
Abstract
Survivors of ischemic stroke are still at a significant risk for recurrence. Antiplatelet agents are the treatment of first choice for long-term secondary prevention of vascular events. This study aims to assess a health promotion program on medication adherence to antiplatelet therapy among ischemic stroke patients in Hainan province, China. In five hospitals from the intervention group, four highly experienced physicians trained 62 neurologists, who in turn trained 613 stroke patients to improve their awareness and adherence to antiplatelet therapy. Physicians and patients of the control group received usual stroke management programs. After one-year follow-up, the proportion of patients who took the antiplatelet therapy increased significantly in the intervention group, reaching 73.2%, with a pre–post difference between two arms of 22.9% (P < 0.01). There was also a significant net increase in the proportion of patients with awareness of antiplatelet therapy (24.4%, P < 0.01). Multivariate analysis illustrated health promotion program, higher education, annual household income, insurance, and medical status affected antiplatelet drug use in stroke patients. In conclusion, the health promotion program, based on a train-the-trainer approach, showed positive effects on awareness of and adherence to antiplatelet therapy, which has the potential to be scaled up to other resource-limited areas.
Introduction
Stroke is a noncommunicable disease of increasing socioeconomic importance in aging populations. According to the Global Burden of Diseases in 2013, it was the second leading cause of mortality and the third leading cause of disability-adjusted life years lost globally. 1 A systematic review has synthesized 56 population-based studies found a divergent, statistically significant trend in stroke incidence rates over the past four decades, with a 42% decrease in stroke incidence in high-income countries and a greater than 100% increase in stroke incidence in low- and middle-income countries (LMICs). 2 In China, the prevalence of stroke has been rising with the rapid socioeconomic growth and lifestyle changes. With 1.4 billion populations, the annual stroke mortality rate is approximately 1.6 million, or 157 per 100,000, which has exceeded heart disease to become the leading cause of death and adult disability. 3
Recent epidemiological data suggest that patients who have suffered from an ischemic stroke are at high risk of recurrent ischemic events, approximately one-third of stroke survivors will have a recurrent vascular event within five years. 4 Antiplatelet agents including aspirin, clopidogrel, and dipyridamole are the treatment of first choice for long-term secondary prevention of vascular events in patients with confirmed ischemic stroke.5,6 In a prespecified meta-analysis of the Chinese Acute Stroke Trial and the International Stroke Trial data, early aspirin intake produced a reduction of seven per 1000 of fatal or nonfatal recurrent ischemic stroke and a reduction of nine per 1000 of further stroke or death. 7 Moreover, a modest clinical benefit of clopidogrel over aspirin has been demonstrated in the CAPRIE trial. 8 However, for the vulnerable population of stroke patients residing in poorly resourced areas, secondary prevention and rehabilitation are largely unavailable, and where present, are far below evidence-based standards.
Train-the-trainer programs are used in a wide variety of fields for workforce development, including healthcare issues, public health preparedness, occupational safety, nutritional education, and a variety of clinical interventions. A benefit to this model is its ability to train a high volume of trainers in a relatively short amount of time. 9 The participants are often already working directly with the target group and are in a prime position to carry out the intervention once trained. Building capacity at the local level also has the potential for enhancing collaboration and networking among those trained and for sustaining the training.
In this study, we aimed to assess the effects of a health promotion program, based on a train-the-trainer approach, on adherence to antiplatelet therapy among ischemic stroke patients in Hainan Province, China.
Methods
Study sites
A controlled multicenter trial with a one-year follow-up was conducted between January 2011 and March 2015 in 10 general hospitals that were distributed throughout the whole Hainan province, China. Chinese hospitals are classified as tier-1 (township hospital that contains less than 100 beds), tier-2 (affiliated with a medium-size city, county, or district and contain more than 100 beds, but less than 500), and tier-3 (comprehensive or general hospitals at the city, provincial, or national level with a bed capacity exceeding 500). Among these 10 hospitals, Hainan Provincial Nongken Hospital, Hainan Provincial People’s Hospital, Hainan Province Nongken Sanya Hospital, Sanya People’s Hospital, and Qionghai People’s Hospital are tier-3 hospitals, while the other five hospitals (Hainan Cadre Sanatorium, Hainan Second People’s Hospital, Nada Nongken Hospital, Wanning People’s Hospital, and Lingao People’s Hospital) are tier-2 hospitals.
