
Abstract
Purposes
The aim of this study was to evaluate the risk factors for the two-year survival after revascularization of critical limb ischemia.
Methods
Between 2008 and 2012, 142 patients underwent revascularization. A retrospective analysis was performed to measure the risk factor.
Results
A total 85 patients underwent surgical revascularization, 31 patients underwent endovascular therapy while 26 patients underwent hybrid therapy. By multivariate analysis, the following variables were considered to be risk factors: ejection fraction <50 % (HR, 3.14; 95% CI, 1.22–7.95; P = 0.02), serum albumin level <2.5 g/dL (HR, 3.45; 95% CI, 1.01–11.7; P = 0.04) and nonambulatory status (HR, 4.11; 95% CI, 1.79–9.70; P < 0.01). The two-year survival rate of the patients with no risk factors was 85.5%, while the patients with at least one risk factor had an unfavorable prognosis (one; 56.7%, two; 45.4%).
Conclusions
The nonambulatory status, serum albumin level <2.5 g/dL and ejection fraction <50% were the risk factors for the two-year mortality after revascularization in critical limb ischemia patients. These risk factors may be useful for the treatment strategy of critical limb ischemia patients.
Introduction
Patients with critical limb ischemia (CLI) are vulnerable to the risk of major amputation or a poor prognosis.1–3 Survival of CLI patients at one year ranges between 10% and 40%. The Bypass versus Angioplasty in Severe Ischemia of the Leg (BASIL) trial in 2005 showed that surgical revascularization was recommended for CLI patients who were likely to survive more than two years after revascularization. 4 Previous reports have utilized various scoring models after revascularization of CLI patients. The Goodney score predicts the one-year survival rate after surgical revascularization. 5 The Finnvasc score predicts the 30-day mortality rates after infrainguinal surgical revascularization for CLI patients. 6 The PREVENT III score showed the risk score for the prediction of the amputation-free survival in patients undergoing infrainguinal autogenous vein bypass. 7 However, these scoring models did not represent the two-year morality after revascularization for CLI patients. Recently, the BEACH score has been demonstrated to indicate the two-year predictors after revascularization in CLI patients. 8 This retrospective study analyzed the risk factors for the two-year mortality of 459 CLI patients (endovascular therapy [EVT]; 396 patients, bypass surgery; 63 patients). This study found that an age over 75 years, nonambulatory status, regular dialysis and ejection fraction <50% were independent risk factors for the two-year mortality.
Although several risk factors have been reported, the prognostic factor for the two-year survival after revascularization for CLI remains unclear. The aim of this study is to investigate the risk factors of the two-year mortality after revascularization for CLI.
Methods
Between January 2008 and December 2012, 142 patients and 158 limbs underwent surgical or endovascular revascularization at the Department of Surgery and Science, Graduate School of Medical Sciences, Kyushu University. Approval for this project was obtained from the institutional review board for research on human subjects. A retrospective analysis was performed, and the patient’s data were obtained from the medical, operative and radiology records. Patients with acute limb ischemia were excluded from this analysis. The main outcome measures were the risk factor of the two-year mortality after revascularization for CLI.
The current treatment strategy for CLI in our institution is as follows. For an aortoiliac (AI) lesion, EVT is the first-line strategy. In a femoropopliteal (FP) lesion, EVT is first-line strategy for TASC II A or B lesions, whereas, patients with TASC II C or D lesions are treated by surgical revascularization. For an infrapopliteal lesion, surgical revascularization is the first choice for long chronic total occlusion (CTO). The patients with local stenosis or short segment CTO are treated by EVT as the first-line strategy. In the EVT procedure, primary stenting was performed for AI lesions. For FP lesions, a nitinol stent was implanted in patients with residual stenosis over 30% or a flow limiting dissection after balloon angioplasty. In infrapopliteal lesions, balloon angioplasty was performed. In surgical revascularization, a prosthetic graft was used in for AI lesions and above-knee popliteal bypass, whereas, an autogenous vein graft was used for an infrapopliteal bypass.
