
Abstract
Introduction
The office-based endovascular facility has increased in number recently due in part to expedient patient experience. This study analyzed treatment outcomes of procedures performed in our office-based endovascular suite.
Methods
Treatment outcomes of 5134 consecutive procedures performed in our office-based endovascular suites from 2006 to 2013 were analyzed. Five sequential groups (group I–V) of 1000 consecutive interventions were compared with regard to technical success and treatment outcomes.
Results
Our patients included 2856 (56%) females and 2267 (44%) males. Procedures performed included diagnostic arteriogram, arterial interventions, venous interventions, dialysis access interventions, and venous catheter management, which were 1024 (19.9%), 1568 (30.6%), and 3073 (60.0%), 621(12.1%), and 354 (6.9%), respectively. The complication rates for group I, II, III, IV, and V were 3%, 1.5%, 1%, 1.1%, and 0.7%, respectively. The complication rate was higher in group I when compared to each of the remaining four groups (p < 0.05). Nine patients (0.18%) died within the 30-day period following their procedures, and none were procedure related.
Conclusions
Endovascular procedure can be performed safely in an office-based facility with excellent outcomes. Lessons learned in establishing office-based endovascular suites with efforts to reduce procedural complications and optimize quality patient care are discussed.
Introduction
The office-based surgical practice has emerged as an alternative to hospital-based surgical practice as a result of advances in anesthesia care, improvement in minimally invasive surgical techniques, and patient preference due to expedient perioperative experience. The shift of practice into the office-based setting offers some significant cost-effective solutions to surgical care, with one study reporting 60–75% reduction in health care costs.1,2 Many studies have demonstrated concurrent benefits of increased patient satisfaction and expeditious patient experience.3,4 These factors have led to an exponential growth in office-based surgical practices, which is rapidly redefining how health care is being delivered. Several recent reports noted that the proportion of outpatient and office-based surgeries have increased from a meager 10–15% in the early 1990s to closer to 60% today.3,4
The rapid expansion of these outpatient surgical facilities in recent years has similarly led to many office-based practice developments in the vascular surgical practice. The Deficit Reduction Act of 2005 coupled with advances in endovascular techniques have resulted in significant growth of office-based vascular interventional facilities. Since the establishment of our first office-based endovascular suite in 2006 in Los Angeles, CA, we have routinely performed outpatient arterial and venous diagnostic angiographic and therapeutic procedures. The growth of our practice has led to further expansion of office-based endovascular facilities in Dallas, TX. In this report, we examined the treatment outcomes of our office-based procedural experience and discussed various lessons learned to ensure optimal patient care quality in this clinical practice.
Patients and methods
This study consisted of a retrospective review of the 5134 consecutive endovascular procedures performed by vascular surgeons in our office-based endovascular suites, located in California and Texas, between April 2006 and December 2013. Data was collected under a protocol approved by the Institutional Review Board in compliance with the Health Insurance Portability and Accountability Act (HIPAA) standards. After opening our center in April 2006, Vascular Management Associates (VMA, Los Angeles, CA) has managed all the patients' office data including office-based endovascular procedures and its outcomes. By using a specialized endovascular procedure patient registering program, Vascunote® (VMA), we obtained the patient's demographic data, risk factors and ASA classification that were entered prospectively. Proportions of each procedure type were calculated and procedure-related complications, hospital transfer cases and 30 day mortality cases were collected. Office-based endovascular facilities are located in Dallas, TX and Los Angeles, CA which were clinical practices of the senior author, and these procedures were performed by physicians within these respective practices. For the purpose of comparison, analysis was performed in five sequential cohorts of groups (I–V) with each containing 1000 consecutive procedures.
Selection criteria and definitions
Prerequisites included an adult accompanying the patient for 24 hr following the procedure, access to communication system and hospital, comprehension of the intervention and complications, acceptable laboratory value of complete blood count, prothrombin time (international normalized ratio) and partial thromboplastin time, and clearance from other specialists if the patient had significant medical issues in the past. Indications for the procedures were peripheral vascular disease, chronic venous insufficiency, varicose veins, extremity ulcers, malfunctioning dialysis access and thoracic outlet syndrome. Peripheral arterial interventions, dialysis access interventions, and venous thrombectomy or related endovascular interventions were routinely performed at the angiosuite.
