
Abstract
Background
Studies reporting the influence of preoperative abdominal aortic aneurysm diameter on late survival following abdominal aortic aneurysm repair have not been consistent.
Methods
Embase, Medline and the Cochrane electronic databases were searched to identify articles reporting the influence of abdominal aortic aneurysm diameter on late survival following open aneurysm repair and endovascular aneurysm repair published up to April 2015. Data were extracted from multivariate analysis; estimated risks were expressed as hazard ratio.
Results
A total of 2167 titles/abstracts were retrieved, of which 76 studies were fully assessed; 19 studies reporting on 22,104 patients were included. Preoperative larger abdominal aortic aneurysm size was associated with a worse survival compared to smaller aneurysms with a pooled hazard ratio of 1.14 (95% CI: 1.09–1.18), per 1 cm increase in abdominal aortic aneurysm diameter. Subgroup analysis of the different types of repair was performed and the hazard ratio (95% CI), for open aneurysm repair and endovascular aneurysm repair were 1.08 (1.03–1.12) and 1.20 (1.15–1.25), respectively, per 1 cm increase. There was a significant difference between the groups p < 0.02.
Conclusions
This meta-analysis suggests that preoperative large abdominal aortic aneurysm independently influences overall late survival following abdominal aortic aneurysm repair, and this association was greater in abdominal aortic aneurysm repaired with endovascular aneurysm repair.
Keywords
Introduction
Abdominal aortic aneurysm (AAA) rupture is associated with high surgical mortality worldwide, 1 yet AAA can be effectively managed by either open aneurysm repair (OAR) or endovascular aneurysm repair (EVAR) in an elective setting with a 10-fold decrease in perioperative mortality. Regardless of the repair method chosen, results from four randomized trials and two large cohort studies indicate that survival is similar between EVAR and OAR.2,3
Previous research has identified several independent prognostic variables associated with lower survival following AAA repair with varying size effects. These include demographic such as age, gender and clinical comorbidities including cardiac, renal or pulmonary impairment. 4 Furthermore, population studies have also shown that an increase in infra-renal abdominal aortic size above the normal aortic diameter or the presence of an AAA (defined as greater than or equal to 3 cm) are independent predictors of increased cardiovascular and overall late mortality.5,6
Koskas and Kfeifer 7 were the first to report that the diameter of the AAA negatively predicted late survival following OAR in a multicenter prospective trial consisting of 794 patients. The hazard ratio (HR), 95% confidence interval (CI) was 1.1 (95% CI: 1.04–1.08) for each 1 cm increase in AAA diameter. 7 Following the emerging use of EVAR in the early 2000s, endovascular registries from Europe (EUROSTAR) and the United States (Lifeline registry) both reported that larger AAA were independently associated with worse late survival.8,9 However, other studies have observed no difference in late survival between small and large AAA diameter.10,11
Since late survival following AAA repair is determined by preoperative factors such as AAA diameter, quantifying the individual risk is necessary in clinical decision-making. This systematic review and meta-analysis aimed to report the influence of preoperative AAA diameter on late survival of patients undergoing elective AAA repair.
Methods
The systematic review was conducted according to the preferred reporting items for systematic reviews and meta-analysis (PRISMA). 12 Individual patient consent was not possible, as this review will analyze published literature only. The Health and Disability Ethics committee has approved this project. This topic was defined in the PICOT 13 format as: the population are patients undergoing elective AAA repair (via either OAR or EVAR); intervention and comparison: preoperative AAA diameter, Outcome: all cause mortality and time: greater than or equal to one year.
Search strategy
EMBASE, Medline and the Cochrane Library Database were searched via the electronic OVID SP database. With the assistance of a clinical librarian, “exploded” medical subject headings (MeSH) terms for MEDLINE and Cochrane, and EMTREE terms for EMBASE were used to broaden the key word search: “abdominal aortic aneurysm,” “size,” “blood vessel diameter,” “long term survival” and “survival rate” along with their synonyms. Two independent researchers (MK and JR) conducted the search and when disagreement arose the reviewers met to resolve any issues.
There was no date restriction and no limitations on publication language or study type applied to the search. The last search was completed in April/May 2015. An additional manual search of articles was conducted using references from relevant articles and review papers. The journals of Annals of Vascular Surgery, European Journal of Endovascular and Vascular Surgery, Journal of Endovascular Therapy, Journal of Vascular Surgery and Vascular were searched for any relevant articles published “online first.” Abstracts of conference proceedings were searched for full text publication. Eligible titles or abstracts where imported into Endnote X7 (Thomson Reuters) library and full text articles were obtained.