Various risk factors were analyzed in this study: age, hypertension, diabetes mellitus, hyperlipidemia, coronary artery disease, cerebrovascular disease, hemodialysis, the Fontaine classification, the ejection fraction, the serum albumin level and the activity of daily living (ADL). We assessed ADL before the development of CLI. If becoming unable to walk because of ulcer formation, the patients are assessed as ambulatory status. The characteristics and distribution of the risk factors in the patient groups were analyzed using the χ2 tests for categorical variables and the t test for continuous variables. A univariate Cox proportional hazards regression model was used to investigate the association of the preoperative characteristics with the two-year mortality. The preoperative variables with a P value <0.1 in the univariate analysis were included in the regression model. For the assessment of amputation free survival (AFS) and the prognostic outcomes, the Kaplan-Meier life table method was employed, and comparisons were made using Wilcoxon and log-rank analyses. Statistical significance was considered to exist at a P value of <0.05. All statistical analyses were conducted using the JMP® 10 software program (SAS Institute Inc., Cary, NC, USA).
Results
Characteristics of patients.
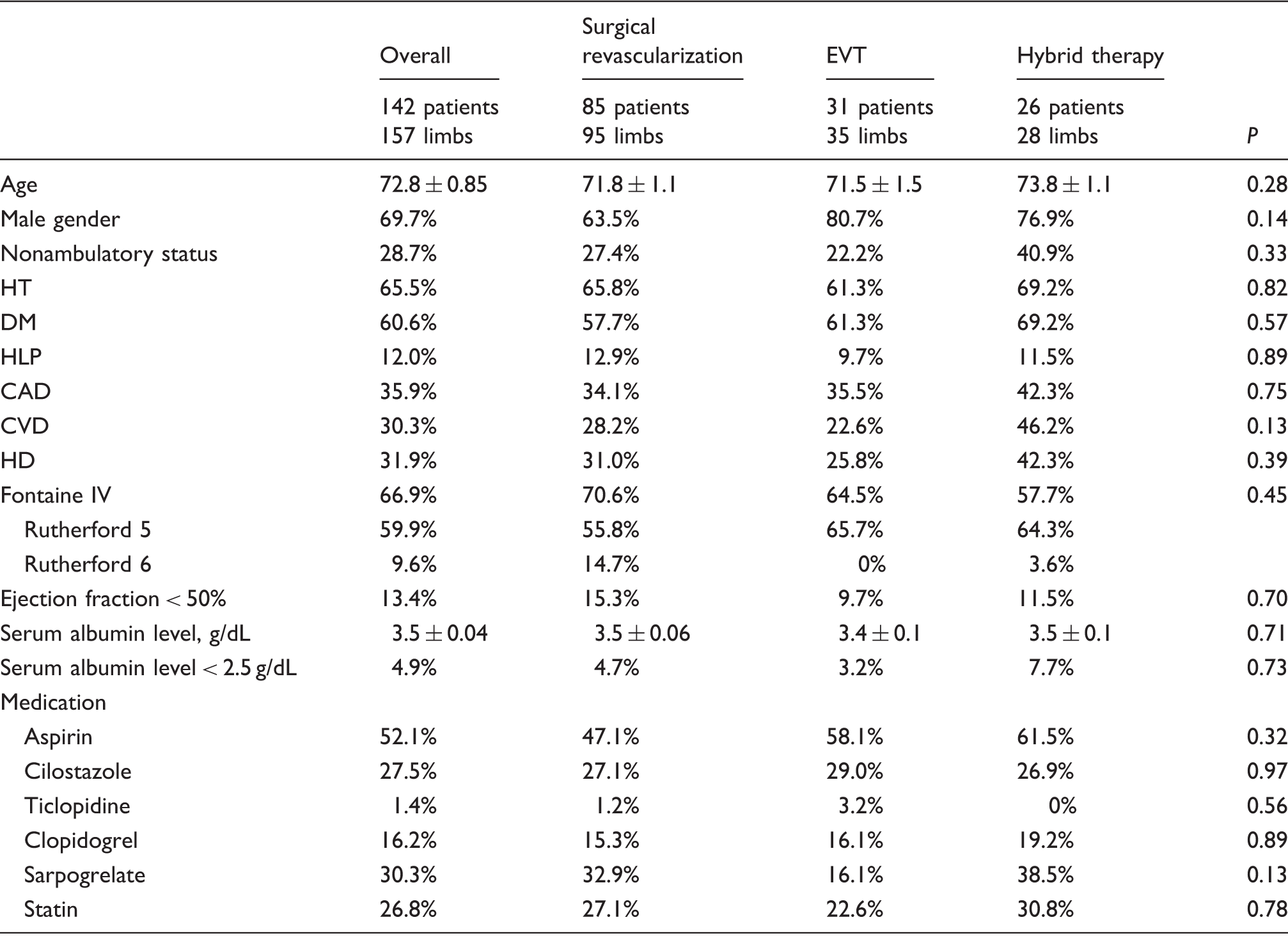
EVT: endovascular therapy; HT: hypertension; DM: diabetes mellitus; HLP: hyperlipidemia; CAD: coronary artery disease; CVD: cerebrovascular diseases; HD: hemodialysis.
