
Abstract
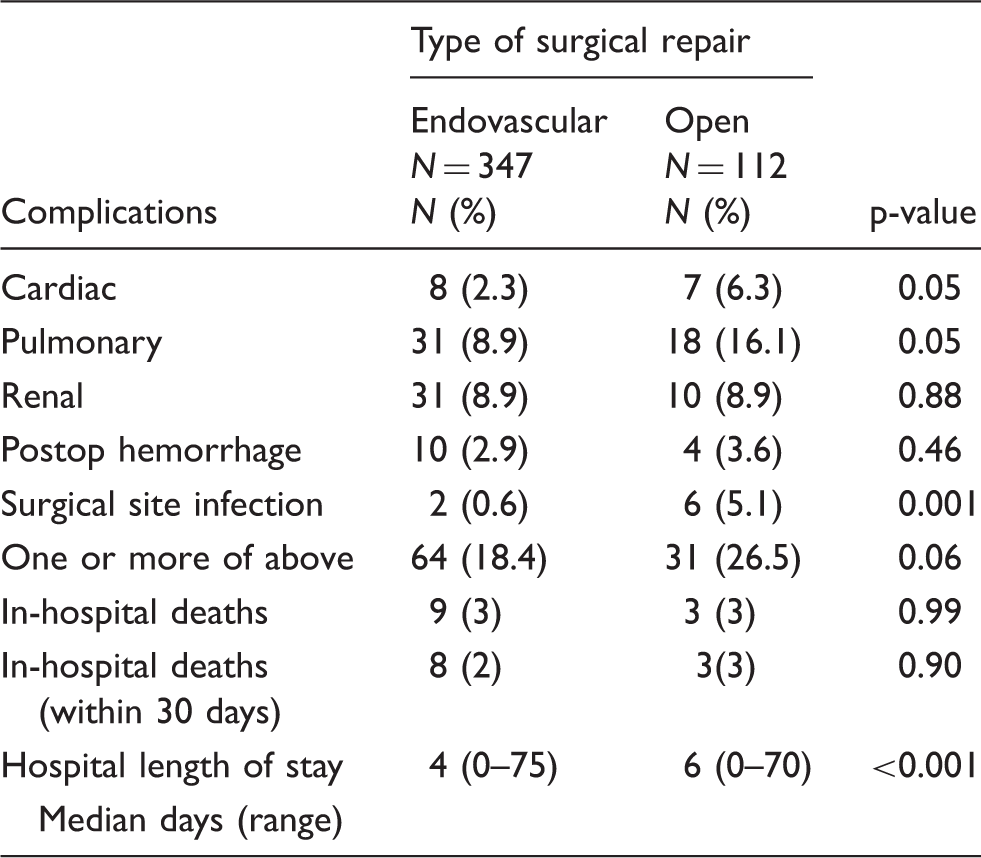
Splenic artery aneurysms are rare with an incidence of less than 0.8%. Evidence to support an endovascular management strategy over open surgical repair for SAA is limited. We used the Nationwide Inpatient Sample to compare open to endovascular SAA repair by assessing postoperative outcomes, length of hospital stay, and mortality. Multivariate logistic regression analysis was done to determine predictors of postoperative complications. There were 2316 admissions with a diagnosis code for SAA [347 (14.9%) endovascular repair and 112 (4.8%) open surgery]. There was a statistically significant lower rate of cardiac (2.3% vs 6.9%, P = 0.05) and pulmonary (8.9% vs 16.1%, P = 0.05) complications for the endovascular repair group. The risk of surgical site infection was also lower (0.6% vs 5.1%, P = 0.01) in the endovascular group. Median in-hospital LOS was greater for open repairs (6 vs. 4 days, P = 0.01). There were no statistically significant differences across procedures for renal complications (8.9%, P = 0.88) or in-hospital mortality (3%, P = 0.99). Regression analysis established procedure type to be independent predictor of postoperative complications. Endovascular repair of SAA is therefore associated with a lower complication rate and less resource utilization but no difference in mortality peri-operatively. This may justify an endovascular first treatment strategy in the management of SAA.
