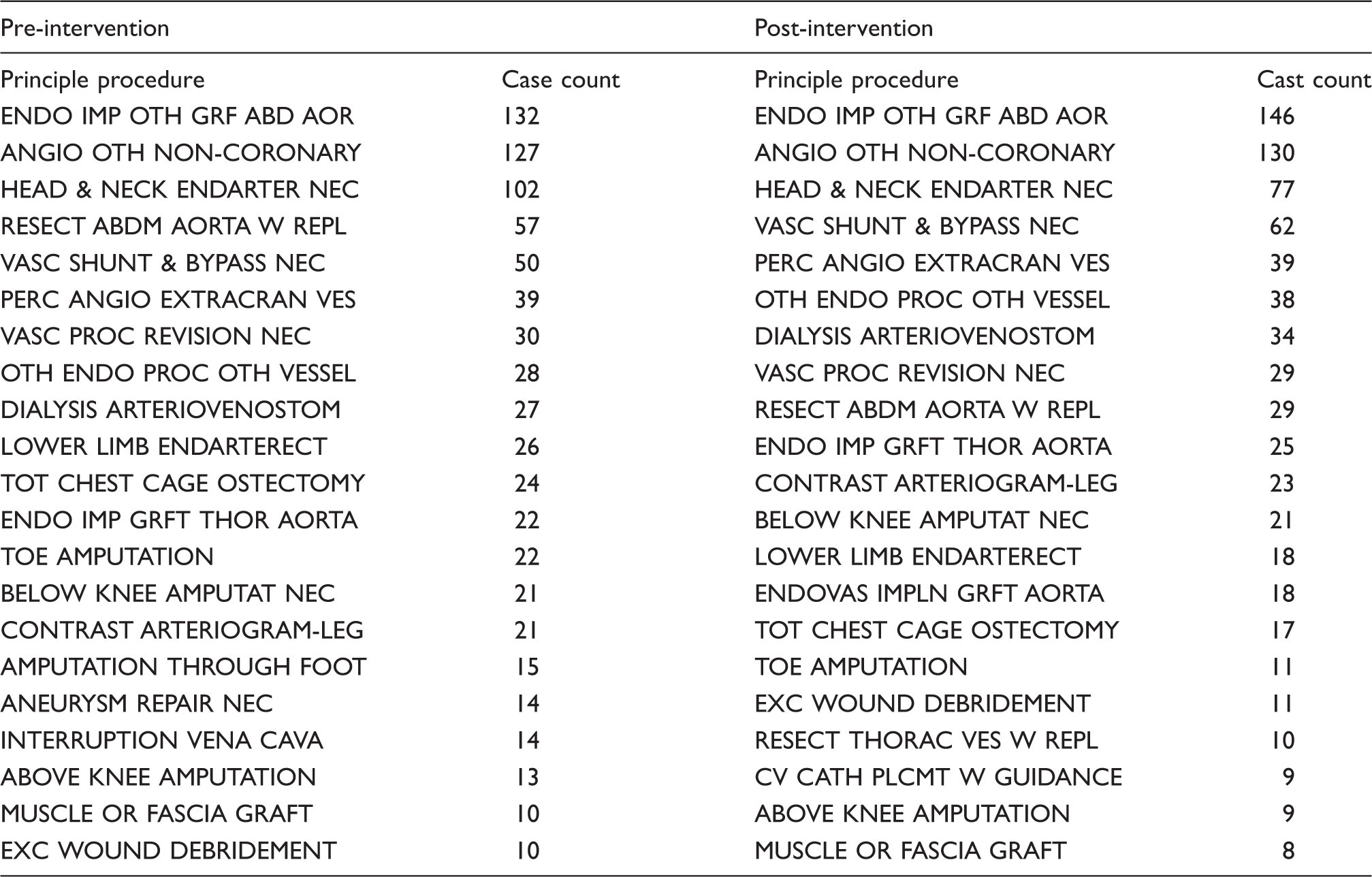
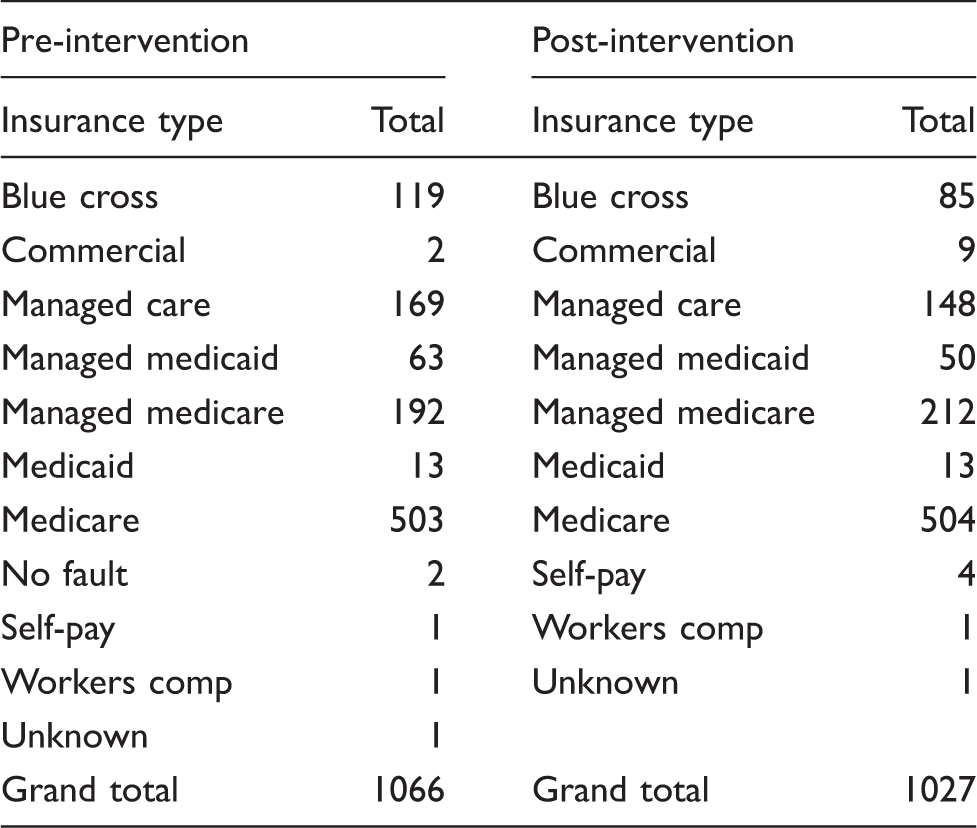
Of the 3135 patients analyzed, 1483 patients were in the pre-intervention group and 1652 patients were in the post-intervention group. All 23-h observation patients were excluded from administrative analysis; these procedures include angiograms and arteriovenous fistulas, for which the hospital stay following the procedure was less than one day. This left a total of 1065 pre- and 1026 post-intervention patients. The rate of pharmacologic prophylaxis was 52.57% pre-intervention compared to 69.33% post-intervention (p < 0.001), while the rate of pharmacologic or mechanical prophylaxis was 91.76% pre-intervention compared to 93.10% post-intervention (p = 0.54). (Figure 1) The overall incidence of VTE prior to the intervention was 1.49% compared to after intervention, which was 0.38% (p = 0.033), which is a 75.00% reduction in the rate of VTE. The DVT rate prior to intervention was 1.09% versus 0.189% after intervention (p = 0.0214). The rate of pulmonary embolism trended towards a significant reduction with the intervention (0.681% versus 0.189%, p = 0.095) (Figures 2 and 3). Furthermore, there was a decrease between the percentages of missed or refused doses in the post-intervention group, when compared to the pre-intervention group (p < 0.042) (Figure 4). AHRQ comorbidity indices as well as APR-DRG Severity of Illness scores were compared between both cohorts and there were no statistically significant difference, p > 0.135 and p > 0.093, respectively (Tables 1 and 2). There was no statistically significant difference between patient age or gender, p > 0.908 (Table 3). Principle procedures were compared between both cohorts and while there were little differences in types of procedures performed between the two time periods, the difference in open abdominal aortic aneurysm repair between the pre- and post-intervention cohorts was statistically significant, p = 0.007 (Table 4). There was no difference in insurance type between the two cohorts (Table 5).