Patients were selected for each procedure according to procedure indications by the respective surgeon. If patients were not in emergency and did not meet any of the following exclusion criteria such as baseline creatinine level greater than 2.0 mg/dl, serum potassium level greater than or equal to 5 mg/ml and BMI greater than or equal to 35 kg/m2, they were thought to be well qualified as office-based procedure candidates.
Procedure related complication was defined as any event which occurred during the entire endovascular and anesthetic procedure and which needed further treatment such as blood transfusion, surgery, or observation with hospitalization.
Setting and procedure
Patients referred for procedure after consultation with the vascular surgeon were processed by our nursing staff. Nurses followed a set protocol for pre-assessment, including patient history, scheduling and pre-procedure instructions. Our facilities include an angiography table, portable C-arm, anesthesia cart, and a full endovascular inventory including any devices that the surgeons may request. Additionally, there is a fully stocked crash cart in close proximity to the anesthesia cart in case an emergency arises.
All patients were provided with some level of sedation. In most cases, certified registered nurse anesthetists or board certified anesthesiologists examined the patients before going into the procedure room. However, in the case of young and healthy patients with no serious previous medical issues, registered nurses experienced in conscious sedation would provide the same examination under the supervision of a physician. Local anesthesia was provided by the surgeon in all cases, while the anesthesiologists and nurse anesthetists provided monitored anesthesia care. Two registered nurses provided conscious sedation under the supervision of the surgeon.
Access was achieved most commonly by a retrograde, contralateral approach but brachial, radial, antegrade femoral, popliteal, dorsalis pedis, posterior tibial or dialysis access approaches were also performed in selected cases. In all cases, ultrasound guidance and 5F, 6F, or 7F sheaths were used, followed by a bolus of 50–75 UI/kg of heparin intravenous injection. An angiogram was performed after these procedures to assess the technical results and punctured vessel conditions. Closure was achieved via a closure device for all femoral arterial punctures (Angioseal®, Perclose®, Starclose®, Exoseal®, or Mynx®). To minimize closure device related complications, an algorithm for optimal utilization of closure devices was developed. For more distal access sites, and dialysis access approaches, TR Band® or simple skin suture and manual compression were applied in obtaining and maintaining hemostasis.
Postoperative care
After the procedure, the patient was transferred to the recovery room in our office under the supervision of a dedicated nurse responsible for monitoring vital signs, peripheral pulses, and the access site. The anesthesia provider accompanied the patient to the recovery room for a time to evaluate the patient's response of the anesthesia and provided follow up care if needed. Following placement of a closure device, the patient sat up in bed within 30–60 min and was mobilized within 1–2 hr.
Patients were issued oral and written instructions to be followed for the subsequent 24 hr. Immediate management of bleeding at the puncture site was explained. This constituted explicit instruction regarding oozing, swelling, and frank pulsatile bleeding from the access site. The patient was instructed to visit the emergency room in the event of any such complication after being discharged from our office recovery room. For any other complication, including pain or coldness of the limb, the patient was instructed to call the office at any time. Patients were advised to limit their activities and to avoid heavy lifting for 24 hr after the intervention.
Within 24–48 hr post-procedure, a registered nurse routinely called the patient to follow up. Patients were also followed-up in each surgeon's clinic 1–2 weeks after the procedure. The evaluation included a clinical examination and non-invasive vascular tests such as ankle-brachial index (ABI) and Duplex ultrasound in all patients.
Statistical analysis
In the analysis, continuous variables were presented as mean ± SD and categorical variables were listed as count and percent. Patient demographic, co-morbidity information, as well as perioperative information was recorded and analyzed. In addition to procedural-related complications, other relevant procedural-related factors, such as procedural time, contrast load, recovery time, and hospital admission rates were analyzed among five patient groups for potential learning curve. A Cox regression model, in a stepwise procedure, was used to identify the most predictive variables associated with procedural related complications. Chi-square analysis and paired Student's t-tests were performed where appropriate; statistical significance was assumed at p < 0.05. Statistical analysis was performed using SPSS version 20.0 (SPSS Inc., Chicago, IL, USA).
Results
During the study period, 4832 patients underwent 5123 endovascular procedures in our office-based endovascular facilities, located in California and Texas. The patient population was 2856 (56%) female and 22,67 (44%) male (average age of 69 ± 7.6, range 15–107). The most common co-morbidities were hypertension in 2965 (58%), diabetes in 1684 (33%) and coronary artery disease in 1187 (23%). The vast majority of these patients were ASA classification I, II, or III, while 675 (13.1%) patients were class IV, all of whom were dialysis patients.