Introduction
Splenic artery aneurysms (SAA) are the most common visceral artery aneurysms, yet they are relatively rare with an overall estimated incidence of 0.8%.1,2 The potential for fatal complications associated with aneurysm rupture may necessitate repair when discovered. In fact, the mortality associated with splenic artery aneurysm rupture has been reported to be as high as 30%, with an even higher rate reported in pregnant populations where the maternal mortality approaches 75% and the fetal mortality 95%.3–5 Repair is therefore usually considered for symptomatic aneurysms, aneurysms greater than 2 cm in size, those uncovered in patients undergoing liver transplantation, or any SAA found in women of child-bearing age.6–10
Traditionally, open surgical techniques have been used to treat or exclude SAAs. More recently, endovascular treatment has been widely accepted as an alternative for the management of these aneurysms.11–13 However, due to the relatively low incidence of this disease, the available literature is limited to case reports and small series and there are few comparative studies. In a recently published meta-analyses of the literature by Hogendoorn et al., endovascular repair of SAA was found to have better short-term results and a lower perioperative mortality when compared to open repair although open SAA repair was associated with fewer re-interventions and better long-term outcomes. 14 The purpose of our review is to compare open to endovascular SAA repair using a large nationwide database to assess postoperative outcomes, length of hospital stay, and mortality to better clarify treatment strategies.
Materials and methods
Data were collected from the Nationwide Inpatient Sample (NIS) database from the Health Care Cost and Utilization Project from 2008 to 2011. The NIS database is sponsored by the Agency for Healthcare Research and Quality, and represents a random 20% sample of all admissions to hospitals in states that require reporting. This currently represents over 1000 hospitals in 46 states, making NIS the largest all-payer administrative database in the USA. This database contains information regarding patient demographics, severity and comorbidity measures, primary and secondary diagnosis and procedures, length of stay, and discharge status.
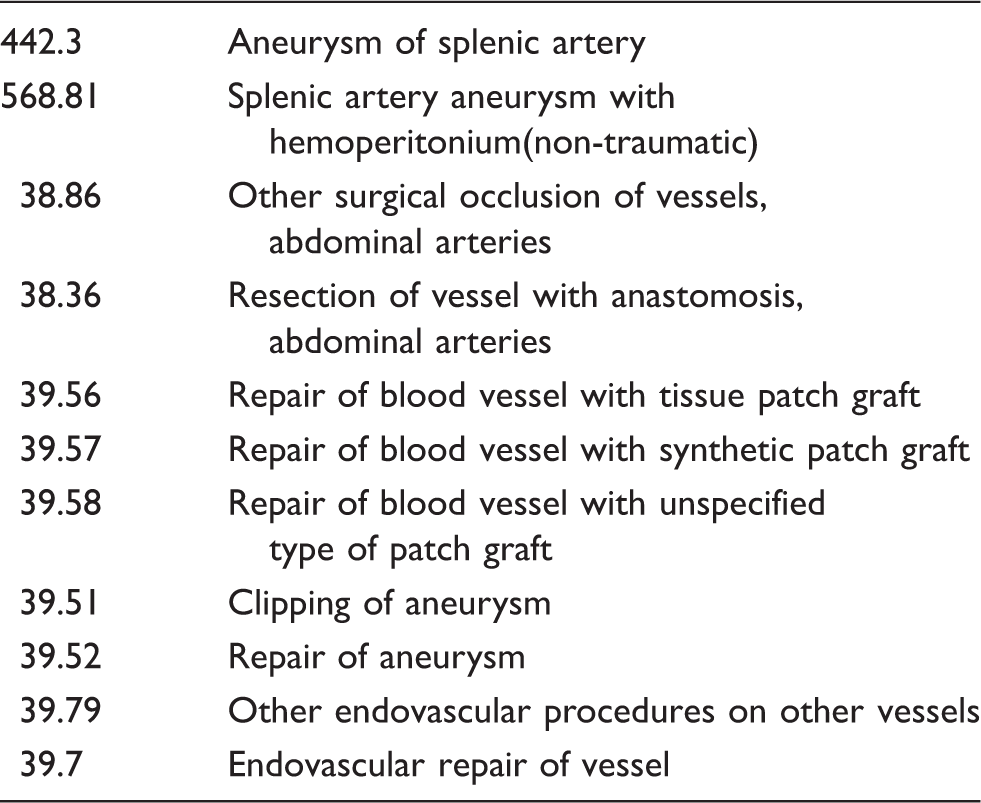
ICD9 codes for SAA and procedure type (open vs endovascular).