The summary of treatment for 142 CLI patients and 158 limbs.
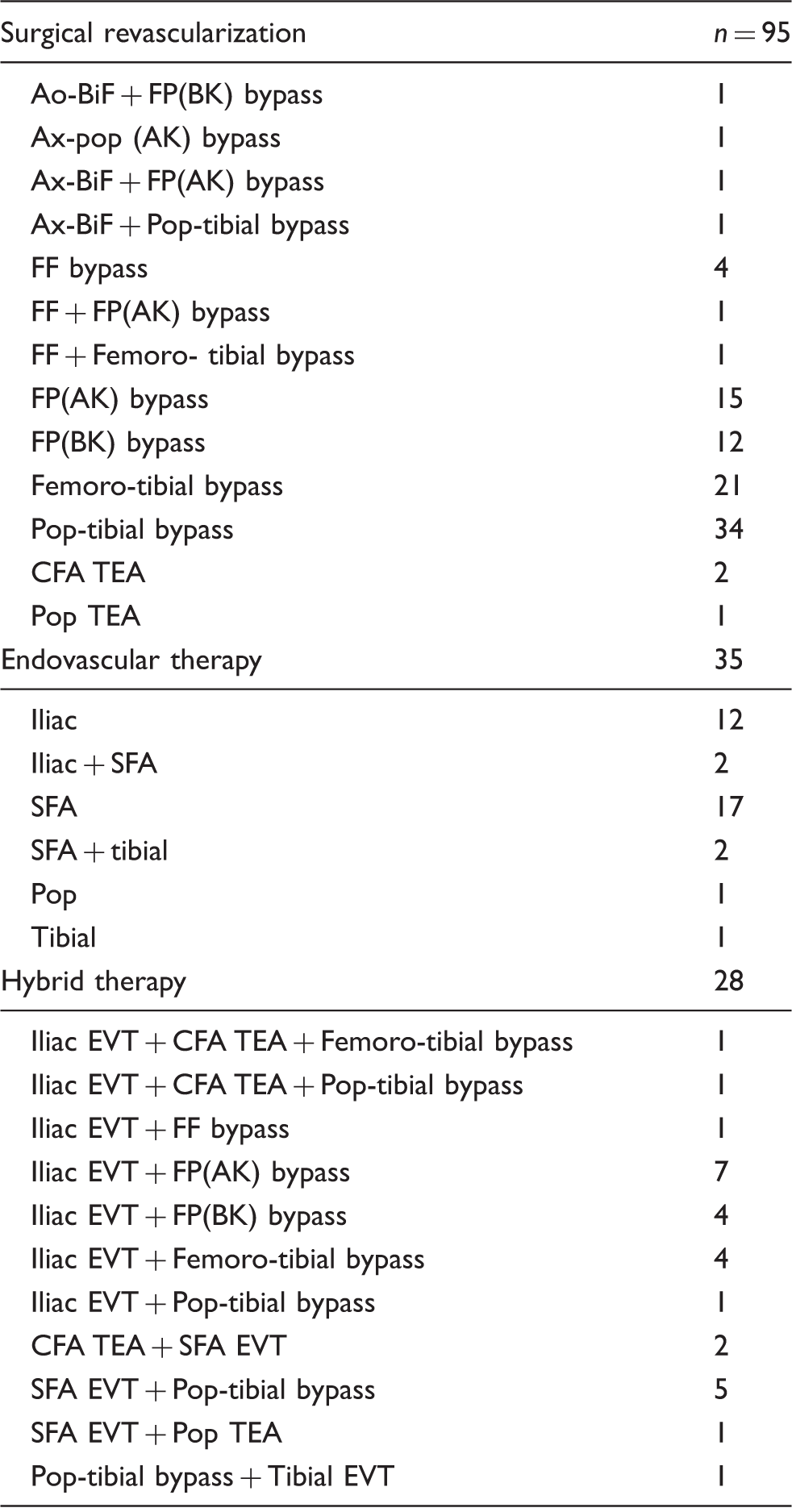
Ao-BiF: Aortobifemoral; FP: femoro-popliteal; BK: below the knee; Ax-pop: Axillo-popliteal; AK: above the knee; Ax-BiF: axillobifemoral; pop: popliteal; FF: femorofemoral; CFA: common femoral artery; TEA: thrombendarterectomy; SFA: superficial femoral artery.
Infection comprised the highest cause of two-year mortality, followed by cardiac death and respiratory