
Abstract
As a common etiology for ischemic stroke, atherosclerotic carotid stenosis has been targeted by vascular surgery since 1950s. Compared with carotid endarterectomy, carotid angioplasty and stenting (CAS) is almost similarly efficacious and less invasive. These advantages make CAS an alternative in treating carotid stenosis. However, accumulative evidences suggested that the long-term benefit-risk ratio of CAS may be decreased or even neutralized by the complications related to in-stent restenosis (ISR). Therefore, investigating the mechanisms and identifying the influential factors of ISR are of vital importance for improving the long-term outcomes of CAS. As responses to intrinsic and extrinsic injuries, intimal hyperplasia and vascular smooth muscle cell proliferation have been regarded as the principle mechanisms for ISR development. Due to the lack of consensus-based definition and consistent follow-up protocol, the reported incidences of ISR after CAS varied widely among studies. These variations made the inter-study comparisons of ISR largely illogical. To eliminate restenosis after CAS, both surgery and endovascular procedures have been attempted with promising results. For preventing ISR, drug-eluting stents and antiplatelets have been proposed as potential solutions.
Keywords
Introduction
Due to the unique geometric profiles and the corresponding hemodynamic changes, carotid bifurcations and adjacent segments are predisposed for atherosclerosis. 1 Occlusive injuries in carotid bifurcations are responsible for 7–20% of all ischemic stroke cases.2,3 Carotid endarterectomy (CEA) and carotid angioplasty and stenting (CAS) are two main treatment strategies for stenoses in this regions. Although CAS is no more efficacious than CEA in preventing subsequent stroke, 4 and CEA remains the gold standard for treating symptomatic carotid stenosis, 5 less invasiveness make CAS a preferred alternative in some selected cases. CAS has other advantages over CEA, such as decreased patient discomfort and shorter hospitalization. 6 CAS is usually recommended to patients with high risk for surgery, radiation-induced stenosis, or restenosis after CEA. 5 Since the publication of several large clinical trials, number of cases with CAS has been increasing, while that with CEA has been decreasing.7,8
There have been two major concerns related to the safety and efficacy of CAS, the periprocedural risk of vascular events and the long-term risk of in-stent restenosis (ISR), since the very beginning of the clinical application of this novel treatment strategy. By using embolic protection devices (EPD) during CAS procedures, composite rate of periprocedural stroke or death can be limited to <6% or even lower in experienced hands and in centers with large patient volume, which is comparable to that in patients with CEA. 9 However, at least one large trial observed that new cerebral lesions detected by MRI diffusion-weighted imaging were more frequent in patients treated with filter-protected CAS than in patients with CEA. 10 Further studies, therefore, are warranted to ascertain the efficacy and safety of EPD. Accumulative evidences suggested that the benefit-risk ratio of CAS may be decreased or even neutralized by the increased risk of recurrent cerebrovascular events related to ISR.11–13 Here, we reviewed incidences and impacts, discussed mechanisms and potential risk factors of ISR. We also compared diagnostic methods and treatment choices for ISR after CAS.
Incidence of ISR after CAS
Incidence of restenosis after carotid artery stenting.