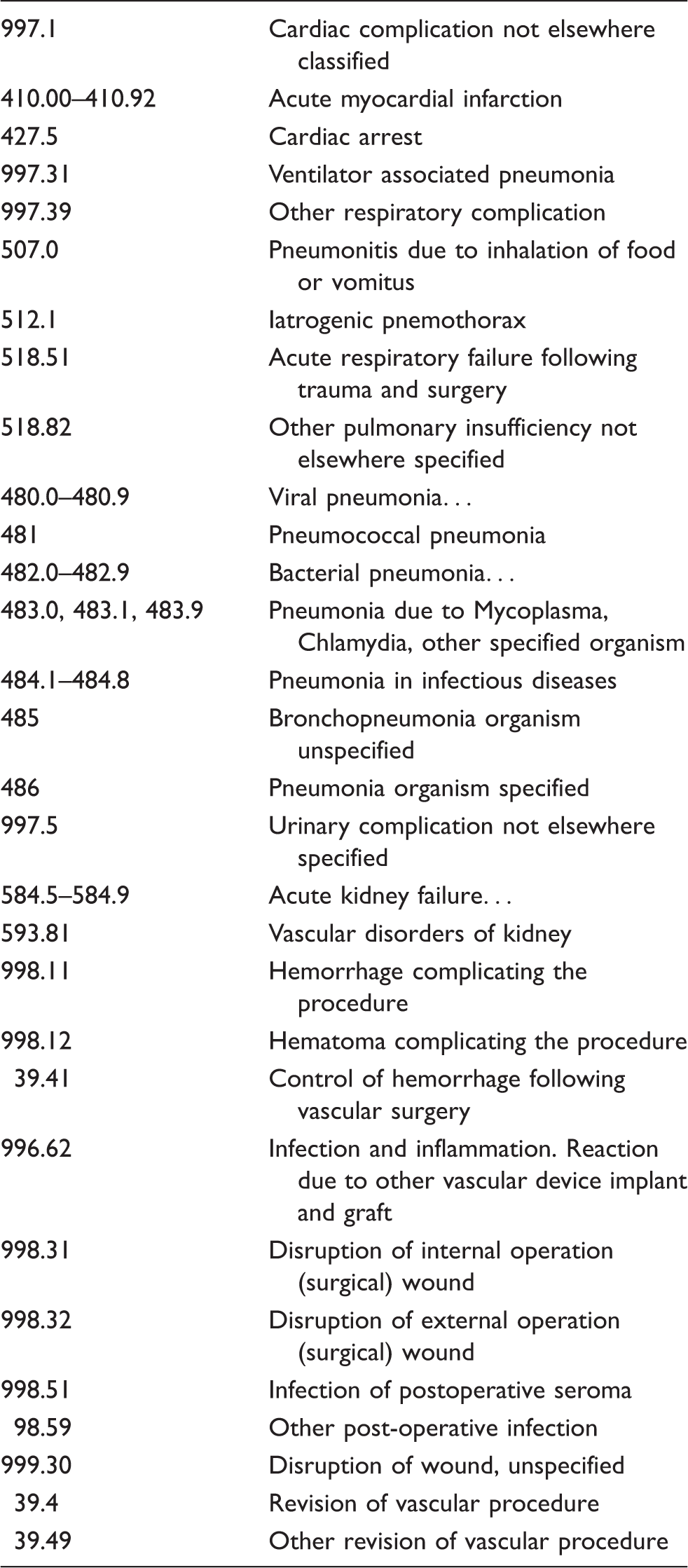
ICD9 codes for complications and other outcome measures.