Percent on pharmacologic prophylaxis. Rate of VTE. VTE rate percentage. Percentage of missed and refused doses by month pre and post intervention. AHRQ comorbidity categories. APR-DRG severity of illness pre- and post-intervention. Patient demographics. P = 0.093. Pre- and post-intervention principle procedures. Insurance type pre- and post-intervention patients.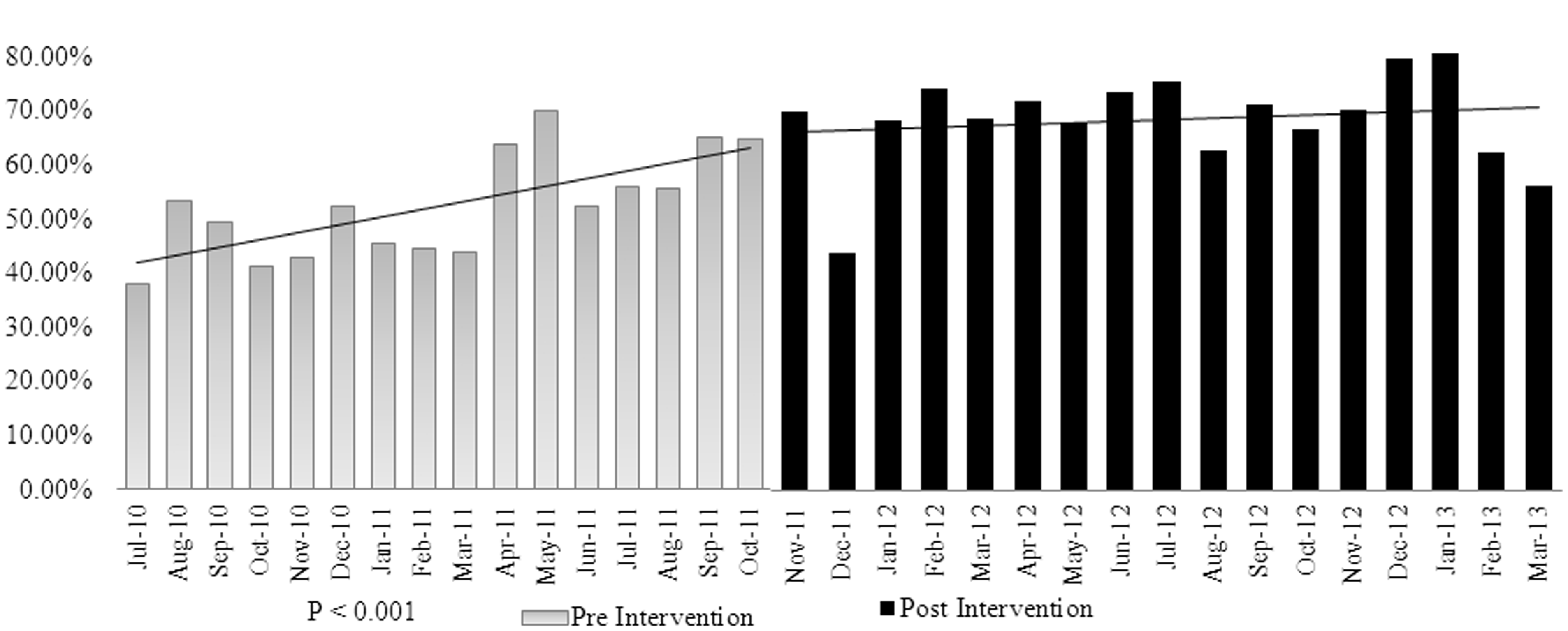
Discussion
VTE has been targeted by the Centers for Medicare and Medicaid Services, the National Quality Forum, and others as an area for quality improvement. PE is the most common preventable cause of hospital death and thus is an integral part of the effort to improve patient safety in hospitals. 9 The key proposed process to accomplish this goal is appropriate VTE prophylaxis.