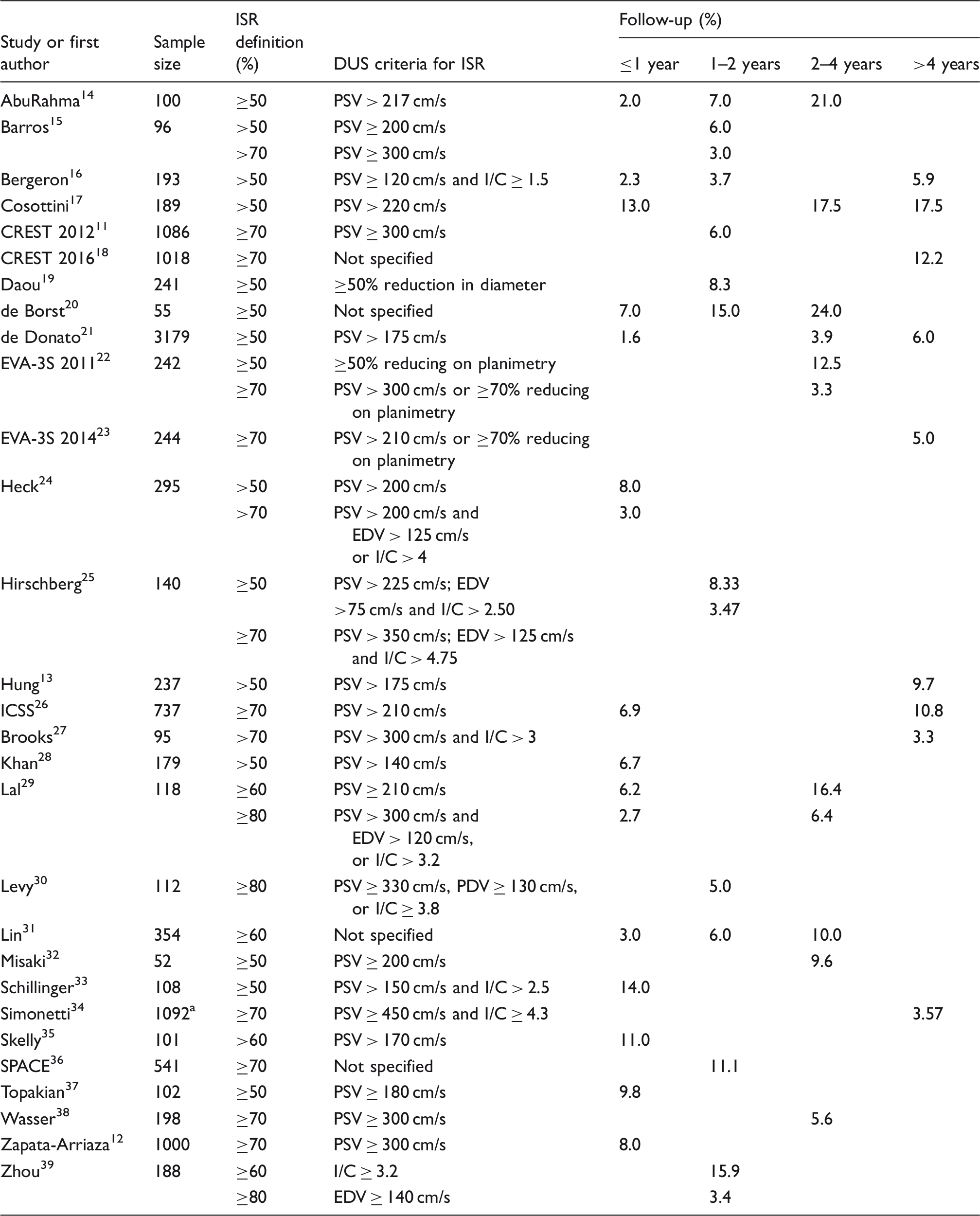
CREST: carotid revascularization endarterectomy versus stenting trial; CTA: computerized tomography angiography; DUS: duplex ultrasonography; EDV: end-diastolic velocity; EVA-3S: endarterectomy versus angioplasty in patients with symptomatic severe carotid stenosis trial; ICSS: international carotid stenting study; I/C: internal to common carotid artery peak systolic velocity ratio; ISR: in-stent restenosis; PDV: peak diastolic velocity; PSV: peak systolic velocity; SPACE: stent supported percutaneous angioplasty of the carotid artery versus endarterectomy trial.
Number of carotid artery stenting procedure.