Study selection
Inclusion and exclusion selection criteria
Two independent reviewers adhered to the following inclusion criteria: any studies with greater than a 100 patients, reporting survival data and information about preoperative AAA diameter following elective AAA repair (OAR or EVAR) with at least one year follow-up with the primary endpoint of outcome being all-cause mortality. There were no restrictions to operative repair methods and complex repairs (suprarenal clamping/visceral debranching or fenestrations). The exclusion criteria were studies that were solely limited to small AAA (<5 cm), rupture AAA, first generation/early custom-made stent grafts, high-risk patients and octogenarians.
Study selection and data extraction
Two researchers independently performed the data extraction. Studies that met the inclusion criteria were entered into a Microsoft Excel spreadsheet. When studies from large registries, or known databases were included, only the most recent study that contained the largest number of patients or the study that kept AAA diameter as a continuous variable was used in the analysis. Study authors were contacted when clarification was required.
The quality of the observational studies (cohort) was assessed using the Newcastle-Ottawa Scale (NOS). 14 This tool employs a 9-point system that assesses three domains: patient selection, comparability of the study groups and the ascertainment of study outcome. Studies with a score of 9 indicate a lower risk of bias whereas scores of 7–8 indicate medium risk of bias and a score of ≤6 indicates a higher chance of bias.
Statistical analysis
Reported baseline risk factors were extracted from baseline tables, group means and standard deviations (SD) were weighted and combined for descriptive purposes. A meta-analysis of time-to-event data was undertaken. Reported HR (statistically significant and non-significant) from multivariate Cox proportional models were extracted from individual studies. Pooled estimates together with 95% CI were calculated using a random effects model, chosen due to expected heterogeneity among the studies. Heterogeneity was expressed with the I2 statistic with greater than 25%, 50% and 75% defined as low, moderate and high degrees of heterogeneity. Statistical significance was set at a p-value 0.05. Sub group analyses were performed according to a priori groupings related to type of repair (EVAR vs OAR). The meta-analysis was performed using Review Manager (RevMan) [Computer program] Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012. Meta-regression was performed in R using the package metafor, with heterogeneity estimated using the DerSimonian–Laird method with inverse variance weights.15,16
Results
The literature search flow chart results are summarized in Figure 1. Of 2167 titles, 72 were thought to be relevant after screening titles and abstracts. Following duplication removal, 66 articles were assessed of which 10 met the inclusion criteria.17–26 The hand searching identified seven additional studies7,11,27–30 and searching vascular journals for ahead of print/“Online first” articles identified two additional studies.31,32 Nineteen articles were included in the systematic review of which three did not include sufficient data to allow inclusion into the meta-analysis. One study provided descriptive results only
27
and two studies included univariate (unadjusted) risk ratios.25,26
PRISMA Diagram showing flowchart of study selection.
Study characteristics of included studies.