Written informed consent was obtained from all physicians and patients or an appropriate family member (in situations in which the patient was disabled). This research was approved by the ethics committees of 10 hospitals. Good clinical practice guidelines in accordance with the Declaration of Helsinki were used and the privacy of patients was strictly protected.
Patient population
Consecutive patients age ≥18 with a confirmed diagnosis of nonfatal ischemic stroke were enrolled. All patients included in this study underwent CT or MRI. Patients were excluded if they suffered from (1) cerebral hemorrhage; (2) venous system infarction; (3) stroke caused by brain tumors, brain injury, or hematological disease; and (4) any serious or life-threatening diseases such as heart, lung, liver, or kidney failure, hematological diseases, or malignant tumors.
Randomization
Patients were randomly allocated to intervention or control groups stratified by hospital. Two tier-3 hospitals (Hainan Provincial Nongken Hospital and Hainan Provincial People’s Hospital) and three tier-2 hospitals (Hainan Cadre Sanatorium, Nada Nongken Hospital, and Wanning People’s Hospital) were replaced to intervention group, while the other five hospitals were allocated to control group.
In the intervention group, 62 physicians (at least 10 from each hospital) involved in the management of stroke patients were trained by four highly experienced physicians in a one-day workshop as “health coaches” to offer the health promotion program at their own working settings. To support the implementation of the health promotion program, the study team provided continuous supervision for the health coaches. The workshop and the supervision, based on the Chinese Guidelines for the Secondary Prevention of Ischemic Stroke and Transient Attack 2010, 10 focused on the secondary prevention of ischemic stroke, including adherence to medication especially antiplatelet therapy, risk identification, management of low mood, etc. Then, patients recruited in this study were trained by the trained physicians and guided by a culturally appropriate and easy-to-understand secondary prevention manual before hospital discharge. The training sessions took about 30 min per day for three days, with the intention of developing patients’ awareness and improving their adherence to medications. The physicians called the patients at one, three, and six months after hospital discharge to monitor progress and offer guidance on secondary prevention. After one year discharge, the patients were asked to return hospitals to receive a follow-up investigation; telephone interviews were performed for patients unwilling or unable to return to hospitals.
Physicians and patients of the control group participated received usual stroke management programs without additional health promotion program.
Data collection
A self-designed questionnaire with a centesimal system was approved by experts in stroke prevention and rehabilitation. It was used prior- and post-training to ascertain physicians’ knowledge and ability to train stroke patients. Standardized baseline assessments for all patients included their (1) sociodemographic factors: age, gender, residence (city or rural areas), education (primary school and below, or junior high school and above), marital status (married or single), working condition (currently employed and retired, or unemployed); (2) financial situation: annual household income (≥15,500 or <15,500 CNY) and whether own insurance (yes or not); (3) hospital characteristics: hospital level (tier-3 or tier-2); (4) medical history: hypertension (yes or no), diabetes (yes or no), cardiac disease (yes or no), hyperlipidemia (yes or no), smoking (yes or no), and drinking (yes or no); (5) clinical status: severe stroke (modified Rankin Scale ≥ 3, yes or no). Prior to the training and after one year discharge, patients’ awareness and adherence to antiplatelet medication were surveyed.
Outcomes
The primary endpoint to assess the effect of the health promotion program was net difference between intervention and control groups in the adherence to antiplatelet therapy. Secondary outcome was the net differences between two arms in the awareness of antiplatelet medication.
Power analysis
Based on a sample of 1100 patients in 10 hospitals (five intervention and five control hospitals), assuming an intracluster correlation coefficient of 0.02, this study will have >90% power (with two-sided alpha of 0.05) to detect a 20% net difference in the primary outcome. 11
Statistical analysis
The distribution of all continuous variables that follow a normal Gaussian distribution was presented as mean ± SD. All categorical variables were summarized and expressed as proportions. Comparisons of the intervention and control groups were carried out using the Mann–Whitney U test for continuous data and Pearson’s chi-square test for categorical data.