Vascular surgery patients have several characteristics that put them at a high risk of developing VTE, such as older age, limited mobility after procedures involving the lower extremities are performed, long duration of surgery, and intraoperative dissection in proximity to the vein, atherosclerosis, and a higher rate of comorbidities.1,4–7,10,11 In a study by Huerta et al., the odds ratio of developing VTE after vascular surgery was 9.34 (95% confidence interval, 5.32–16.38) compared with no surgery, which was third only to musculoskeletal surgery and neurosurgery. 5 However, the study did not describe the types of vascular procedures performed. Rogers et al. studied different vascular procedures and assigned a high VTE risk score for several of these operations. 7 Rogers et al. found an overall VTE rate of 0.63% in 183,069 patients studied. Patients with VTE were more likely to have undergone emergency operation, have had a general anesthetic, and be an inpatient. Their operations were almost an hour longer than those without VTE and had a higher work RVU. Patients were placed into one of eight separate categories according to operation type, and those undergoing operations involving the respiratory system, hematologic and lymphatic systems, mediastinum, and diaphragm had the highest VTE rate which was 1.46%, followed by patients undergoing thoracoabdominal aneurysm repair, embolectomy/thrombectomy, venous reconstruction, and endovascular repair which had a VTE rate of 1.15%. Patients who underwent procedures for aneurysm repair, blood vessel repair, thromboendarterectomy, angioscopy, angioplasty and atherectomy, bypass and composite grafts, other artery, and vein procedures had a 0.73% VTE rate. 7
Despite this, the American College of Chest Physicians recommendations for thromboprophylaxis after vascular surgery are mainly based on effectiveness of chemical prophylaxis in general surgery patients.4,6 Eight randomized trials for VTE prophylaxis after vascular surgery were evaluated. The evidence for prophylaxis in high-risk vascular surgery patients was grade 1C, whereas that for low-risk vascular surgery patients was grade 2B, with all trials having a small number of patients. Although data on in-hospital VTE prophylaxis in patients undergoing vascular surgery are limited, the scarcity of quality data on VTE in patients undergoing vascular surgery highlights the importance of the findings from this data-set.
Identifying patients at high risk for the development of VTE is integral for instituting preventative measures targeted at high-risk groups. In other disease states, risk assessment scores have been developed to predict the post-operative complications, such as mortality from the procedure itself, pneumonia, respiratory failure, and cardiac complications.12–15 For example, the European system for cardiac risk assessment score (EuroSCORE) was developed to predict mortality in the cardiac surgery patient population.12,15 Additionally, the National Surgical Quality Improvement Program (NSQIP) database was developed to identify patients at risk for postoperative pneumonia and respiratory failure after manor non-cardiac operations.12–15
In our study, 3135 patients from the vascular surgical unit at our institution were examined, and our results highlight the importance of an aggressive prophylaxis regimen. The overall rate of VTE was reduced by 75% after the initiation of a standard prophylaxis regimen. Furthermore, the rate of pharmacologic intervention increased from 52.57% to 69.33% which was statistically significant, and 93.10% of all patients were receiving either mechanical or pharmacologic prophylaxis in the post-intervention cohort compared with 91.76% in the pre-intervention cohort. Prior to intervention, the DVT rate in our cohort was 1.49% compared to 0.189% after intervention which was determined to be statistically significant, while the rate of pulmonary embolism trended towards a significant reduction after intervention with a rate of 0.681% pre-intervention compared to 0.189% post-intervention. In addition, the rate of missed or refused doses also decreased in the post-intervention group when compared to the pre-intervention group. These results are particularly significant in light of the finding that there were no differences in return to the operating room for bleeding in the group that was post-intervention.
The results of this study highlight the importance of an aggressive prophylaxis regimen. Clinical treatment guidelines are based on up-to-date clinical evidence and consensus-based expert opinion, and they provide an important resource for healthcare professionals regarding optimum VTE prophylaxis practices. Despite the existence of such guidelines and their widespread dissemination, VTE prophylaxis is often underutilized and prescribed inappropriately in day-to-day clinical practice. Failing to provide appropriate prophylaxis has clinical implications, in terms of the higher rates of preventable VTE-related morbidity and mortality, and also the considerable impact on already over-stretched healthcare resources. This study was developed to drive improvement and, in so doing, narrow the gap between guideline recommendations and clinical practice. The development of hospital-wide VTE prevention strategies and the implementation as done so in this study increased the use of appropriate VTE prophylaxis and improved the clinical and economic outcomes of vascular surgery patients at risk of VTE.
Conclusion
In this study, the overall rate of VTE was reduced by 75% after the initiation of a standard protocol for pharmacologic VTE prophylaxis. These results suggest that an aggressive approach to VTE prophylaxis in vascular surgery patients can successfully decrease VTE events.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.