Several multicenter, randomized clinical trials compared the safety and efficacy of CAS and CEA.11,18,22,26,36 Carotid Revascularization Endarterectomy versus Stenting Trial (CREST) involved heterogeneous patient population of both symptomatic and asymptomatic patients. 11 Duplex ultrasonography (DUS) was used to assess restenosis during follow-ups. DUS is a noninvasive and inexpensive examination with favorable reproducibility. Peak systolic velocity (PSV) measured with DUS was often used as a major parameter for detecting and rating ISR after CAS. For example, when a PSV ≥300 cm/s or no flow signal was detected with DUS in carotid artery, an ISR of ≥70% or occlusion was usually proposed. Based on this criterion, CREST reported a cumulative ISR incidence of 6.0% in 2 years after CAS. On these grounds, the authors concluded that the mid-term incidence of severe ISR after CAS was acceptably low. To compare the long-term safety and efficacy of CAS and CEA, investigators extend the follow-up of CREST patients to 10 years. The ISR was defined as either ipsilateral revascularization, ≥70% diameter-reducing stenosis, or occlusion. Based on this revised criterion, they reported a cumulative ISR incidence of 12.2% in 10 years after CAS. 18
In Endarterectomy versus Angioplasty in Patients with Symptomatic Severe Carotid Stenosis (EVA-3S) trial, restenosis of 50–69% was diagnosed with planimetry, whereas carotid restenosis of ≥70% or occlusion was diagnosed with either planimetry or a PSV ≥300 cm/s. The results showed that the 3-year cumulative incidence was 3.3% when ISR was defined as ≥70% stenosis or occlusion; while the 3-year cumulative incidence increased to 12.5% when ISR was defined as ≥50% stenosis or occlusion. 22 The EVA-3S investigators also extended the follow-up of some patients. 23 Carotid restenosis of ≥70% or occlusion was identified with either planimetry or a PSV ≥210 cm/s. The 10-year cumulative incidence of ISR was reported as 5.0%. However, direct comparison of incidences in the primary and follow-up studies may be inappropriate due to difference of patients and PSV value in these two studies.
International Carotid Stenting Study (ICSS), the largest trial of this kind to date, compared the efficacy of CEA and CAS in treating symptomatic carotid stenosis. 26 In this trial, ISR was defined as any residual or recurrent stenosis of ≥70% or occlusion and was detected as a PSV ≥210 cm/s. ICSS reported 1- and 5-year cumulative incidences of ISR as 6.9% and 10.8%, respectively.
In the Stent-Protected Angioplasty versus Carotid Endarterectomy (SPACE) study, ISR was also defined as ≥70% stenosis and identified by DUS without specific value. 36 The 2-year cumulative incidence of ISR was reported as 10.7% and 11.1% in intention-to-treat and per protocol estimates, respectively.
In above clinical trials, only patients with primary carotid artery stenosis were included. Besides de novo stenosis, other trials listed in Table 1 also included patients with recurrent stenosis after endarterectomy.13,14,16,17,19,28–31,34,35,38,39 Therefore, incidences of primary ISR might be overestimated in these studies.