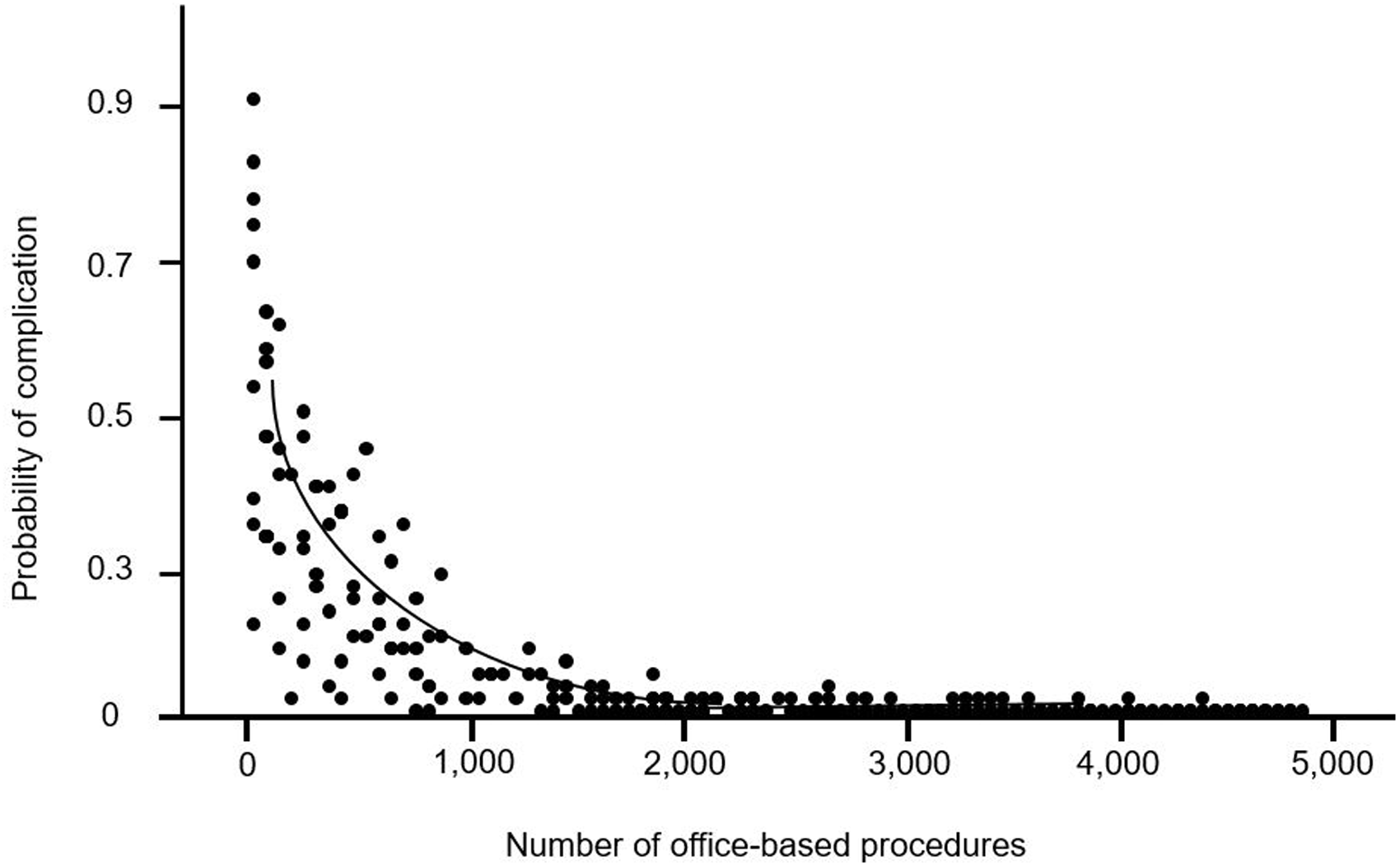
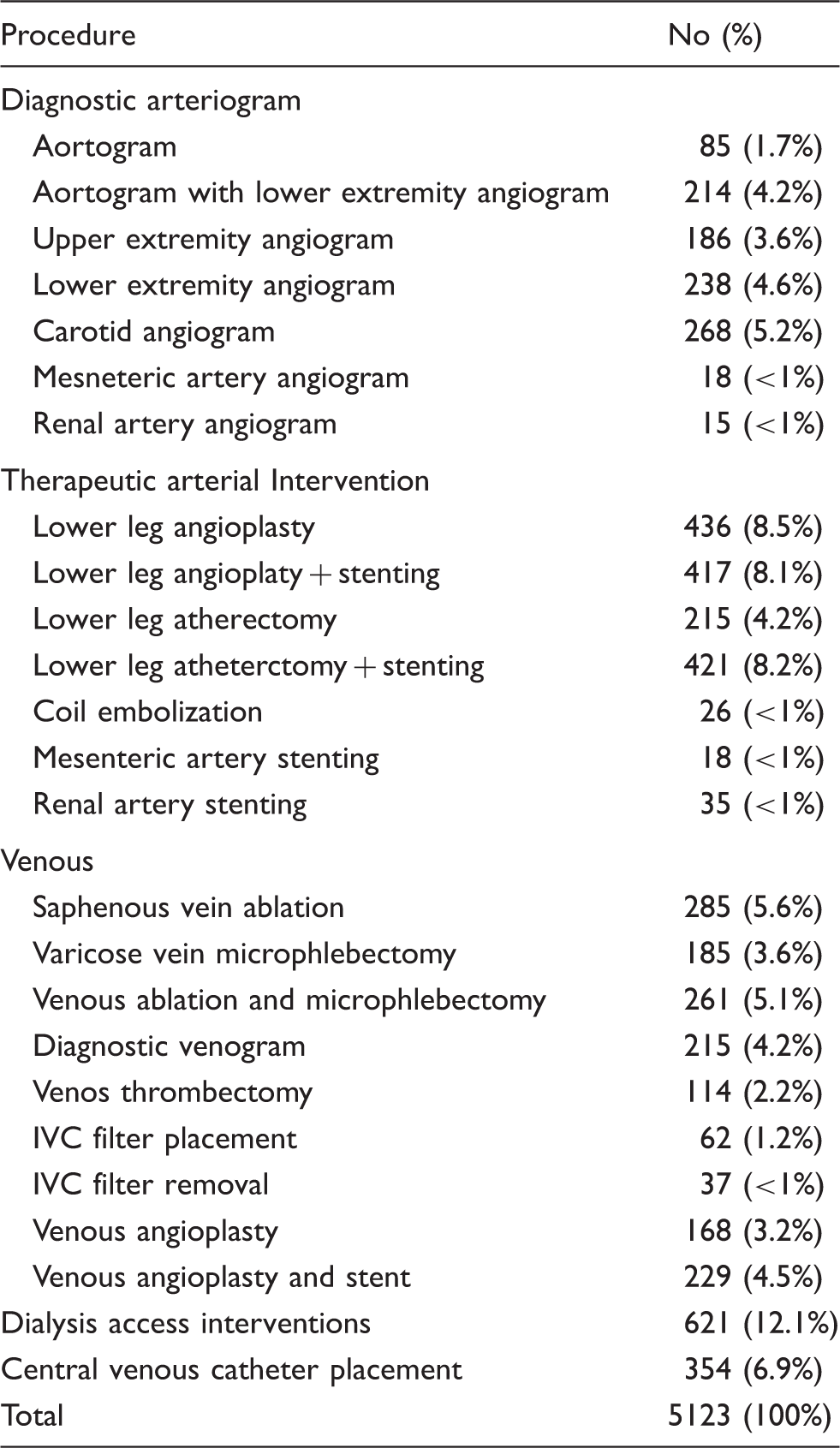
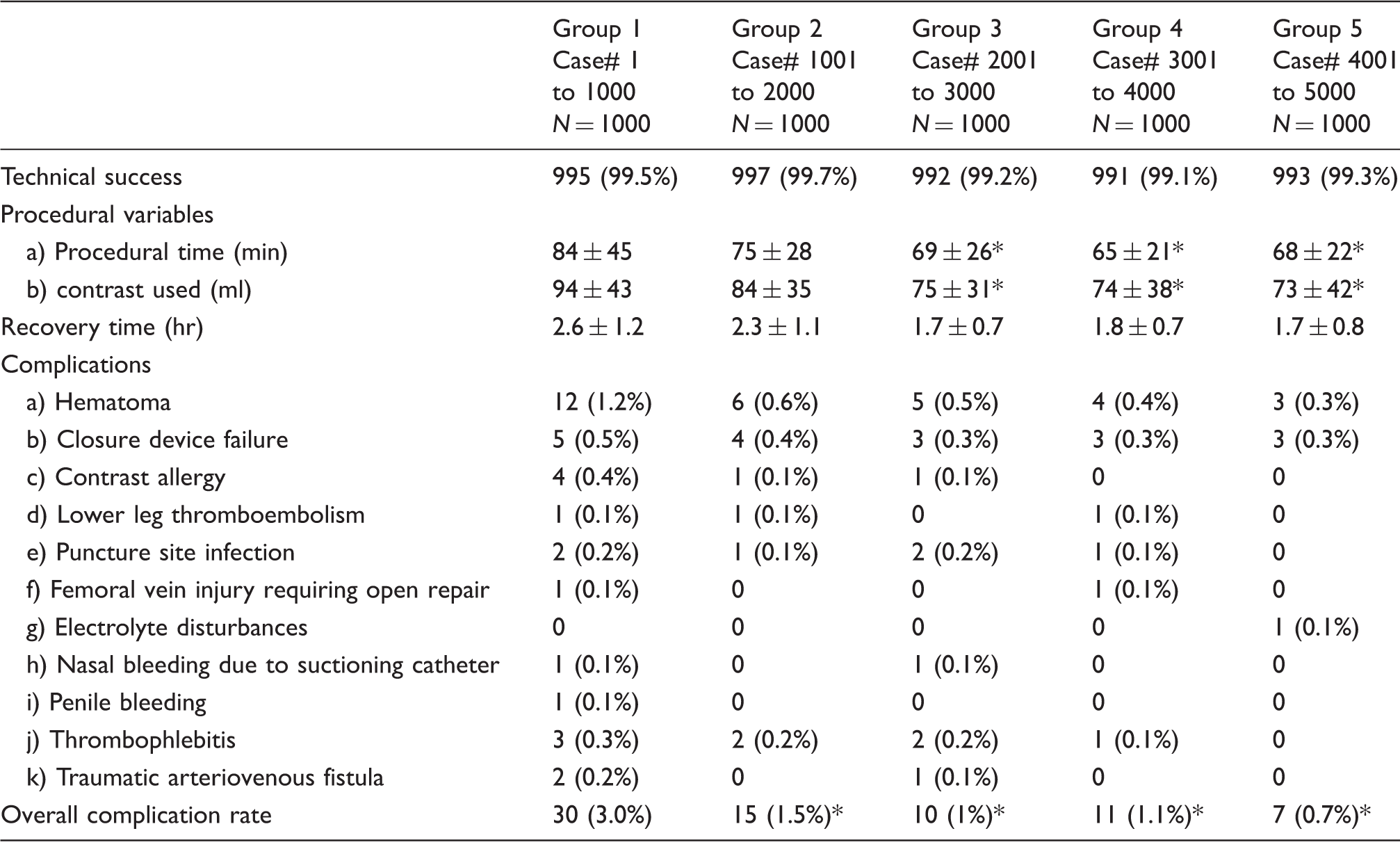
All procedures were performed by board certified vascular surgeons, and detailed breakdown of these procedures are shown in Table 1. Briefly, diagnostic arteriogram, therapeutic arterial interventions, and venous interventions were 1024 (19.9%), 1568 (30.6%), and 3073 (60.0%), respectively. Additionally, dialysis access related interventions and central venous catheter placement were 621(12.1%) and 354 (6.9%), respectively. Table 2 displays technical success, procedural variables, and procedural related complications of our patients. No difference in technical success was noted among the patient groups. As our experiences increased, progressively shorter procedural time and decreased contrast used were noted in the most recent three groups (p < 0.05). Graphic analysis of procedural time versus number of office-based procedures was shown in Figure 1. The complication rates for group I, II, III, IV, and V were 3%, 1.5%, 1%, 1.1%, and 0.7%, respectively. The complication rate was significantly higher in group I when compared to each of the remaining four groups (Table 2). Procedural complications occurred in 73 cases, which resulted in an overall complication rate of 1.4%. From these complications, 18 (0.35%) needed semi-elective admission for observation, 15 (0.29%) required immediate hospitalization for conservative treatment, and 7 (0.13%) required emergency surgery for either hematoma evacuation or thromboembolectomy procedures. Using a Cox proportional regression risk analysis to assess procedural complications, low procedural volume (p = 0.03) was identified as predictive variables. When applying this predictive variable in a Cox regression model, an actuarial plot was created to predict procedural complications based on procedural volume (Figure 2).
