
Abstract
Objectives
To study the safety and efficacy of bare and covered stents in infrainguinal vein grafts after failure of PTA for treating graft stenoses.
Methods
An analysis of a prospective database of all patients who underwent stenting of infrainguinal vein bypass grafts at this institution between 1 January 2008 and 31 December 2012 was carried out. The main outcome considered was primary patency, which was reported at 1, 6 and 12 months.
Results
A total of 18 patients with a mean age of 73 years (range: 56 to 86) were included. The indications for stent placement were significant recoil (7, 39%), graft rupture (6, 33%), residual vein cusps (3, 17%) and aneurysmal degeneration (2, 11%). There was a high overall technical success rate of 94% (17/18) and arrest of haemorrhage was achieved in all cases of graft rupture. The primary patency at 1, 6 and 12 months was 89%, 71% and 59%, respectively.
Conclusion
The use of bare and covered stents in infrainguinal vein grafts appears safe and effective. They are an excellent bail-out option for the treatment of graft rupture and give acceptable short-term results.
Introduction
Occlusion of infrainguinal bypass grafts is a morbid and costly event and its prevention is worthwhile. 1 Whereas graft surveillance of prosthetic grafts has not proven to be beneficial, 2 surveillance is critical to the long-term outcomes of infrainguinal bypasses using vein grafts and has been shown to be cost-effective 1 and beneficial to the long-term patency of the grafts. 3
Graft stenoses are often solitary and focal 4 and hence respond fairly well to percutaneous transluminal angioplasty,5,6 though no consensus exists on its primary use.
The role of stents and stent-grafts in the percutaneous salvage of infrainguinal vein grafts is not yet defined and data are sparse. Jahnke et al. established its technical feasibility by using a monorail balloon-expandable stent device made of stainless steel. 7 Stent use has mainly been reported as a bail-out procedure when balloon angioplasty fails due to recoil, dissection or significant residual disease.8,9 There are also numerous reports of stent grafts used to treat vessel rupture complicating angioplasty of vein grafts used in coronary circulation, lower limbs and haemodialysis access.10–12
This study aims to evaluate the safety and efficacy of stents and stent grafts used as bail-out and adjuvant options in the salvage of failing infrainguinal vein grafts following balloon angioplasty. It also describes the indications necessitating their use.
Materials and methods
We reviewed a prospectively maintained database of the Queen Elizabeth Hospital Birmingham (Dendrite Clinical Systems, London, UK) over a 5-year period from 1 January 2008 to 31 December 2012. Patients were selected for percutaneous transluminal balloon angioplasty (PTA) on detection of significant infrainguinal vein graft stenosis (>70% stenosis: peak systolic velocity more than 300 cm/s and a velocity ratio across the stenosis of >3.5) by routine post-operative duplex surveillance of infrainguinal vein grafts at six weeks, three months, six months and every six months thereafter. Synthetic and composite part prosthetic and part venous grafts were excluded. The modality of treatment for these lesions was decided by the vascular surgical consultant based on morphologic characters of the lesion, patient co-morbidities, availability of conduit and patient preference. There was a preference for surgical revision for lesions which were diffuse and extending for more than one-third of the conduit length and those with suboptimal results or rapid restenosis after graft angioplasty provided other factors were favorable. All patients who had stents and stent-grafts inserted in infrainguinal vein bypass grafts were included. In the majority of these patients, these stents were not inserted primarily as a planned elective procedure, but only as bail-out options consequent to failure of angioplasty.
Definitions
Technical success was defined as achievement of final residual diameter stenosis of <30% on the procedural completion angiogram. Primary patency was defined as persistent patency from the time of the stent placement free from stenosis of >50% without any repeat interventions performed on or at the margins of the treated segments. Primary assisted patency was defined as patency after repeat endovascular interventions for morphologically significant restenosis plus all cases of primary patency.
Stenting
All procedures were performed under local anaesthesia in the angiographic suite by vascular interventional radiologists. Written informed consent was obtained prior to the endovascular intervention. Retrograde access through the contralateral groin into the grafts was employed in seven procedures and antegrade puncture in the rest. Antegrade puncture was carried out by puncturing the hood of the graft or the common femoral artery under ultrasound guidance and a 4-French vascular sheath was positioned to perform a preliminary angiographic study, using the non-ionic iso-osmolar contrast medium Visipaque® (Iodixanol) 320 (GE Healthcare, Little Chalfront UK) diluted up to 50%. Intravenous heparin (1000 to 3000 units) was routinely given after placement of the sheath. Patients who had graft stenting as day procedures were discharged the same day unless they had complications.