Demographics, comorbidities and outcomes were compared across patients undergoing open and endovascular repairs. A Chi-square test was used to analyze categorical variables, while continuous variables were analyzed using the Student t-test or Mann–Whitney U statistic. Multivariate logistic regression analysis based on age, comorbidities, and procedure type (open vs endovascular) was done to predict the presence of postoperative complications. Statistical significance was considered at a P-value of less than 0.05. All statistical analyses were performed using SPSS software (SPSS, Chicago, IL, USA).
Results
There were 2316 admissions during the study period with a diagnosis code present for SAA. Among these, 347 (14.9%) patients underwent endovascular repair and 112 (4.8%) patients had open repair. Therefore, the majority of patients admitted with a diagnosis of SAA were discharged without intervention. Of the 459 patients who underwent repair, 33 (7.2%) had a diagnosis of hemoperitoneum, with 20 of these undergoing endovascular repairs and 13 open surgery. There were three mortalities in this subgroup presenting with rupture, 1 (5%) in the endovascular group and 2 (15%) in the open group, which was a non-significant difference (P = 0.31).
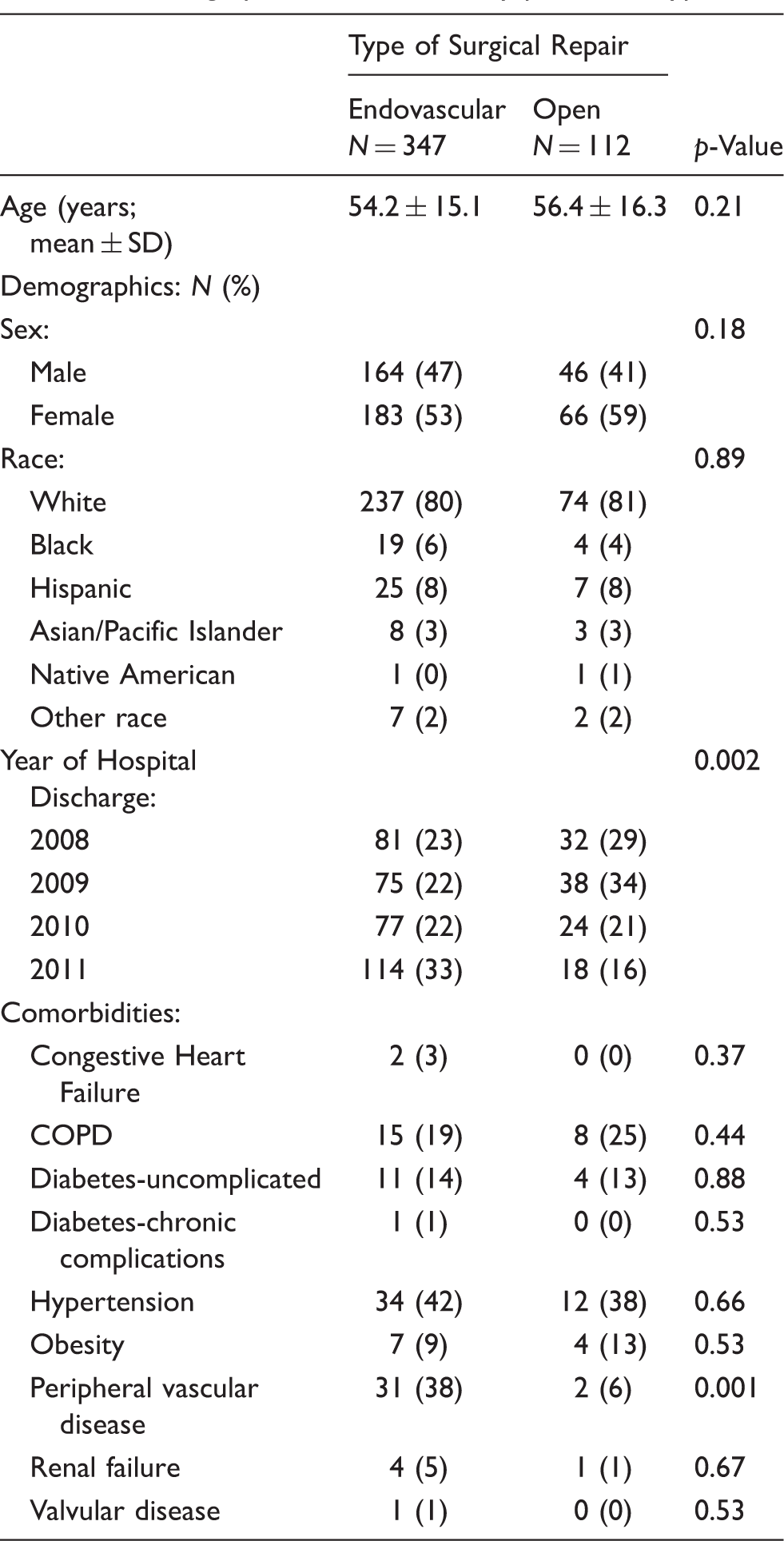
Demographic characteristics by procedure type.
Outcomes measures by procedure type.
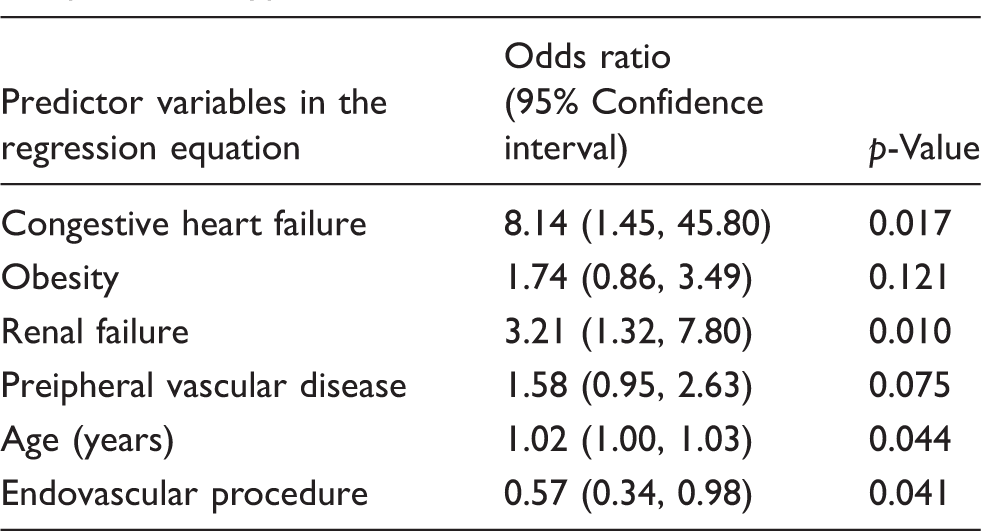
Multiple logistic regression analysis predicting presence of any complication based on age, co-morbidities, and procedure type.