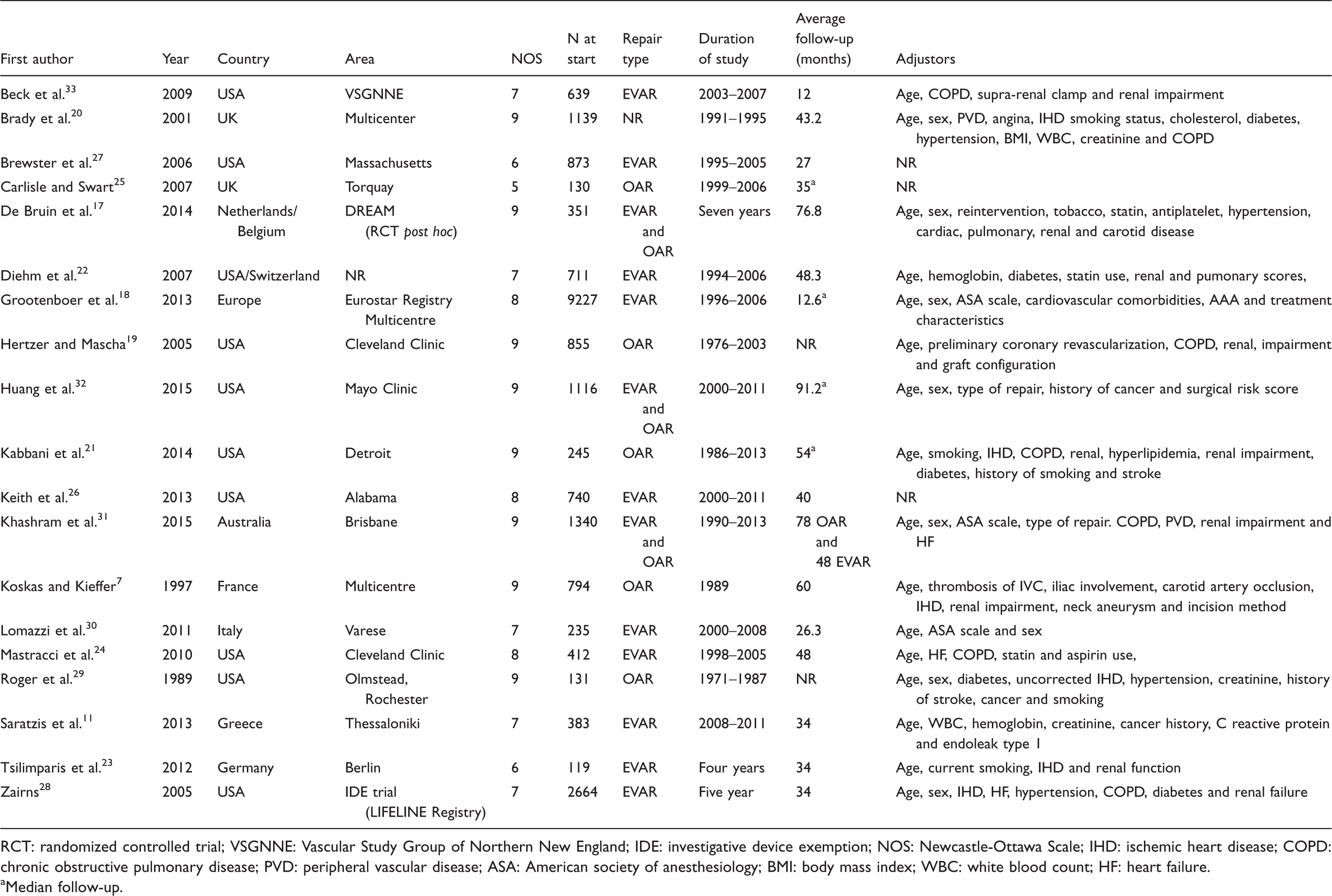
RCT: randomized controlled trial; VSGNNE: Vascular Study Group of Northern New England; IDE: investigative device exemption; NOS: Newcastle-Ottawa Scale; IHD: ischemic heart disease; COPD: chronic obstructive pulmonary disease; PVD: peripheral vascular disease; ASA: American society of anesthesiology; BMI: body mass index; WBC: white blood count; HF: heart failure.
Median follow-up.
Patient and AAA baseline characteristics.
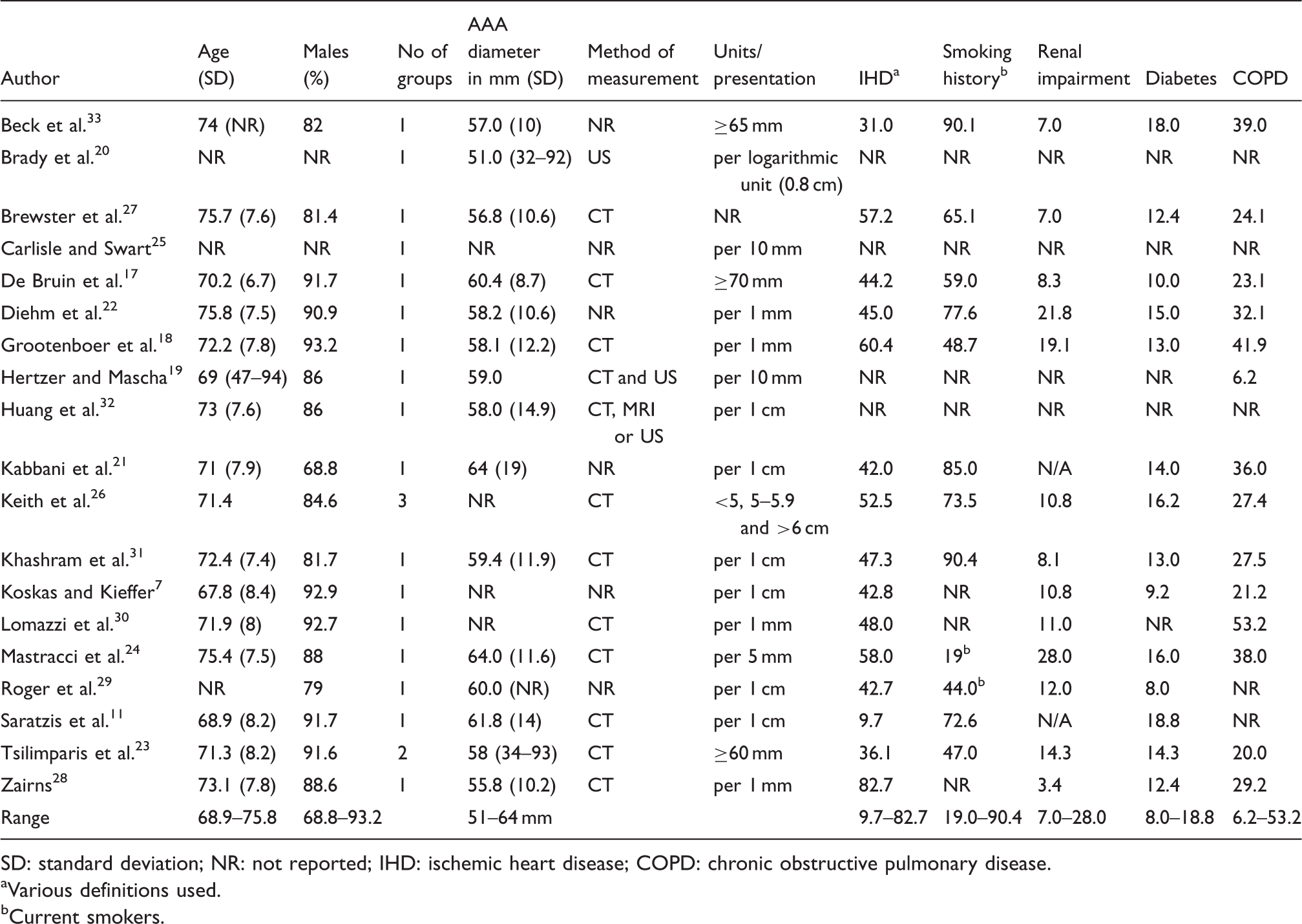
SD: standard deviation; NR: not reported; IHD: ischemic heart disease; COPD: chronic obstructive pulmonary disease.
Various definitions used.
Current smokers.
The full meta-analysis included 16 studies and 19,722 patients. All of the studies adjusted for age while several also adjusted for comorbid conditions (Table 1). Larger AAA diameter measured prior to AAA repair was associated with lower reported survival compared with smaller aneurysms. A 1-cm increase in AAA diameter was associated with a pooled HR of 1.14 (95% CI: 1.10–1.18), I2 = 48% (Figure 2). Excluding four studies with either categorical17,23,33 or logarithmic
20
AAA diameter conversions did not influence the overall risk – HR 1.13 (95% CI: 1.09–1.18), I2 = 50% for each increase in 1 cm of AAA diameter.