Follow up
After discharge patients were seen in the outpatient clinic at six weeks. In addition to a clinical examination, all patients had routine duplex examination as part of the graft surveillance regimen. They were subsequently followed up at three months, six months and every six months thereafter unless they required any further interventions in which case they would again be followed up as fresh cases. Surgical revision was preferred for grafts which thrombosed after stent implantation and hence secondary patency was not calculated.
End points
Patency rates over one year of follow up were analysed, and reported at one, six and twelve months. Factors considered in the analysis included the site of stenosis, previous intervention, indication for stent insertion, number and length of stents and stent dimensions.
Statistical analysis
Patency times were analysed using survival analysis methods and Kaplan-Meier survival curves. All analysis was performed using IBM SPSS 19 (IBM Corp. Armonk, NY).
Results
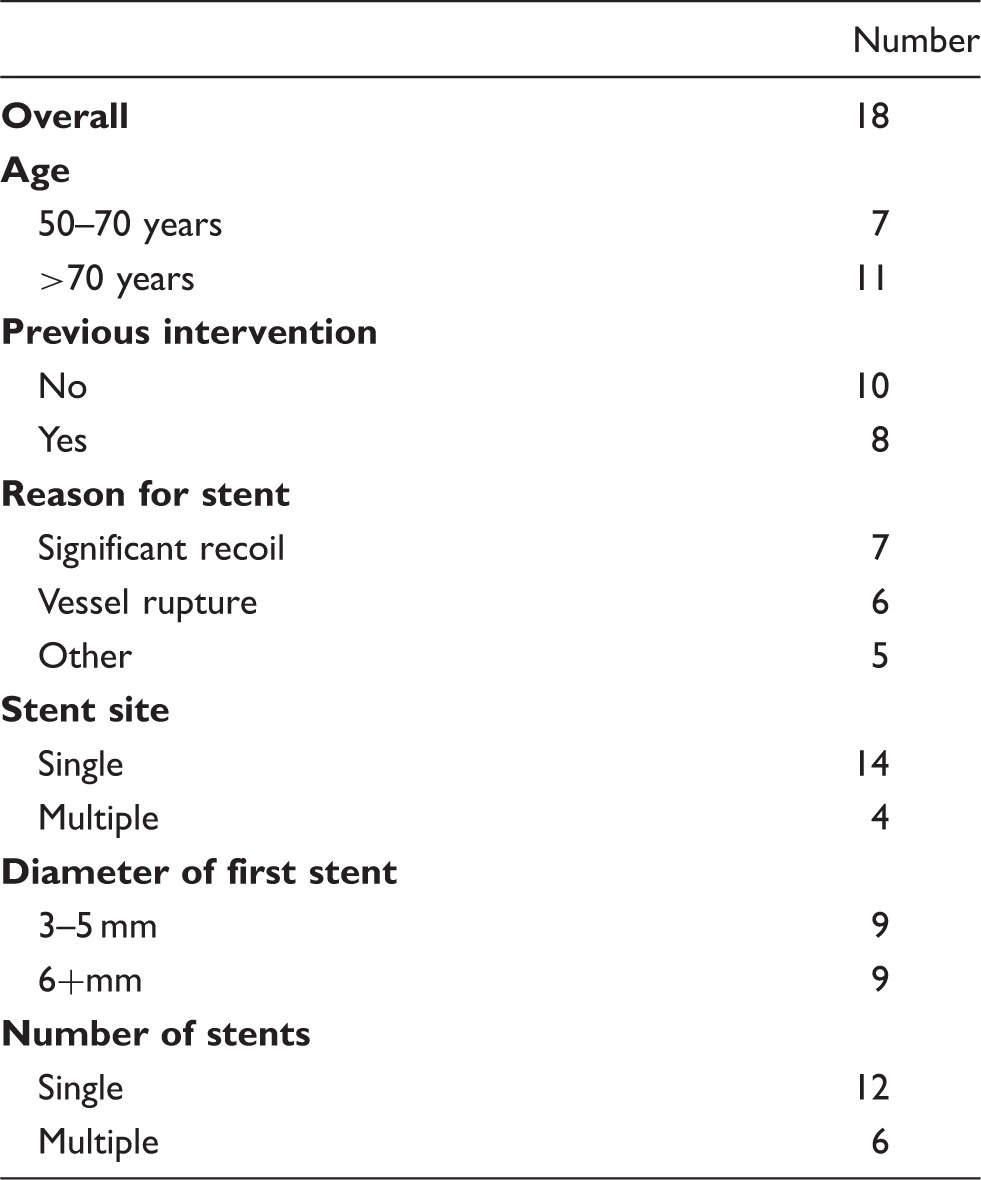
From 1 January 2008 to 31 December 2012, 18 patients (4 females, 14 males) had stents and covered stents put in infrainguinal vein bypass grafts. Their mean age at the time of intervention was 73 years with a range of 56 to 86 years. There were 5 patients (28%) with diabetes mellitus, 13 (72%) with hypertension and 2 (11%) with elevate renal parameters (serum creatinine >150 mmol/L). Infragenicular bypass grafts formed the majority with 15 (83%). 8 of the 18 (44%) grafts had already undergone one or more graft revisions (angioplasty and open). Further details are summarized in Table 2. None of the grafts had been previously stented.