Potential influencing factors for ISR
Many factors have been reported to influence the risk of ISR after CAS. The demographic characteristics associated with ISR included advanced age 28 and female gender.11,28 Khan et al. 28 showed that advanced age (>75 years, odds ratio (OR) = 1.107, 95% confidential interval (CI) = 1.020–1.202, p = 0.015) and female gender (OR = 3.519, 95% CI = 1.633–7.583, p = 0.001) were related to increased risk of >50% restenosis. In another trial, female patients were identified with greater risk for ≥70% restenosis than male patients (hazard ratio (HR) = 1.42, 95% CI = 0.84–2.39). 11
Several concomitant conditions have been associated with ISR. One single-center study observed that smoking (OR = 3.9, 95% CI = 1.6–8.7, p < 0.005) and diabetic mellitus (OR = 3.4, 95% CI = 1.4–7.9, p < 0.005) were significantly associated with ISR. 42 In CREST, diabetic mellitus (HR = 2.44, 95% CI = 1.46–4.08), dyslipidemia (HR = 5.12, 95% CI = 1.25–20.96), and hypertension (HR = 3.37, 95% CI = 1.05–10.76) were more prevalent in patients with ISR than in those without ISR. 11 Furthermore, hypertension (HR = 6.2, 95% CI = 1.9–19.9, p = 0.002), 12 peripheral vascular disease (HR = 1.92, 95% CI = 1.03–3.62, p = 0.041), 43 and contralateral carotid occlusion (OR = 10.11, 95% CI = 2.06–49.63, p = 0.004) 38 were identified as independent predictors for ≥70% restenosis in other trials. Recently, the history of cardiovascular disease (OR = 8.88, 95% CI = 4.4–17.6, p < 0.001) was reported as a predictor for ≥50% restenosis. 19
Characteristics and nature of the target lesion may also influence the ISR. Post-endarterectomy stenosis was identified as an independent predictor of ≥60% restenosis (OR = 3.98, 95% CI = 1.2–4.93, p = 0.02) on multivariate analysis. 31 In addition, recurrent stenosis after prior stent implantation (OR = 9.2, 95% CI = 1.6–53.2, p = 0.01) 33 and stenosis after radiotherapy (HR = 6.32, 95% CI = 3.00–13.3, p < 0.001) 13 were detected as independent predictors for ≥50% restenosis. A univariate analysis of outcome of 1000 carotid Wallstent implantations showed that symptomatic stenosis, de novo stenosis, and calcification (plaque type III/IV) were significantly associated with ISR. 42 Subsequent multivariable analysis identified calcification (plaque type III/IV) as an independent risk factor for ISR (OR = 36, 95% CI = 12.3–40.1, p < 0.001). The presence of calcified plaque was also significantly associated with ≥50% restenosis in another trial (p = 0.02). 44 Plaques longer than 20 mm were significantly related to ISR. 45 In the multivariate analysis, Misaki et al. 32 found that only the volumes of the plaque components with radiodensities <0 HU was associated independently with ≥50% restenosis (HR = 1.041, 95% CI = 1.006–1.078, p = 0.021).
Stent profile, residual stenosis immediately after CAS, post-stenting homodynamic status may influence the ISR. Multiple stent implantation was reported as an independent predictor for >50% restenosis in one study (OR = 5.2, 95% CI = 1.49–18.5, p = 0.0084) 17 and for ≥60% restenosis in another study (OR = 3.68, 95% CI = 1.4–5.36, p = 0.03). 31 Hung et al. 13 detected stent diameter (OR = 0.82, 95% CI = 0.71–0.95, p = 0.009) and pre-dilatation (HR = 2.03, 95% CI = 1.19–3.43, p = 0.008) as independent predictors for >50% restenosis. 13 ISR was more common in patients with an open-cell stent than in patients with a closed-cell stent. 41 The residual stenosis after CAS was a predictor of >50% restenosis (OR = 1.091, 95% CI = 1.050–1.130, p < 0.0001) in one trial. 17 In another study, residual stenosis of 10–30% after stent implantation (OR = 9.7, 95% CI = 1.6–59.3, p = 0.01) was an independent predictor of ≥50% restenosis. 33 In a third study, post-stenting residual stenosis >50% was significantly related to the ISR (p = 0.05). 45 Post-procedure carotid duplex ultrasound with a PSV ≥120 cm/s was identified as an independent predictor for ≥70% restenosis (OR = 6.33, 95% CI = 1.27–31.44, p = 0.024). 38 In a large cohort study, Cox regression analysis identified that pre-procedure impaired vasoreactivity was an independent risk predictor for >70% restenosis (HR = 1.7, 95% CI = 1.09–2.8, p = 0.019). 12
Some blood biochemical markers were also related to ISR. C-reactive protein levels at 48 h after CAS was an independent predictor of ≥50% restenosis (OR = 1.3, 95% CI = 1.1–1.6, p = 0.01). 33 Likewise, leukocyte count in 24 h after CAS as an inflammatory serum marker was also an independent predictor of ≥70% restenosis (OR = 1.31, 95% CI = 1.02–1.69, p = 0.036). 46 As markers for endothelium injury,47,48 serum VWF and ET-1 levels in the ISR group were higher in patients with ISR than those without non-ISR within 6 months after CAS. 49 In a cohort study, restenosis of ≥50% was significantly associated with lower high-density lipoprotein (HDL) cholesterol levels 1 month after CAS. 37 Multivariate logistic regression analyses identified HDL cholesterol >45 mg/dl as the only independent predictor of carotid stent patency at 1 year after the procedure (OR = 0.09, 95% CI = 0.01–0.83, p = 0.033).