Meta-analysis of the effect of AAA size of late mortality following elective AAA repair (per 1 cm increase).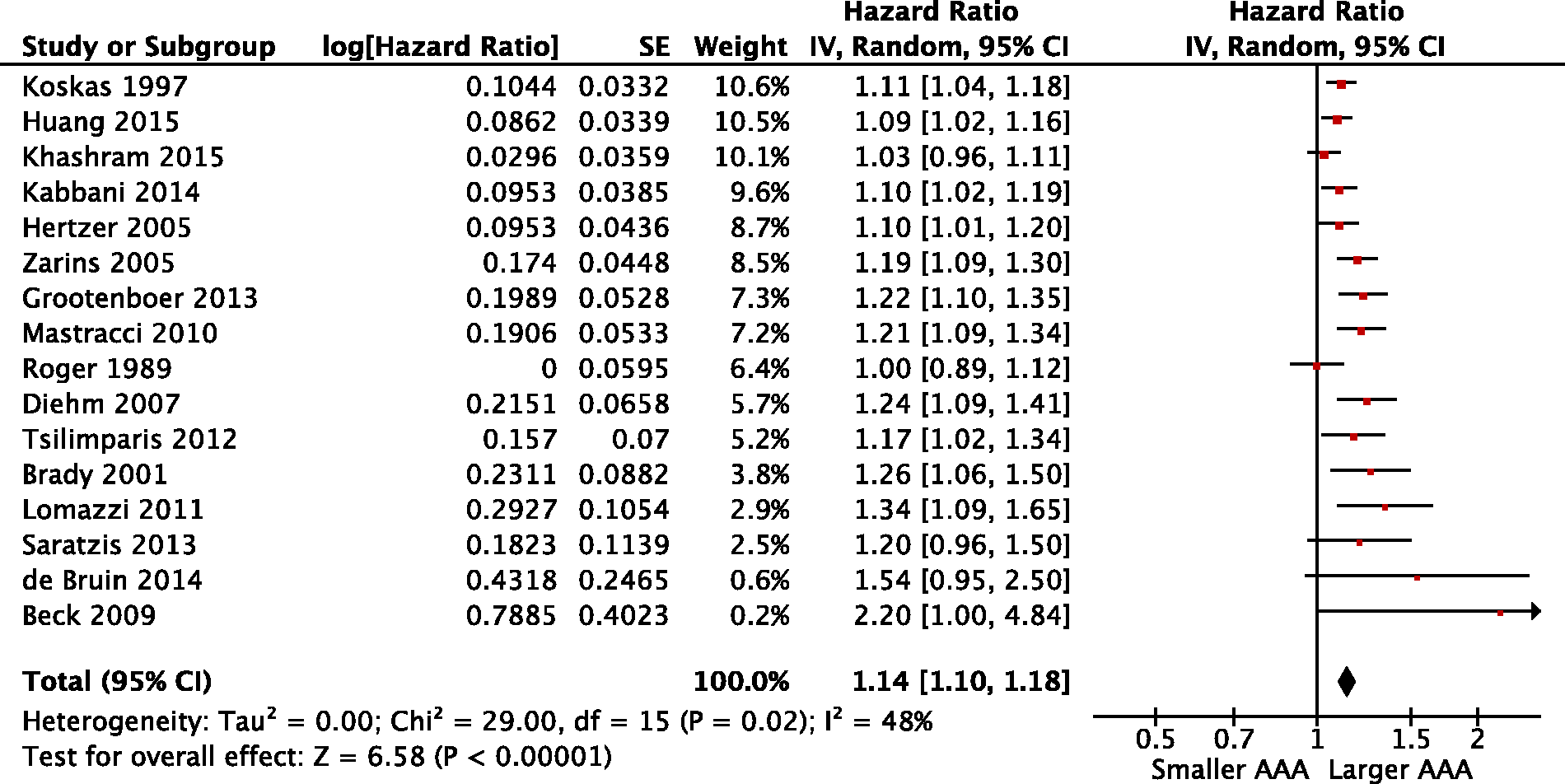
Thirteen studies were included in a subgroup analysis according to AAA repair type that included an equal weight (50%) for each category (Figure 3). EVAR was associated with a significantly higher mortality risk compared with OAR for each 1 cm increase in AAA diameter, pooled HR was EVAR 1.20 (95% CI: 1.15–1.25), I2 = 0% and OAR 1.08 (95% CI: 1.03–1.12), I2 = 12%, respectively (Figure 3). This subgroup analysis excluded two studies that included both EVAR and OAR in the same analysis,17,32 one study that categorized AAA diameter
23
and one that did not report how the AAA was repaired.