failure due to pneumonia or chronic obstructive pulmonary disease (Figure 1).
The cause of death within two years after revascularization. Infection was high proportion of cause of death, followed by cardiac death and respiratory failure.
Univariate analysis.
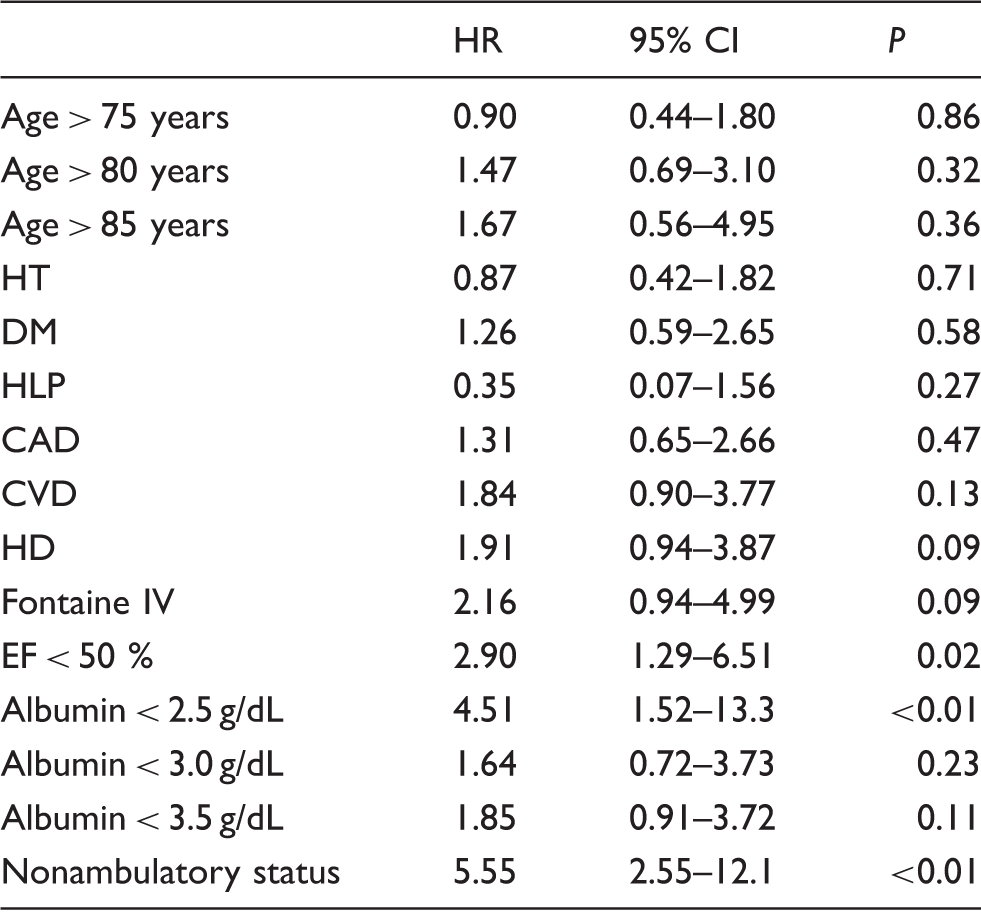
HT: hypertension; DM: diabetes mellitus; HLP: hyperlipidemia; CAD: coronary artery disease; CVD: cerebrovascular disease; HD: hemodialysis; EF: ejection fraction.