The majority of these factors being associated with ISR were only observed in individual study. These varied results not only indicated the multifarious mechanisms of ISR, but also reflected the inconsistencies in ISR definitions, follow-up schemes, and ISR measurements used among studies. Further studies with uniformed ISR criteria and similar follow-up schemes are warranted to clarify this important issue.
Athero-Express study revealed that patients with transient ischemic attack (TIA) or stroke had a decreased risk of restenosis as compared to asymptomatic patients after CEA. 50 In another study, a higher prevalence of atherosclerotic carotid plaques with a large lipid core was observed in patients presenting with TIA or stroke. 51 The underlying mechanism may partly due to decreased inflammatory response and intimal hyperplasia in the operation area.
The reported risk factors for restenosis after CEA included female gender, 52 hyperlipidemia, 53 hypertension, 54 smoking, age <65 years, 55 carotid clamping time, 56 postoperative C-reactive protein, 57 metabolic syndrome, 58 highly calcified plaques, 59 homocysteine, 60 and severe renal insufficiency. 61 Among these factors, metabolic syndrome, homocysteine, and severe renal insufficiency have not been associated with restenosis after CAS. On the other hand, advanced age was associated with restenosis after CAS.
Possible mechanisms of ISR after CAS
As a vascular response to injury and implanted foreign materials, ISR is mainly attributed to neointimal hyperplasia and vascular remodeling during the early postoperative (e.g., within 2 years) and to recurrent atherosclerosis in later stage.62,63 Vascular smooth muscle cells (VSMCs) proliferation and migration were suggested as the main causes for neointimal hyperplasia after stent implantation. 64 The transition of VSMCs from contractile to synthetic phenotype is a prerequisite for the proliferation and migration of VSMCs. 65 Using a balloon-induced injury model in rat, Kang et al. 66 observed that expression of 44 proteins significantly changed within 3 days after artery injury, which was relevant to phenotypic changes. Among these proteins, oxidized LDL receptor-1 (OLR1) was suggested as a regulator for VSMCs hyperplasia. Furthermore, the OLR1 may play dual roles in the VSMCs hyperplasia by directly mediating oxidized LDL-induced monocyte adhesion via NF-κB activation and by improving activation of platelet-derived growth factor receptor (PDGFR). Studies also indicated that the adhesion and infiltration of monocytes to the stent-injured intima correlated with VSMCs proliferation, 67 and activation of PDGFR could induce VSMC migration and proliferation. 68 These results suggest that the OLR1 is a key molecule linking inflammatory responses to VSMCs proliferation and may play a vital role in neointimal hyperplasia. 66 Therefore, it is worthwhile to attempt OLR1 as a potential treatment target for preventing ISR.
In a case reported by Mazighi et al., 69 the CAS patient received 75 mg clopidogrel and 160 mg of aspirin daily after the procedure, but overt ISR was observed 3 months later. Laboratory testing indicated possible clopidogrel resistance. The angiography indicated that the ISR eliminated 1 day after the clopidogrel dosage being increased. Authors suggested that early ISR may be associated with increased platelet aggregation. In another case, a repeat CAS was performed in the patient with TIA 10 days after the initial CAS procedure. However, duplex ultrasound examination revealed progression of ISR 6 days after the second CAS procedure. The patient was then arranged with a surgery to remove the implanted stent. On biopsy, it was revealed that an atherosclerotic plaque prolapsed into the stent, which was deemed as the cause of the ISR. 70 It is known that pathogenesis of late ISR differs from early ISR (<6 weeks) which mainly results from stent misplacement or other periprocedural complications. In early stage, prolapsed atherosclerotic plaque may result in ISR and make endovascular techniques less advantageous.