20
Subgroup analysis of AAA size according to type of repair (per 1 cm increase, EVAR: endovascular aneurysm repair, OAR: open aneurysm repair).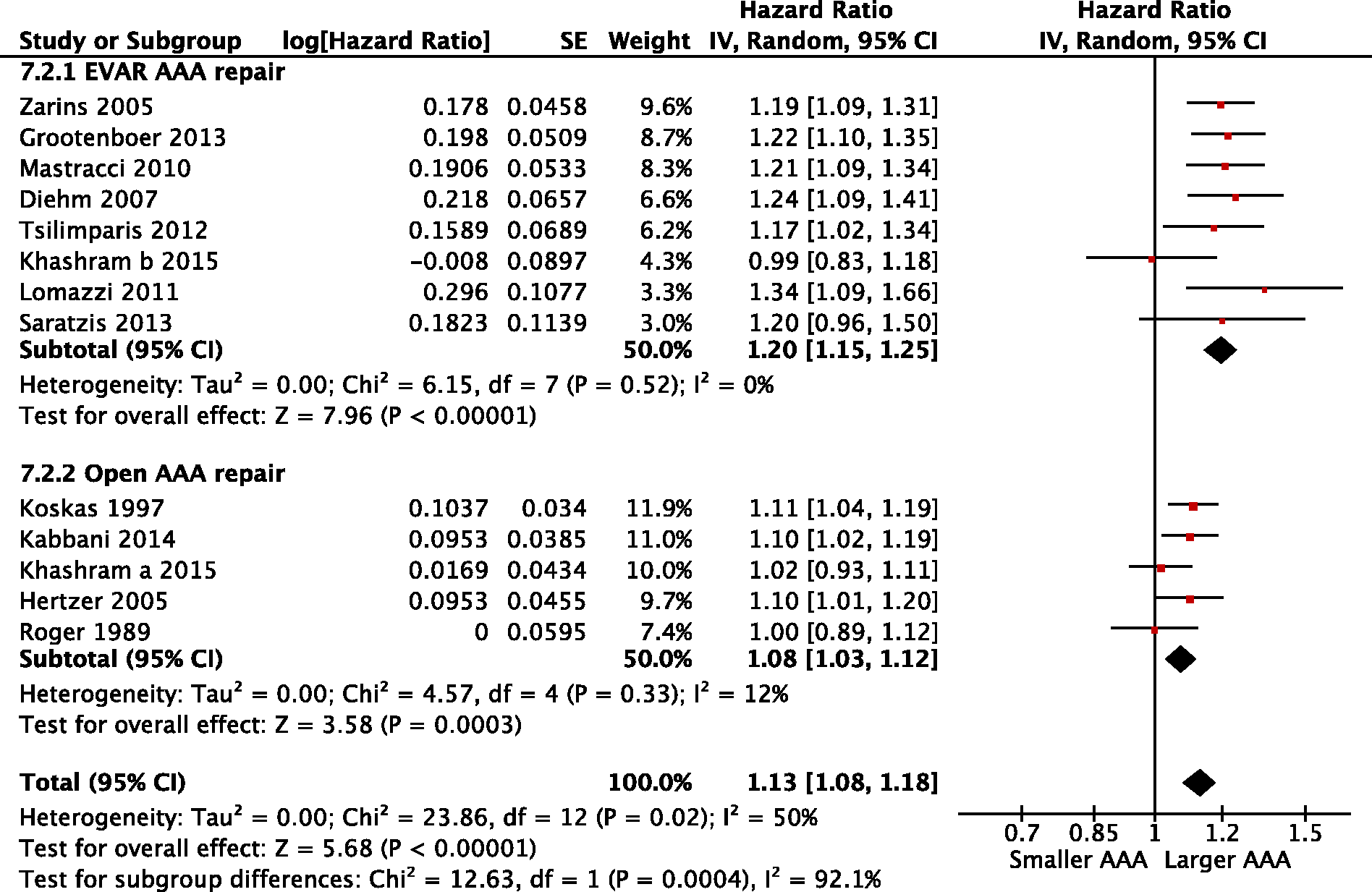
Meta-regression was undertaken to determine if the between-study heterogeneity could be accounted for by the mid-year of study or duration of follow-up; 16 studies contributed to mid-year of the study and 15 studies contributed to the duration of follow-up. There was an association for a decrease in log(HR) by duration of follow up (β = 0.998, 95% CI: 0.996–1.000, I2 = 24%, p < 0.013; Figure 4). There was no evidence of a change in log(HR) by mid-year study (β = 1.004, 95% CI: 0.999–1.010, I2 = 47%, p = 0.13).