Summary of bypass graft and stent features and outcomes.

AT: anterior tibial artery; AKP: above-knee popliteal artery, BKP: below-knee popliteal artery; PT: posterior tibial artery.
JOSTENT GraftMaster Coronary Stent Graft System is a product of Abbot Laboratories, Abbot Park, Illinois, USA.
LifeStent® is a product of CR Bard, Inc. Murray Hill, New Jersey, USA
Astron Pulsar is a product of Biotronik AG. Ackerstrasse, Switzerland.
Gore® Viabahn ® endoprosthesis is a product of WL Gore & Associates, Inc. Flagstaff, Arizona, USA.
Zilver® Vascular Stent and Zilver® PTX® Drug Eluting Peripheral Stent are products of Cook, Inc. Bloomington, IN, USA.
Patient and stent characteristics.
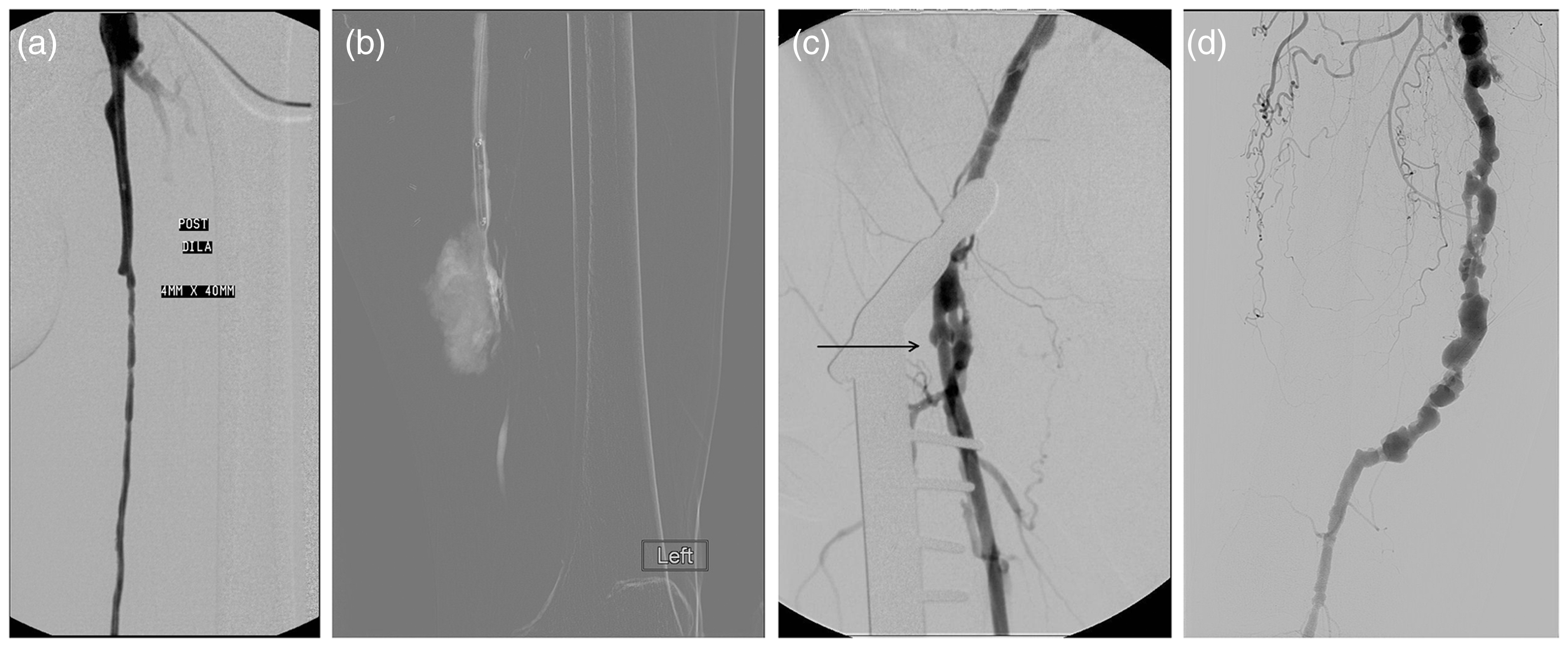
(a) Significant recoil after graft angioplasty, (b) graft rupture after angioplasty (c) Vein graft stenosis due to persistent valve leaflet (arrow) (d) aneurysmal degeneration of the vein graft.