Actuarial procedural time versus the office-based procedural volume. Actuarial plot based on a Cox regression model analyzing probability of procedural complication versus office-based procedural volume. Procedures performed in office-based endovascular suite. Comparison of technical success, procedural variables, and complications among five patient groups. p < 0.05 when compared to group I.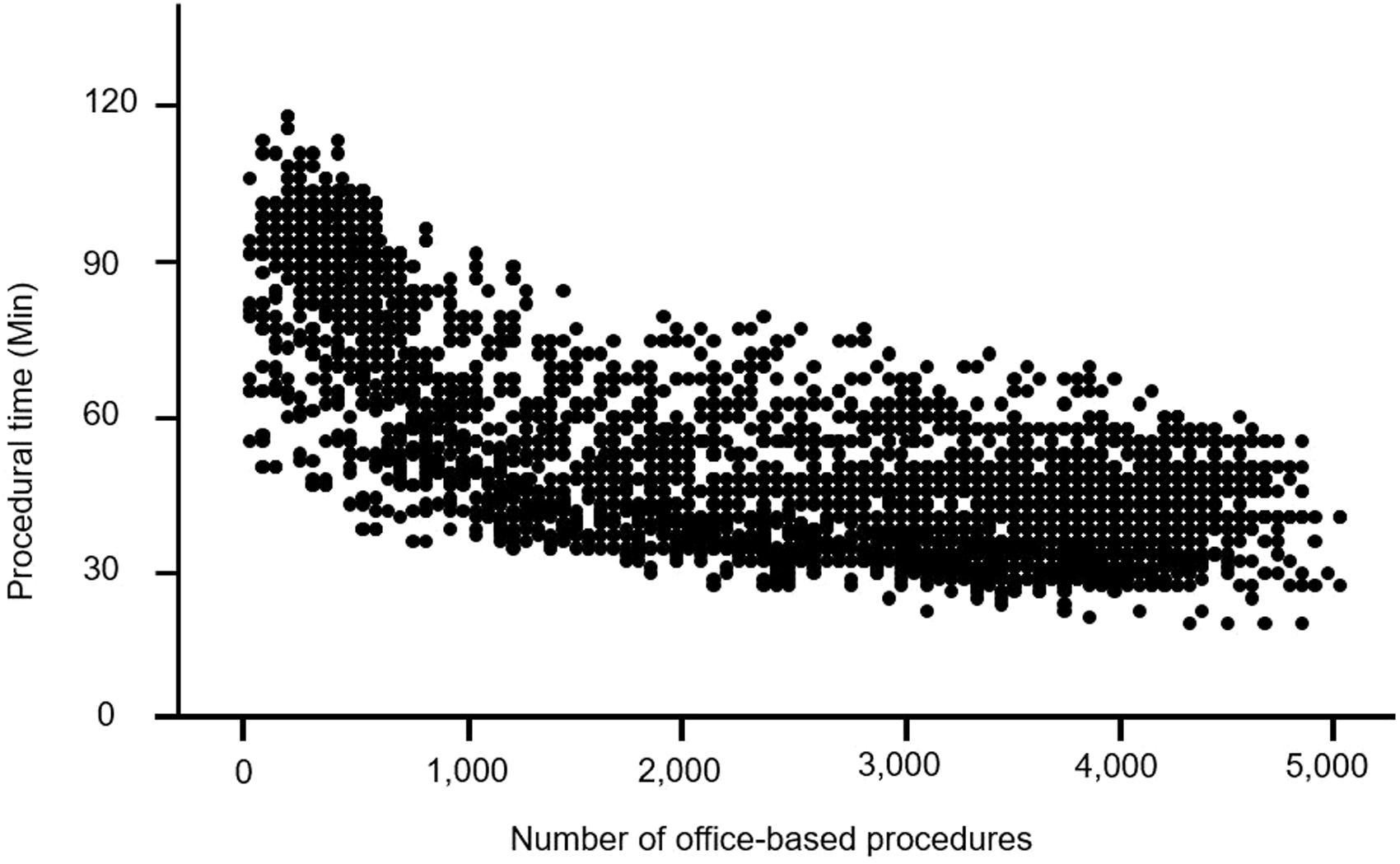
In 5085 (99.3%) of the cases, patients were discharged home from the recovery room without any inpatient management. Nine patients (0.18%) died within the 30-day period following their procedures. However, none of the deaths were procedure related. Six patients (0.12%) were dialysis-dependent and died of cardiac arrest during, and just after hemodialysis. Three of the deaths were related to respiratory issues; one patient died of secondary pneumonia which resulted from congestive heart failure and one patient who had underlying chronic obstructive pulmonary disease died of respiratory failure.