Discussion
SAA are the most common of all visceral artery aneurysms, but are still rare and infrequently encountered in clinical practice. 15 More often, they are asymptomatic and found incidentally on abdominal imaging. SAA may present as a signet ring calcification in the LUQ on plain abdominal radiographs although most are found on abdominal CT.16,17 These aneurysms can be associated with renal artery aneurysms and other visceral artery aneurysms, findings which have been reported 14% and 3% of the time, respectively. 2 SAA tend to be more common in women, with a 4:1 female to male ratio5,18 although we found a near equal male to female distribution. 5
The most common risk factors for SAA are portal hypertension and multiple pregnancies. 8 Multiple pregnancies are believed to be a strong risk factor for SAA because of the hormonal changes and hepatic congestion that occurs during pregnancy. 17 Other risk factors include splenomegaly, medial fibrodysplasia, atherosclerosis, autoimmune diseases, collagen vascular diseases, α-1 antitrypsin deficiency, and pancreatitis.10,2,18,20 The majority of SAA are small and saccular and located in the middle or distal splenic artery. 2 If the aneurysm were to rupture, as occurs in approximately 3–10% of the cases, presentation tends to be abdominal pain with hypovolemic shock. 21 In our study, 7.2% of the patients presented with hemoperitoneum and greater than 60% of these patients were treated endovascularly, making endovascular SAA repair a preferred modality even for emergent situations. Data concerning ruptured SAA and type of repair could not be built into multivariate analysis because the number of patients with ruptured SAA was too small to allow for any meaningful statistical analysis.
A topic of debate in recent years has been on the approach taken to treat these SAA, or if they should be treated all. Studies have shown that SAA less than 2 cm in size that were left untreated had very few complications with a survival rate of 95%. 19 Hence, treatment for SAA is generally reserved for larger or symptomatic aneurysms, or for those found in liver transplant patients or women of child-bearing age. As demonstrated by our study, the move in recent years has been towards an endovascular approach for SAA treatment. For the endovascular approach, these aneurysms may either be embolized or stented. 17 Embolization tends to be the preferred modality as stent grafts may be harder to insert and deploy within tortuous arteries. 17 In this study, procedure type was an independent predictor of postoperative complications. In fact, we found endovascularly treated SAA’s to have a nearly 50% lower risk of pulmonary and cardiac complications, a lower risk of having more than one complication per patient, and a shorter hospital stay than SAA treated via open surgical repair. Also, we found a five-fold higher risk of surgical site infection when treating via open repair as opposed to an endovascular approach. Another factor favoring endovascular treatment is that this can be accomplished using only local anesthesia and sedation as an outpatient procedure, while open surgical repair necessitates general anesthesia and hospitalization.
As with other endovascular procedures, durability has been questioned, and data regarding long-term outcomes for endovascular approaches are limited. Our study focused on short-term outcomes and therefore does not help establish the durability of endovascular SAA repair. However, a recent report established 100% technical success rate for patients undergoing endovascular SAA repair with no aneurysm-related deaths on a median follow-up period of 45 months. 22 In another publication with a mean follow-up of 15 months, aneurysm exclusion was seen on imaging studies in 97% of cases with no reports of sac growth. 13 This study represents a retrospective analysis of the NIS database and is limited by all the inherent problems associated with the use of large databases. Commonly recognized in any administrative database, the data collection is subject to entry errors and selection and reporting bias. Additionally, we did not include any complications beyond the initial hospitalization period as these data are not included in NIS, and this might underestimate the morbidity associated with SAA repair. An additional limitation of this database is that is does not include any detail regarding the etiology or anatomy of the SAA undergoing treatment, nor are any technical aspects of repair provided. Despite these limitations, we believe this study adds support to the growing body of literature favoring endovascular treatment as the preferred approach in the management of SAA.
Conclusions
SAA are a rare but potentially fatal condition. While observation may be a reasonable approach, select patients may require open or endovascular repair. In this study, endovascular SAA repair was associated with a lower peri-operative complication rate and less resource utilization when compared to an open approach to SAA repair. We would favor endovascular treatment for patient with SAA requiring repair.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.