Imaging detection of ISR
Several imaging examinations have been used to detect ISR, including DUS, computed tomography angiography (CTA), DSA, magnetic resonance angiography (MRA), intravascular ultrasound (IVUS), and optical coherence tomography (OCT). Due to different definitions (Table 1), the reported ISR vary widely among studies.22,29,71 Therefore, it is largely illogical to directly compare the reliability of these examinations in detecting ISR after CAS.
DUS
DUS has been demonstrated as a reliable tool for evaluating untreated carotid stenosis, and the results correlates very well with catheter-based angiography. 15 However, the biomechanical profiles of the carotid artery will be changed after the implantation of a stent, with elastic modulus increased and compliance decreased. 72 Furthermore, the types of stents may also influence the velocity measurement by DUS, and close-cell stents have been associated with relatively higher velocities as compared to open cell stents. 73 Therefore, the established DUS velocity criteria for evaluating stenosis in untreated carotids may be less feasible for detecting ISR after CAS. By introducing new parameters such as PSV, end-diastolic velocity (EDV), and internal to common carotid artery PSV ratio (I/C), several studies attempted new velocity criteria for detecting and grading ISR after CAS. In a 6-year follow-up study involved 6427 DUS examinations and 1123 angiographies, Setacci et al. 74 suggested that a PSV of 300 cm/s, EDV of 140 cm/s, and ICA/CCA of 3.8 were optimal cut-points for detecting ≥70% carotid restenosis after CAS. These cut-points have been used in other studies.11,12,38 However, biomechanical profiles of the carotid artery after CAS for primary stenosis may differ from that of stenosis after-CEA or radiotherapy. In the study by Setacci et al., 74 116 (14.25%) patients with CAS for restenosis of post-CEA were included, the recommend velocity criteria for grading primary ISR should be critically considered when interpreting the results. Although the good sensitivity, noninvasiveness, and low cost make DUS a favorable choice for detecting ISR after CAS, recorded velocity may vary remarkably among laboratories, which made the comparison of results from different centers problematic. DUS was also used for grading ISR after CAS, which may be helpful for determining whether a further endovascular or surgery intervention is indicated when an ISR was detected. 75
CTA
CTA is a noninvasive examination with high resolution and short acquisition time. Its reliability has been evidenced in detecting severe stenosis (≥70%) of untreated carotid, with a sensitivity of 100% and a specificity of 63%. The negative predictive value of CTA in detecting <70% carotid artery stenosis was 100%. 76 In several clinical trials, CTA was used to detect and to grade ISR after CAS. Kwon et al. 40 reported that CTA may overestimate ISR and had a lower sensitivity than DUS. In another study, ISR cases identified with DUS were further evaluated by a subsequent CTA. 15 The degrees of restenosis assessed by DUS were in good agreement with those by CTA. However, beam hardening from the metallic stent protrude a technical problem for CTA in evaluating ISR, which is expected to be solved by software upgrading in future.
DSA
DSA is currently the gold standard for evaluating occlusive carotid disease. It is capable to detect and grade ISR of different degrees. DSA is usually performed to determine whether a given ISR should be treated with aggressive interventions. As an invasive examination, however, DSA may introduce a neurological complication rate ranged from 1.3% to 2.63% in different patients.77,78 So this examination should be reserved to patients whose diagnosis cannot be determined with noninvasive methods and whose ISR was programmed for a possible surgery or endovascular treatment. 79
MRA
Considering the possible metal artifacts, MRA was once regarded as an inferior examination in evaluating ISR. However, Kono et al. recently reported that nonenhanced magnetic resonance angiography (NE-MRA) can visualize the lumen inside the carotid Wallstent (Boston Scientific, Natick, MA) 3 months after CAS. Using NE-MRA, ISR after CAS can be detected with a sensitivity of 100% and a specificity of 94%. 80 But these results have not been confirmed by other studies to date.