Logistic regression analysis was performed to determine associations between compliance with antiplatelet therapy and each variable of interest. Univariate analyses were carried out first. Factors that were significant at the p < 0.20 level in the univariate models were put into the multiple logistic regression models. Then, the importance of each variable included in the model was evaluated with an examination of the Wald statistic for each variable in this model and a comparison of each estimated regression coefficient in the multivariate model with the regression coefficient from the corresponding univariate model. Variables that did not make significant contributions to the models on the basis of these two criteria were deleted in a stage-wise manner, and a new model was fitted. This process of eliminating, refitting, and verifying continued until all of the variables included were statistically significant, yielding a final model.
All significance tests were two-sided and a P value < 0.05 will be considered statistically significant. All statistical analyses were performed using SAS software, version 9.4 (SAS Institute, Cary, NC, USA).
Results
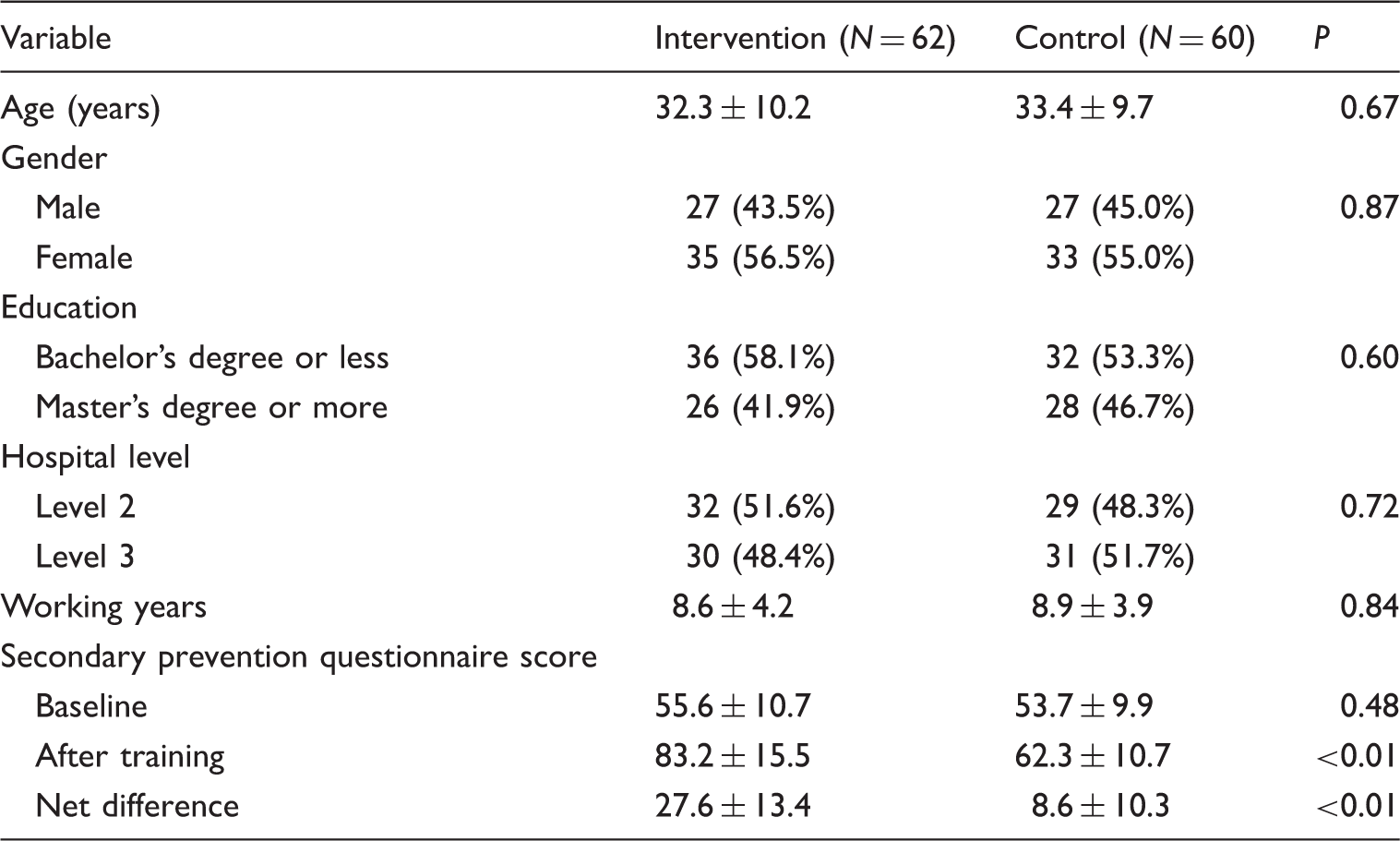
Demographic characteristics of trained physicians (N = 122).