Discussion
The number of office-based endovascular labs in the United States has increased significantly since 2008 when the Centers for Medicare & Medicaid Services modified reimbursement rates to encourage more efficient outpatient use of peripheral vascular intervention. 5 This has caused a paradigm shift in many physicians' practices in that elective endovascular procedures which were traditionally performed in a hospital are now being performed in an office-based facility. Supporters for this outpatient clinical practice highlight many perceived benefits including improved patient satisfaction with expeditious outpatient experience, reduced financial burden in patient cost compared to hospital charges, convenience in managing case schedule in physician's own facilities, and favorable procedural reimbursement in an office-based practice. However, many critics have raised concerns regarding the safety and standard of patient care in this outpatient healthcare model. Our study is notable because it examines the treatment outcome of a large patient cohort who were treated in office-based endovascular facilities. Importantly, we discussed various lessons we learned from this large patient experience in an effort to improve patient safety and optimize patient care.
Many physicians have reported their experiences in office-based endovascular interventions with widely varied complication rates which ranged from 0.1% to 16%.6–12 The overall complication rate in our series was 1.4% which was remarkable and well within the range compared to published reports.6–12 Kruse and Cragg 10 analyzed 239 arterial interventions in their outpatient practice and noted a complication rate of 8% in those who had a postprocedural observation period of less than 4 hr. In contrast, their patients who required greater than 4 hr of postprocedural observation had a significantly higher complication rate of 24.3%, predominantly due to minor hematoma. Since no groin closure device was used in their study, their patients' puncture site bleeding was managed with manual compression. Struk et al. 12 conducted a comparative study of 141 outpatient peripheral arterial procedures and 84 inpatient arterial interventions during a 4-year period. The authors reported fewer complications of 5% in outpatient procedures in contrast to an inpatient procedural complication rate of 8.3%. Gradinscak et al. 7 reported a prospective analysis of 2683 procedures performed on an outpatient basis during a 5-year period, and noted an overall complication rate of 23%. Although the authors included minor complications such as local pain or puncture site bruising, they reported a major complication rate of 3.6% including hematoma that required surgical decompression. Jain et al. 8 recently reported a large series of 6458 outpatient procedures in 2822 patients during a 5-year period and described an overall complication rate of 0.8%. Specific complication rates in venous interventions, diagnostic aortogram without interventions, peripheral arterial interventions, dialysis related fistulogram were 2.2%, 1%, 2.7%, and 0.5%, respectively. 8 The widely varied complication rates from these reports could in part be explained by the lack of uniform reporting standards and inconsistent definitions of procedural-related complications. Furthermore, these clinical series contained varying proportions of arterial and venous interventions. Since the majority of procedural complications are related to arterial access issues such as major hemorrhage, pseudoaneurysm, or hematoma, clinical reports with high volumes of arterial interventions typically had greater complications in contrast to those office-based practices with predominately venous procedures.