The Kaplan-Meier curves showed AFS in Figures 2 and 3: one-year AFS 81.2% in overall, 84.0% in bypass surgery, 92.1% in EVT and 59.9% in hybrid therapy.
Kaplan-Meier curves of amputation free survival (AFS) after revascularization for critical limb ischemia; one-year AFS 81.2% in overall. Kaplan-Meier curves of amputation free survival (AFS) after revascularization for critical limb ischemia; one-year AFS 84.0% in bypass surgery, 92.1% in EVT, and 59.9% in hybrid therapy.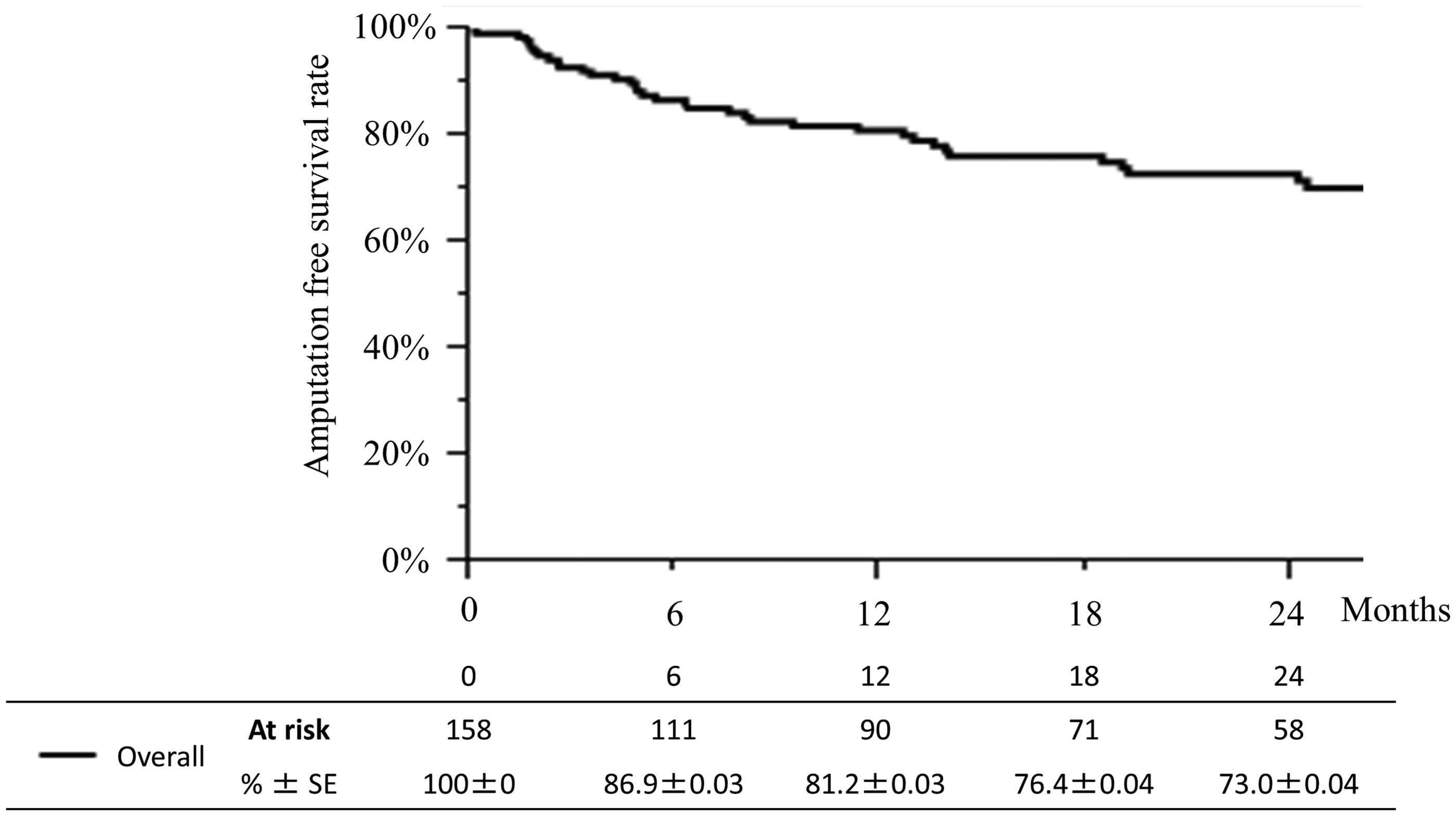
The two-year survival rate of the patients with no risk factors was 85.5%, while the patients with at least one risk factor had an unfavorable prognosis; the two-year survival rates for one risk factor and two risk factors were 56.7% and 45.4%, respectively (Figure 4).
Risk stratification by the number of risk factors after multivariate analysis. Two-year survival rate of the patients with no risk factor was 85.5%, while the patients with at least one risk factor were unfavorable prognosis; one risk factor 56.7% and two risk factor 45.4% at two-year survival rates. SE: standard error.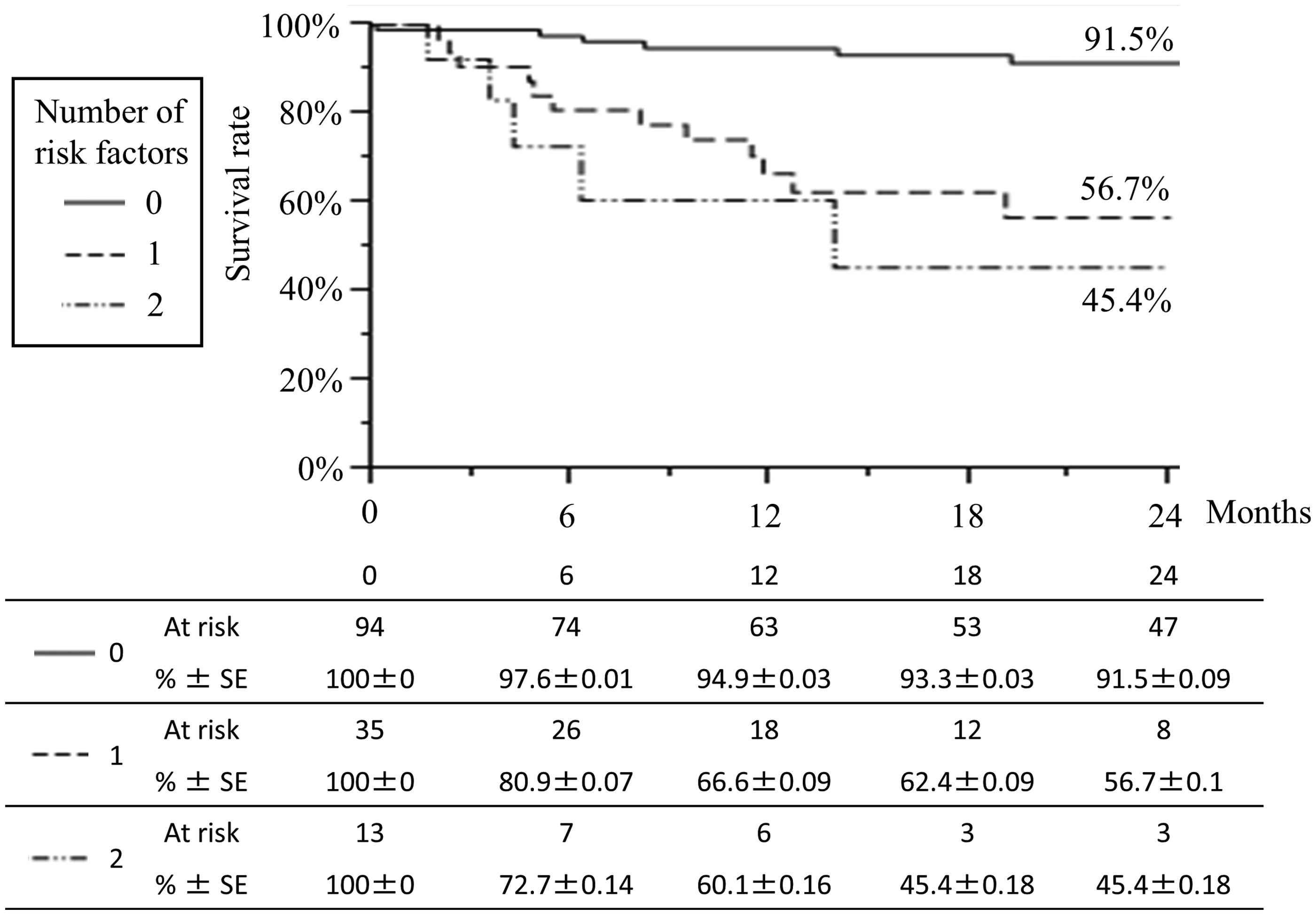
Discussion