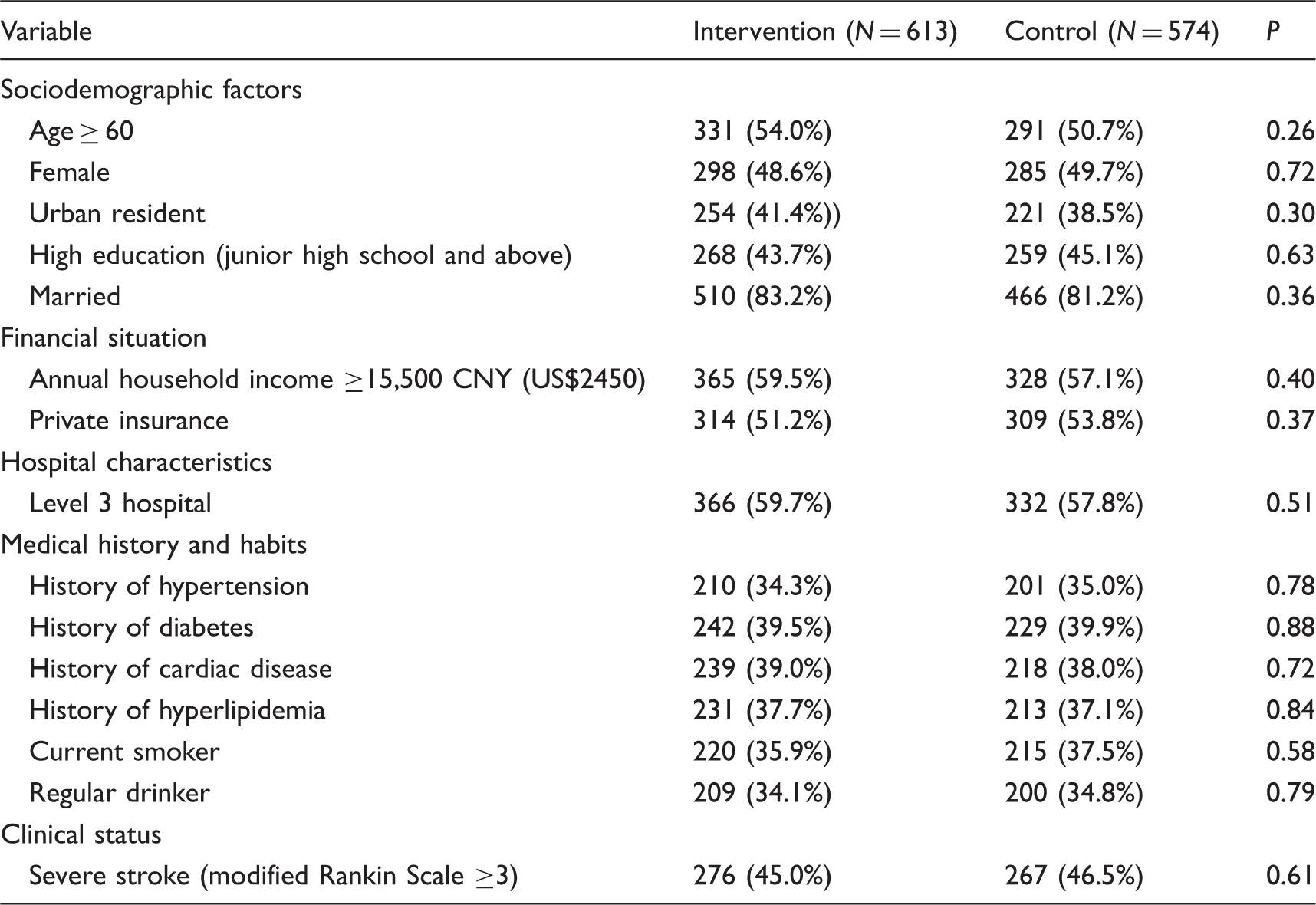
Demographic characteristics of ischemic stroke patients (N = 1187).