While many clinical reports have demonstrated that office-based endovascular interventions can be performed safely with good outcomes,6–12 we believe routine use of percutaneous closure devices with established protocols in arterial intervention is an essential component to ensure optimal treatment outcomes. In our practice, a treatment algorithm was developed that all punctures were performed under ultrasound guidance. A sheath contrast angiogram of the puncture site was performed prior to closure device insertion. If a closure device failed, a second device would be used. If this device failed then prolonged manual compression or Femostop® was applied. In our study, a definite procedural-related learning curve was observed, which was evidenced by the reduced procedural time and contrast volume as our endovascular volume increased. Additionally, procedural related complications similarly declined in the latter four groups in contrast to group I patient cohort. The sharp contrast in the procedural time between the early and recent patient groups underscored the importance of the operator's experience and may be partly responsible for the declined complication rates. As illustrated in Figure 2, the probability of procedural complications decreases as endovascular volumes increase. Several other reports have similarly underscored the importance of percutaneous closure device in reducing puncture-site related complications, improved patient postprocedure discomfort, and early outpatient discharge to home.13–16
Another important lesson which we learned to ensure optimal health care delivery in an office-based lab is organizational accreditation. A recent New York Time article brought forth a public health concern regarding the possibility of overuse or inappropriate care in office-based vascular interventions. 17 Unlike procedures being performed in hospitals or ambulatory surgical centers, currently there is no consistent oversight for office-based endovascular procedures. There is also no established review process of treatment indications or outcomes following these interventions. Similarly, there is no required licensing to assure the safety and qualities of these office-based endovascular interventions. Although accreditation for office-based lab is not uniformly mandated by all states, currently nearly 30 states require accreditation for ambulatory surgical procedures. We believe there are definite benefits with obtaining accreditation in office-based practices. Accreditation introduces an objective third party to monitor, validate the activities of an office-based practice, and provide a national acknowledgement of quality. This level of standardization provides confidence that the office-based surgery center has the same level of safety as that of hospitals or ambulatory surgical centers. Recognition in the healthcare industry among other office-based facilities is another compelling benefit to seek accreditation. Patients, insurance carriers, and even physicians employed by the office practice may have a better perception of a center with accreditation because the practice will have met a higher standard of care, or at least that equal to hospitals and ambulatory surgical centers. Additionally, accreditation validates all aspects of an office-based endovascular lab: administrative, clinical, and surgical. The administrative points include facility and equipment maintenance, medical records documentation, and credentialing of personnel. Clinical considerations include patient rights management, approval of procedures in the office, and nursing services. Surgical issues include preoperative testing requirements, medication administration, and risk management.11,18
In our office-based facilities, we received accreditation through the Accreditation Association for Ambulatory Health Care (AAAHC), which is a nationally recognized accrediting organization that governs ambulatory facilities. There are two other organizations which provide accreditation services for outpatient facilities, which are the Joint Commission and Accreditation Association for Ambulatory Health Care (AAAHC). These accreditation agencies generally focus on structure and process variables. The main objectives of the accreditation process is to ensure that accredited outpatient facilities have an organizational structure and governance that provides proper oversight, sufficient facilities and equipment, appropriately trained providers, and established policies and procedures to ensure safe and high-quality patient care. More recently, these accreditation organizations are also seeking evidence of high-quality patient outcomes through requirements for benchmarking and ongoing quality improvement activities. In addition to the aforementioned accreditation organizations, several professional society-based accreditation programs have also been established for more focused areas in cardiovascular systems. The American College of Cardiology has six programs in diagnostic and interventional cardiac and vascular procedures. 19 Similarly, the American College of Radiology has accreditation programs in nine areas of imaging. 20 Other organizations have specifically been created to provide accreditation in areas such as chest pain and heart failure. 21 Similar accreditation specifically for ambulatory or office-based venous centers was recently established. 22 Regardless of the accreditation agency, we believe facility accreditation by these nationally recognized or society-sponsored organizations is essential in providing quality patient care in office-based endovascular practices.
There are undoubtedly several weaknesses in our study. The lack of reporting standards in outpatient vascular interventions represents a definite limitation in accurately comparing our results with other published reports. Since patients chosen for outpatient endovascular interventions in our practice are based on an inclusive criteria, this creates an inevitable selection bias such that our treatment outcomes may differ from comparative hospital-based treatment results. Additionally, the heterogeneity of patient populations in our office-based practice which included both arterial and venous interventions further compound the complexity of outcome analysis with regard to complication rates and procedural learning curve. Taken altogether, we believe our study is important as it highlights valuable lessons learned in establishing a large volume office-based endovascular practice.
In conclusion, enthusiasm for office-based interventional procedures will continue to grow in the future because of benefits including expeditious perioperative patient experience and favorable physician reimbursement schedule. Our study, along with other reported experiences, have demonstrated that office-based vascular interventions can be performed safely with remarkable outcomes. Diligent efforts to not only reduce complications but also maintain quality of care are paramount in the continual success of this office-based practice. Our experience demonstrated a procedural related learning curve with office-based vascular interventions, which can certainly be overcome. We believe routine use of percutaneous closure device is beneficial in reducing access related complications. Additionally, facility accreditation of an office-based practice is a cornerstone of providing high quality of care and ensuring appropriate organizational oversight in ambulatory treatment outcomes. Further efforts from professional societies and regulatory agencies to provide appropriate benchmarks for healthcare delivery in office-based facilities will undoubtedly lead to both reduced adverse events and enhanced treatment outcomes.
Footnotes
Acknowledgments
This work was presented at the Annual Meeting of Society of Vascular Surgery in June 2012 in Washington, DC.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.