The BASIL trial in 2005, which is the only available randomized controlled trial (RCT) of CLI patients, showed surgical revascularization was recommended for CLI patients who were likely to survive more than two years after revascularization. 4 However, the prognostic factor for the two-year survival after revascularization for CLI remains unclear. The aim of this study was to investigate the risk factors of the two-year mortality after revascularization for CLI patients. In this study, the risk factors of the two-year mortality after revascularization for CLI patients were nonambulatory status, ejection fraction <50% and serum albumin level <2.5 g/dL. The patients with at least one risk factor had a poor prognosis at the two-year time point. These risk factors may be useful for the treatment strategy of CLI patients. In regard to AFS, previous reports showed one-year AFS range from about 60% to 80%. 9 In this study, one-year AFS was 81.2% in overall similar to previous reports. Considering this result, our treatment strategy of CLI patients are generally acceptable.
Previous reports showed various scoring models after revascularization. The Goodney score predicts the one-year survival after surgical revascularization. 5 The following factors were identified to be risk factors: congestive heart failure, diabetes, CLI, lack of single-segment saphenous vein, age over 80 years, dialysis and emergency operation. The Finnvasc score indicate the 30-day mortality rates after infrainguinal surgical revascularization for CLI patients. 6 Diabetes, coronary artery disease (CAD), foot gangrene and urgent operation were independent predictors of the 30-day mortality. The PREVENT III score showed the risk score for the prediction of the amputation-free survival in patients undergoing infrainguinal autogenous vein bypass. 7 Dialysis, tissue loss, age over 75 and CAD were identified to be risk factors. However, these scoring models did not predict the two-year morality after revascularization for CLI patients. Recently, the BEACH score represents two-year predictors after revascularization in CLI patients. 8 This retrospective study analyzed the risk factors for the two-year mortality of 459 CLI patients (EVT; 396 patients, bypass surgery; 63 patients). And found that age over 75 years, nonambulatory status, regular dialysis and ejection fraction <50% were independent risk factors for the two-year mortality. Taking these results together, various factors were evaluated to reveal the risk factors for the two-year survival after revascularization of CLI patients.
Multivariate analysis.