IVUS
IVUS is a direct and detailed examination in detecting arterial response to CAS. Clark et al. 81 performed IVUS in 50 carotids to detect ISR immediately and 6 months after the CAS procedures. Minimal luminal diameter, lumen area, stent area, and neointimal hyperplasia area were measured at multiple sites. The relative restenotic area at follow-up correlated negatively with post-procedural minimum stent area and stent expansion. Authors concluded that smaller stent dimensions immediately after the procedure were associated with increased risk of restenosis.
OCT
OCT is an optical analogue of IVUS that can obtain high-resolution (10 µm) tomographic intra-arterial imaging. 82 With the help of OCT, several studies investigated the in vivo histopathological changes of vascular intima after CAS. In one case report, OCT observed atheromatous changes at the in-stent neointima and slow progressive ISR within 10 years after CAS. Author suggested that novel atherosclerosis may play an important role in the development of late ISR. 83 In a retrospective study, OCT was performed before and after CAS procedure in 26 patients, and qualified imaging was obtained in 20 patients. 84 These 20 patients were followed with DSA, and ISR was observed in 12 patients in 6 months after CAS procedures. Mal-apposed stent struts and ruptured fibrous cap observed immediately after CAS by OCT were not associated with ISR. However, plaques load (e.g., plaque longer than 20 mm) 45 and plaque calcification before CAS42,44 were associated with ISR. As a high-resolution imaging modality, OCT may be helpful in identifying influencing factors for ISR. The usefulness of this new technique in carotid artery warrant further study.
Generally, as invasive methods, DSA, IVUS, and OCT have higher accuracy than noninvasive methods such as DUS, CTA, and MRA. The reliability of noninvasive methods to diagnose and grade ISR might be decreased for secondary ISR because few studies distinguished the primary and secondary ISR.
Treatment of IRS after CAS
Although most ISR after CAS were asymptomatic, some restenosis may progress to total occlusion, and some may result in ischemic events.21,85 Currently, it is generally accepted that a symptomatic ≥50% restenosis would be treated. 3 But the criteria for treating asymptomatic restenosis largely remains controversial. 86 Considering the continuously increasing cases of CAS, it is necessary to investigate the treatment strategies for severe ISR. Some strategies for treating ISR have been applied widely in clinical settings, while others were still under investigation.
Medical treatment
Cilostazol is an antiplatelet drug with extra effects for dilating artery and inhibiting VSMCs proliferation.87–89 In a retrospective study with 97 CAS cases being followed for 12 months, patients on cilostazol were reported with significantly lower risk of ISR (0% vs. 15.7%, p = 0.03). 90 The Retrospective Study of In-Stent Restenosis after Carotid Artery Stenting (ReSISteR-CAS) study enrolled 553 patients with CAS, who had been followed for 30 months after CAS. 91 Cilostazol treatment was associated with lower incidences of ISR or target vessel revascularization (1.4% vs. 6.4%; log-rank, p = 0.006). A recent meta-analysis involving 1233 patients also indicated that cilostazol treatment was associated with a significantly lower ISR incidence after CAS during a mean follow-up of 20 months. 92 Authors concluded that cilostazol may decrease the ISR rates after CAS without affecting the risk of cardiovascular events and death, in both early and late settings.
In a recent clinical trial, 114 patients were randomized to argatroban and placebo treatments. 93 The rate of ISR in patients with argatroban was significantly lower during the 9 months follow-up. The authors suggested that intravenous administration of argatroban may be effective and safe for preventing restenosis after CAS. Other reported drugs for preventing ISR after CAS included vinpocetine 94 and statin, 95 but with undetermined efficacy.