Of the four the grafts which showed multi-segmental lesions, three were purely occlusive and one was associated with stenosis in one segment and aneurismal degeneration of multiple segments of the graft. All the three grafts with purely occlusive multisegmental lesions fared poorly with none remaining patent at 12 months and two patients requiring major amputations. Subset analysis was not attempted due to the small numbers in the groups.
Complications were encountered in two patients. The first was unexplained spasm of the distal vessels. This patient had presented with a thrombosed graft which after angioplasty had shown severe recoil in almost all segments of the graft and required a total of four stents. The outcome was probably a reflection of the severity of ischemia. Even a subsequent attempt at bypass failed and the patient needed a major amputation. The second complication was that of distal embolization which was successfully managed with aspiration.
The primary patency at 1, 6 and 12 months was 89%, 71% and 59% respectively (Figure 2). One patient died after the first follow-up. Limb salvage at the end of 1 year was 82% (14/17) in the remaining 17. Only one patient required repeat stenting due to recurrent stenosis during the period of follow-up, but as this was after the sixth month and the graft thrombosed before the end of the follow up, it did not change the primary assisted patency. Of the seven patients with occluded grafts, two were managed without further intervention during the 12-month period of follow-up. A further two had successful redo bypasses using fresh grafts and the remaining three had major amputations.
Kaplan–Meier estimate of patency rates.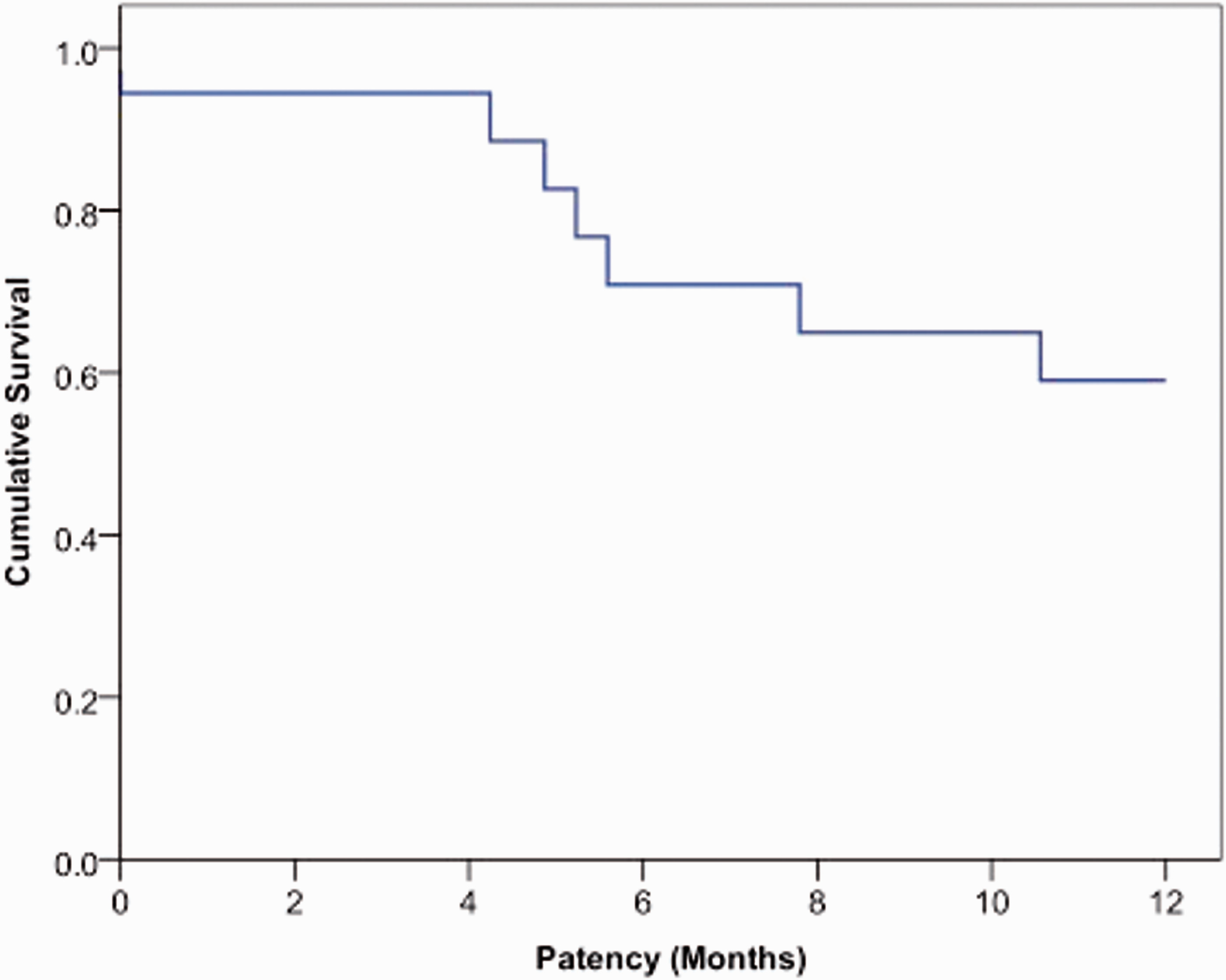
Discussion
There are very few published articles in the literature on stenting of infrainguinal vein grafts. Jahnke et al. 7 reported monorail stenting in eight infrainguinal grafts, four of which were vein grafts. There was successful device implantation in all eight grafts with no residual stenosis or procedure related complications. However, one graft occluded in two weeks, four grafts occluded before six months and only two patients had uninterrupted stent patency at 18 and 24 months. A review article on interventions in infrainguinal bypass grafts suggested that stenting of failing bypass grafts is justified in high risk patients or in whom surgery is doomed to fail due to extensive disease or complex lesion morphology. 9