Log(HR) of AAA size vs study follow-up. The solid line represents the regression line and the shaded gray area corresponds to the 95% CI. Each circle represents a different study and the size of the circle is proportional to the weight of study (inverse variance = 1/standard error
2
of the HR).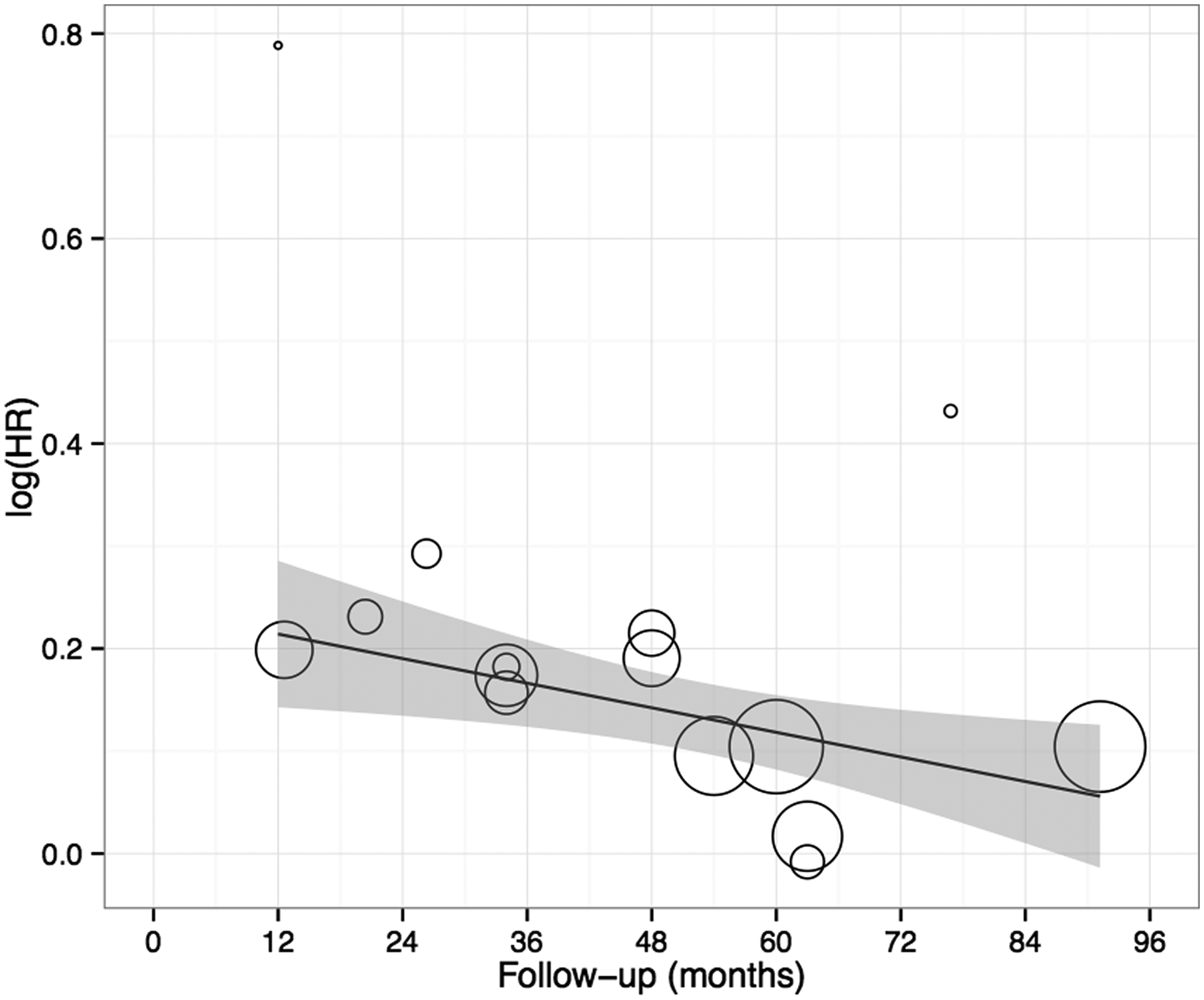
Discussion
Individualizing patient treatment to their specific demographics and comorbidities is warranted to improve long-term outcomes. This systematic review found that larger AAAs were independently associated with a lower survival following elective AAA repair and this observation was greater for EVAR than OAR.