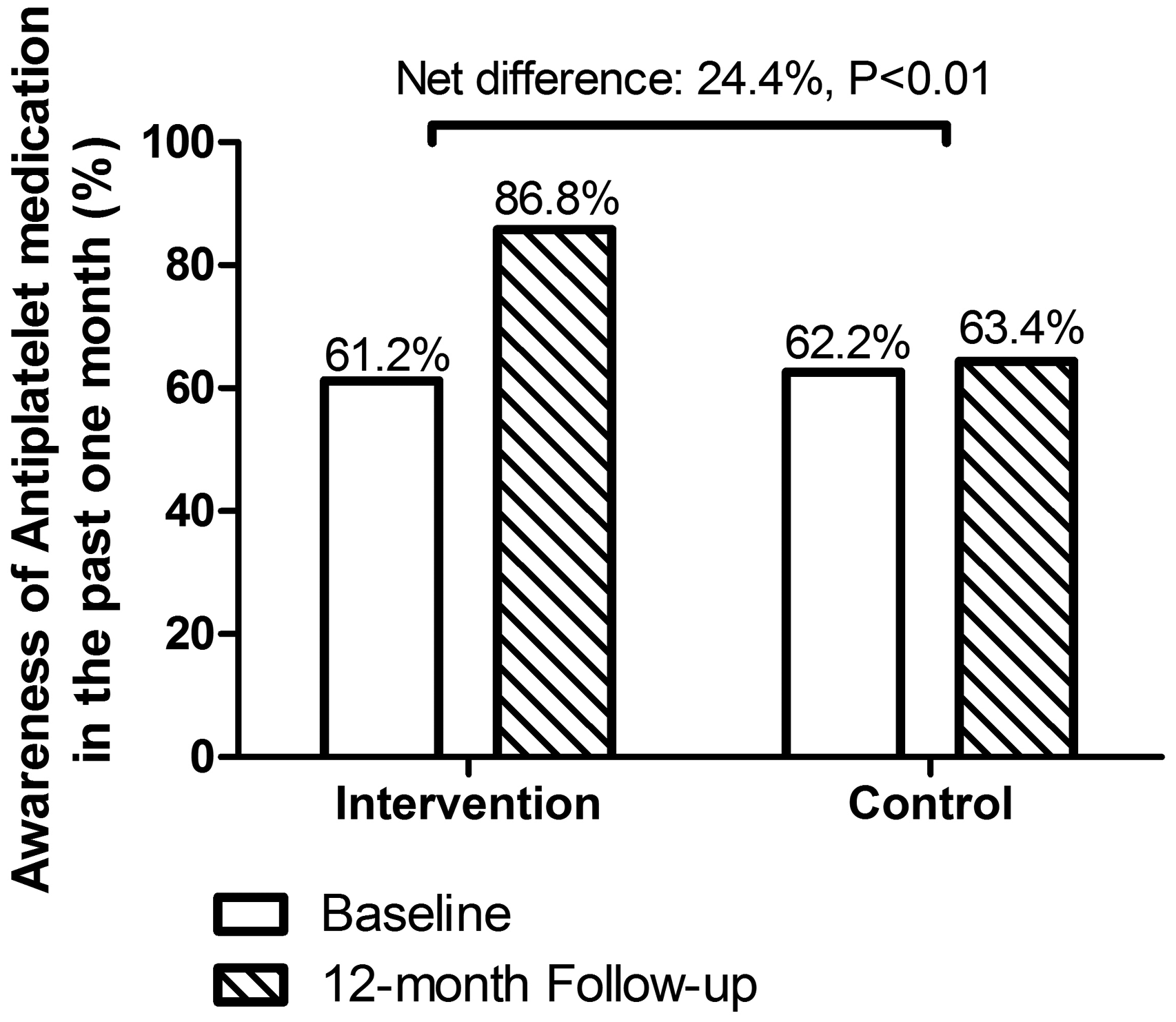
Prior to intervention, the use of antiplatelet medication was low in both groups (Figure 1). After one-year follow-up, the proportion increased significantly in the intervention group, reaching 73.2%, with a pre–post difference between two arms of 22.9% (P < 0.01). Among these 773 patients taking the antiplatelet medication, 707 (91.5%), 42 (5.4%), and 24 (3.1%) took aspirin, clopidogrel, and dipyridamole, respectively. Similarly, there was a significant net increase in the proportion of patients with awareness of antiplatelet therapy in the intervention group (24.4%, P < 0.01; Figure 2).