Perhaps the largest series on the use of stents in infrainguinal bypasses was from Controneo et al. 13 where they described primary stent placement at distal anastomotic stenoses in 21 patients and reported cumulative primary, assisted primary and secondary patency rates of 71%, 81% and 86% respectively at one year. However, there are significant differences with this study, as they included four patients with synthetic grafts (leaving 17 infrainguinal vein grafts) and did not reserve stenting for failed PTA, but advocated its primary use on distal graft stenoses. Instinctively, those patients should have better outcomes.
In this study, we have described the use of stents after failure of PTA with four different situations where they were used for bail-out. Of these significant recoil and graft rupture reflect tough stenotic lesions in veins grafts. Residual vein cusps are a problem peculiar to the use of in-situ and non-reversed vein grafts. Importantly, the stents were successful in bailing out of trouble in all but one patient and achieved hemostasis in all the patients with graft rupture. Moreover, PTA alone would be inappropriate in aneurysmal degeneration of vein grafts with kinks and tortuosity of the grafts causing turbulent flow.
Major limitations of our study include the fact that it is a retrospective review and the small number of patients. On the latter point, this means that the estimates of outcome rates are subject to a wide margin of error and did not allow us to test for the effect of factors such as the number of stents, their diameter, the indication for stenting and the site of the stent, which might display an effect on the outcome. However, to the best of our knowledge, this is the largest series yet on stents in infrainguinal vein grafts. In light of this, we would advocate further research in this area, using a larger cohort to analyse factors affecting patency rates.
Conclusion
The use of bare and covered stents in infrainguinal vein grafts appears safe and effective. They have shown excellent results in the treatment of graft rupture and other complications of graft angioplasty and give acceptable short-term results in patients with few other percutaneous and surgical options.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.