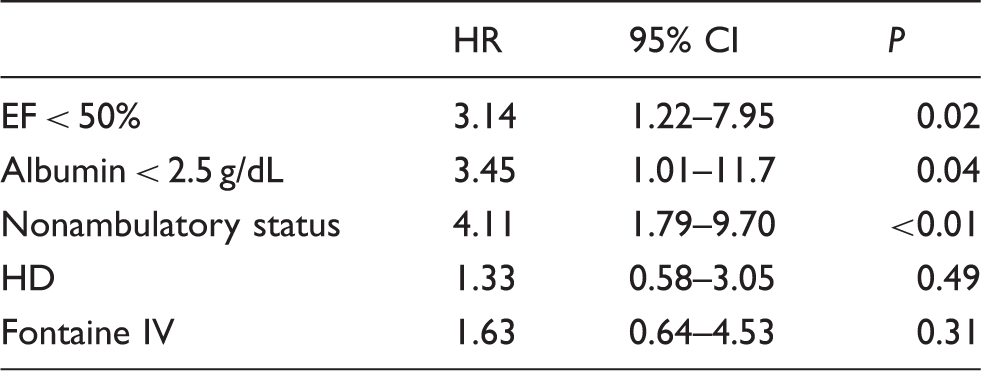
EF: ejection fraction; HD: hemodialysis.
Our study was differed from the BEACH trial is sseveral manners. First, the proportion of the patients treated with surgical revascularization was larger in the present study compared to the BEACH study. Furthermore, the number of patients with a nonamburatory status was larger in the BEACH registry, which may have lead to the outcome that many of the patients were treated by EVT due to a poor general status. Thus, our findings could serve as a reference for CLI patients predominantly using surgical revascularization.
Recently, our colleague reported sarcopenia to be a prognostic factor for CLI patients. 12 Sarcopenia is diagnosed by the presence of both a low muscle mass and low muscle function according to the European Working Group on Sarcopenia in Older People guidelines. 13 Sarcopenia caused by various factors such as aging, disuse atrophy and a low nutrient condition. In the present study, low albumin level and nonambulatory status were found to be independent risk factors for the two-year mortality after revascularization. Considering that a poor nutritional condition and disuse atrophy are some of the causes of sarcopenia, sarcopenia may also be associated with the two-year survival rate. For the evaluation of the muscle mass, computed tomography (CT) is necessary. However, CT was not performed in the preoperative examination in all CLI patients; therefore, sarcopenia could not be evaluated in the present study.
In the treatment strategy of CLI patients, the BASIL trial is the only available RCT trial to date, which recommended surgical revascularization for the patients who were likely to survive more than two years after revascularization. However, whether it is appropriate to consider the two-year prognosis for the selection of treatment for CLI patients according to a single RCT is unclear. It is very difficult to precisely predict the two-year mortality after revascularization in CLI patients in clinical practice. Furthermore, some treatments may be the only option according to the patient’s general status, the degree of ischemia or infection in order to avoid major amputation. While several scoring models have been suggested by previous reports, common risk factors such as an advanced age, daily dialysis, the deterioration of cardiac function and nonambulatory status have emerged. Therefore, in order to improve the prognosis of CLI patients, the treatment strategy of CLI should be individualized according to the patient’s risk factors. The findings of the present study may lead to another scoring model that is useful for the treatment strategy of CLI patients. Surgical revascularization may be a better indication in CLI patients without these risk factors.
There are several limitations associated with this study. First, this study was a retrospective study with a small number and the patients were not randomized to treatment. Second, there may be a treatment selection bias. We treated CLI patients according to our treatment strategy; however, a selection bias cannot be ruled out completely because of only a single institution and retrospective study. Furthermore, a precise prediction model for CLI patients is needed.
Conclusion
The nonambulatory status, serum albumin level <2.5 g/dL and ejection fraction <50% were found to be risk factors for the two-year mortality after revascularization in CLI patients. These risk factors may be useful for the treatment strategy of CLI patients regarding the result of the BASIL trial for the two-year survival rate.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.