Effect of the health promotion program on the adherence to antiplatelet therapy among stroke patients. *P value for the net difference of preintervention and after one-year follow-up between the groups. Effect of the health promotion program on the awareness of antiplatelet therapy among stroke patients. *P value for the net difference of preintervention and after one-year follow-up between the groups.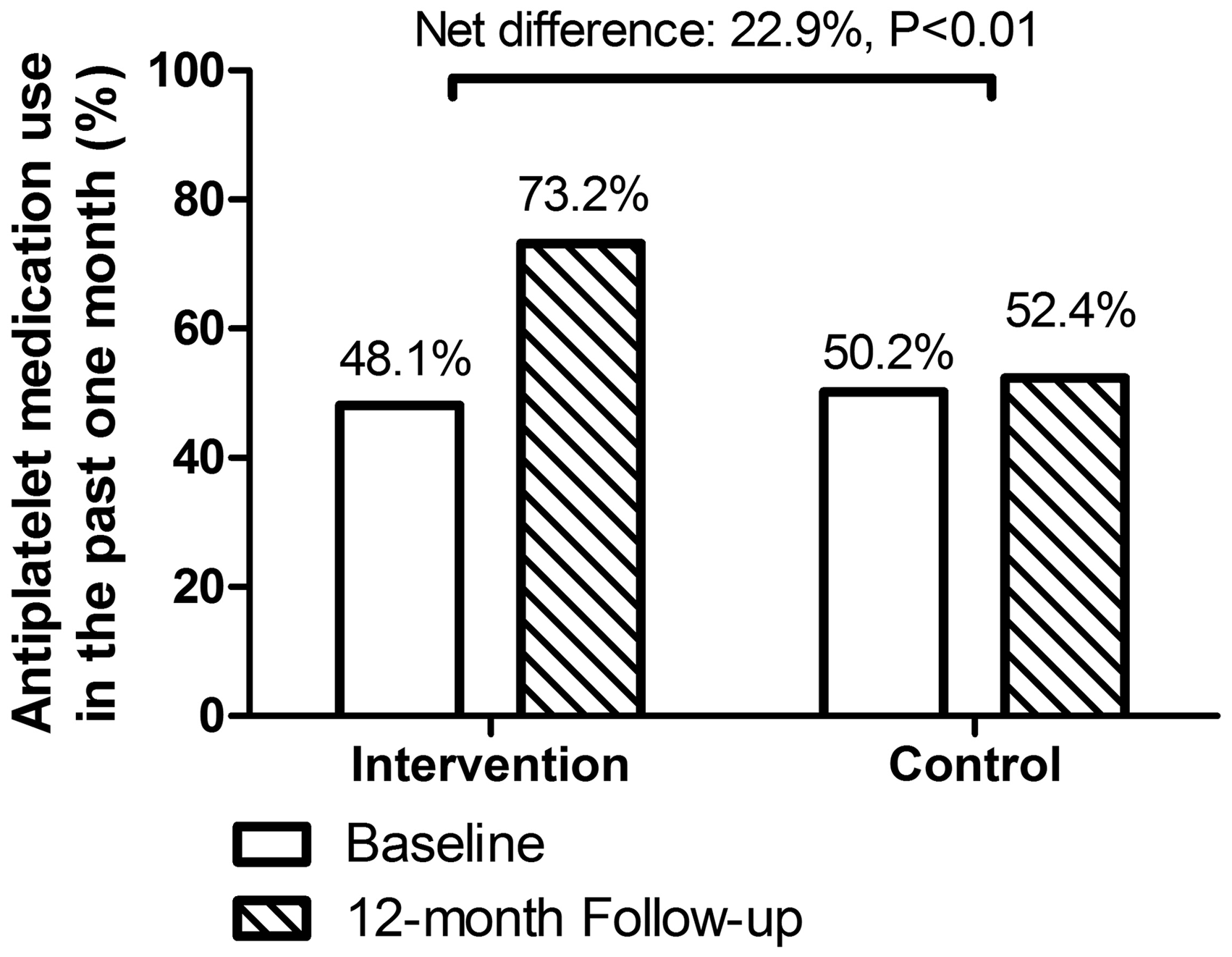
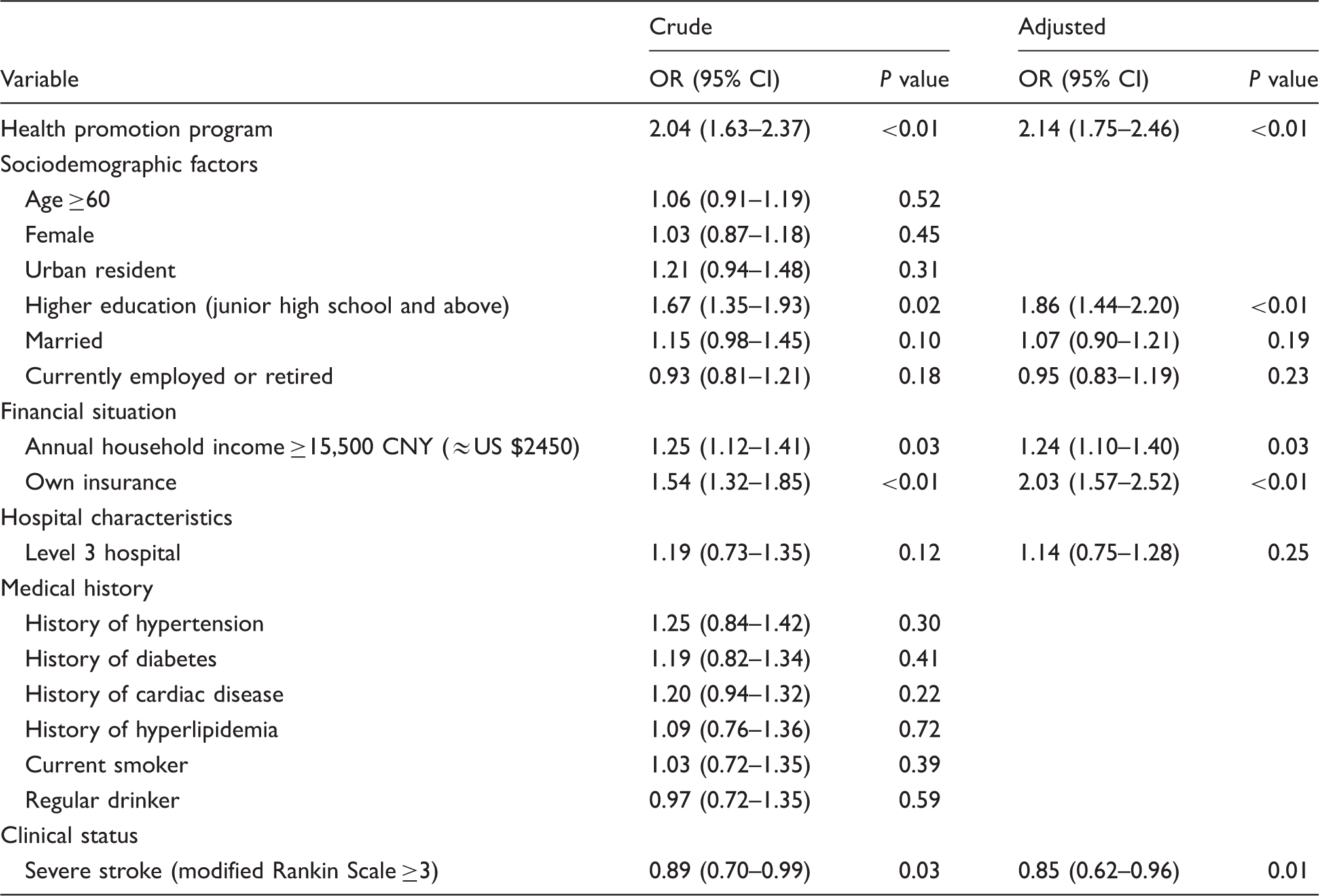
Factors associated with use of antiplatelet therapy in patients.