AAA size has also been shown to be an important independent predictor of perioperative morbidity and mortality. Schouten et al. 34 reported on 500 patients undergoing elective open AAA repair and larger AAA diameter had a significantly higher risk of cardiovascular complications and mortality. A recent report from the Vascunet database included 5895 patients from six countries and concluded that the size of AAA was associated with higher perioperative mortality with an adjusted odds ratio of perioperative mortality for a 1-cm increase in AAA size in patients undergoing either OAR or EVAR of 1.14 (95% CI: 1.03–1.27) and 1.28 (95% CI: 1.06–1.55), respectively. 35 The diameter of AAA at the time of repair has also been associated with a decreased five-year survival as demonstrated by a recent meta-regression analysis including 13,281 patients treated between 1978 and 2011. 36
Why are larger AAAs associated with worse survival?
Based on the results from this meta-analysis, there appears to be two factors that could explain why larger AAAs may have a worse survival. First, this association was found in both types of repairs; therefore, a biological cause seems plausible. Larger AAA might exhibit more inflammatory mediators or larger size AAA might be associated with more advanced cardiovascular disease.8,23,34 Five studies provided group comparison between small and large AAA. The results from three large studies8,9,26 suggest that patients with larger AAA were older and had a greater burden of cardiovascular disease than patients with small AAA. In the two other smaller studies,10,23 there was no difference in morbidities between the groups. However, patient co-morbidities were adjusted for in the survival models and the influence of AAA size was an independent predictor of late survival.
Second, the effect estimate of AAA size of EVAR treatment was significantly higher in this analysis compared to the OAR group.
Nevertheless, this does not adequately explain why the association was greater in EVAR than OAR. Results from the Lifeline and EUROSTAR registries have also shown that an increase in AAA diameter was independently associated with a higher AAA related mortality, higher rupture post repair, re-intervention and surgical conversion to OAR.8,9,28 One might speculate that each re-intervention might have an additive mortality risk.
Roger et al. 29 were the first to include AAA size in a multivariate model, but AAA diameter was not a significant mortality predictor in their study. Almost a decade later, Koskas and Kfieifer 7 were the first to show that preoperative AAA size was an independent predictor of poor late survival. Interestingly, this finding appeared to generate little discussion, including within the reporting paper. It was not until subsequent EVAR data began to emerge, highlighting morphological aortic neck and iliac artery differences between small and large AAA that interest in this area has increased.8,9
Limitations
This systematic review has a number of potential limitations related to study selection and potential biases in reporting and publication. Specifically, as AAA diameter (>5.5 cm) has not been subjected to any randomized trials, it is possible that higher risk patients were selected to undergo EVAR and hence were more likely to experience higher late mortality. However, it was notable that three studies7,19,29 in the OAR group recruited patients prior to the EVAR era, and AAA diameter remained a negative predictor of late survival.
Furthermore, potential confounders that were not adjusted for in the analysis might have contributed to the findings of this review. For example, other anatomical features of AAAs such as short proximal necks or juxta/supra-renal aneurysms have been associated with worse outcomes and lower survival following AAA repair. Some of the earlier studies might have included first generation endovascular stent grafts that were associated with higher mortality and endoleak rates and might have influenced the results. 37 We excluded studies that only included such grafts to minimize the selection bias.
The outcome of interest in this analysis was overall patient survival during the reported follow-up period. This period ranged from 12 to 91.2 months and the metaregression at univariable level suggests an association of a decreased risk with larger AAA during follow-up. In addition, the long-term success of the index EVAR procedure and variations in endoleak rates and reporting is not accounted for. Future studies comparing endoleak rates, AAA diameter and the effect on aneurysm related mortality is warranted to better understand this relationship.
In addition, this review contains a mixture of study designs: single surgeon series, tertiary single center studies, national registries, treatment specific registries and post hoc randomized trials. Therefore, heterogeneity is expected in such an analysis. We were able to reduce heterogeneity by grouping studies into type of repair (OAR and EVAR).
As more AAA are repaired with endovascular therapy and open repair is reserved for a selected population, 38 estimating the influence of AAA diameter in relation to repair method will be susceptible to selection biases. We recommend that future studies reporting on late predictors of survival following AAA repair should include AAA diameter within the predictive modeling. In addition, AAA measurements should be kept as continuous data. 39 When applicable, separating the analysis according to type of repair might shed further light on the influence of repair type in relation to late survival.
Conclusion
In conclusion, best estimate from the published literature appears to indicate that preoperative AAA diameter influences late survival following elective AAA repair. Larger AAA is associated with poorer survival and this association is greater for EVAR than OAR.
The inclusion of AAA diameter in the clinical decision-making process, therefore, seems warranted when considering the most appropriate surgical management option for individualizing patient care.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.