Discussion
Many regions in LMICs are characterized by the rapidly rising burden of noncommunicable chronic diseases and the serious lack of economic and healthcare resources coupled with a weak healthcare system.12,13 Despite well-established national guidelines on stroke prevention and management, its uptake into routine clinical practice remains limited. As a remote economically backward province with poor healthcare facility, the antiplatelet treatment rate among stroke patients in Hainan is only 49.2%, much lower than that in the China mainland (81.0%). A cost-effective, feasible, and culturally tailored approach is urgently needed.
Our prospective randomized controlled trial has demonstrated the effectiveness of a train-the-trainer method in enhancing the physicians’ capacity and improving the patients’ awareness and adherence to antiplatelet medication in 10 general hospitals throughout Hainan province, China. The train-the-trainer model has been frequently used in business, education, and interventions, to disseminate knowledge and skills. For instance, this model has been moderately successful in disseminating disaster mental health training in New York after the terrorist attacks on 11 September 2001. 14 A German health promotion program based on a train-the-trainer approach showed positive effects on health-related quality of life and mental health, especially anxiety, of long-term unemployed persons, a highly burdened target group where an improvement in mental health is a crucial prerequisite to social participation and successful reintegration into the job market. 15 In a cluster-randomized, controlled trial using a simplified multifaceted management program for individuals at high cardiovascular risk (SimCard Trial) conducted in China and Indian, village doctors received health professional training and aimed by the smartphone-based electronic decision support system to prescribe appropriate medication and lifestyle counseling during the monthly follow-up. The results indicated that this innovative intervention could improve quality of primary care and clinical outcomes in resource-limited settings. 16
The longitudinal changes observed in the intervention group of our study sample must be considered a particular success of the health promotion program evaluated here since, first, the stroke patients have often been described as reluctant to change and, second, dramatically improvement of awareness of and adherence to medication in behavioral research are often generated under laboratory conditions rather than in welfare settings. The fact that the health promotion program analyzed in our study showed such promising results among stroke patients can, in our view, be explained by the participatory focus in the development of the program (involving both the health coaches at the settings and the stroke patients) and the continuous supervision and support offered to the patients throughout the duration of the program. These aspects of the program design ensured a high degree of empowerment not only at the level of the participants but also among the professionals in charge of implementing the program in the settings.
Some sociodemographic factors or financial status were also related to the secondary prevention compliance of ischemic stroke. Patients with higher education might possess more preventive knowledge on this disease. Financial difficulty cannot be overlooked as the average income level of Hainan residents is lower even than in mainland China. Medical insurance could reduce patients’ economic concerns, thereby improving compliance with antiplatelet therapy. It is interesting to note that patients who had suffered a severe stroke were less likely to receive therapy, possibly because they would choose more conservative management. All these risk factors are similar with the results from previous studies.11,17
A few limitations of the current evaluation deserve note. First, the data collected are self-reported, measuring respondents’ perceptions of learning and impacts. It is possible that participants over- or underrated their skills and knowledge when responding to survey items. In addition, the short-term follow-up cannot be enough to assess whether this health promotion program could decrease the recurrence of stroke. Further larger, well-designed clinical trial is needed to address these problems.
In conclusion, our research demonstrated that this feasible and applicable health promotion program not only enhanced the patients’ awareness of secondary prevention, improved medication adherence to antiplatelet therapy, but also built up the physician’s skills and healthcare capacity of local health system. This evidence-based train-the-trainer model has potential to be scaled up to other resource-limited areas in China and around the world.
Footnotes
Authors’ contribution
Qingjie Su, Chaoyun Li, Faqing Long, Bin Chen, and Zhongqin Wan contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Major Program of Hainan Ministry of Science and Technology (Grant Number ZDXM20130068) and the Key Research Project of Hainan Ministry of Health (Grant Number Qiong Health 2010-40).