Endovascular interventions
Severe ISR after CAS has been treated with different endovascular procedures, such as percutaneous transluminal angioplasty with regular balloon (PTA), cutting-balloon angioplasty (CB-PTA), repeat CAS, off-label use of a cardiac angioplasty balloon, and more recently, drug-eluting balloon (DEB) angioplasty and drug-eluting stents (DES). 96
Since DES has become the mainstay for treating coronary atherosclerotic disease, 97 using DES for treating ISR after CAS has been attempted. In a pilot study, one dug-eluting stent was implanted in a patient with a >70% ISR which was detected at 6 months of the initial CAS and then received suboptimal PTA. DUS did not observe further ISR during 1 year follow-up. 98 In another trial, recurrent restenosis was reported in seven patients with ISR after repeat PTA. Zotarolimus-eluting stents (ZES) were implanted completely within the original stent in five patients. 99 DUS did not observe further ISR during the 17-month follow-up. In other two patients with ISR, ZES was also implanted but protruded beyond the original stent, which resulted in stent deformation and kinking, and finally artery occlusion.
In addition to conventional DES, the efficacy of biofactor-eluted stent in treating ISR was also investigated. Stents coating with an integrin-binding cyclic Arg-Gly-Asp peptide (RGD) can inhibit neointimal hyperplasia by recruiting endothelial progenitor cells. 100 Simsekyilmaz et al. 101 observed that the biofunctionalization of star-PEG-coated nitinol-stents with RGD/CXCL1 can reduce in-stent neointima formation in mice.
In recent years, DEB has emerged as a new therapeutic alternative for ISR. In a pilot study, none of the seven patients with severe ISR (>80% stenosis) underwent angioplasty developed ISR in 13.7 months. 102 In a larger cohort, 51 patients underwent 63 balloon dilation (DEB or conventional balloon) for treating ISR. Lesions treated with DEB manifested a significantly lower incidence of restenosis than those treated with conventional balloon (9% vs. 50%) in 8 months after the remedy procedures. 103
According to a recent system review, the available evidence for ISR treatment is still limited owing to methodological heterogeneity. Although PTA is the common treatment for ISR, limited durability may result in recurrent ISR, leading to repeated interventions and cost implications. 96 Considering the limited sample size and methodological heterogeneity, there is no enough evidences to support the efficacy of DEBs in treating ISR.
Surgery
Severe ISR after CAS has been treated with surgery of different maneuvers, such as CEA with stent removal and carotid artery bypass with reversed saphenous vein interposition graft, with polytetrafluoroethylene interposition graft, and with an internal-to-external carotid artery interposition graft. In a large series of CEA with stent removal for ISR after carotid stenting, Reichmann et al. 104 reported that all 15 treated patients remained asymptomatic and without recurrent restenosis (≥50%) on duplex ultrasound imaging after a median follow-up of 21 months. Currently, CEA remains as the major surgical maneuver in treating ISR after CAS.
Gene therapy
Several studies investigated the effects of gene therapy on restenosis after stent implantation in animal models, with inhibiting VSMCs proliferation as the main target. Jing et al. designed a lentiviral vector, Lenti-SM22α-p27-EGFP. The contained SM22α promoter can inhibit VSMC proliferation by increasing p27kip1 expression. 105 In a rat carotid artery balloon injury model, 50 μl of PBS, Lenti-SM22α-EGFP, or Lenti-SM22α-p27-EGFP (2 × 109 TU/ml) were infused into the blood vessel, and incubated for 30 min after the balloon injury. Compared to the rats treated with PBS or Lenti-SM22alpha-EGFP, significantly lower intima/media (I/M) ratio and restenosis rate were observed in rats infected with Lenti-SM22α-p27, with no overt side effects observed. Lompre et al. constructed another vector with SERCA2a, an inhibitor of VSMC proliferation, being combined into an adenovirus. Using this recombined vector can decrease the neointimal hyperplasia after balloon injury in rat model. 106 Concerning gene therapy, only some explorative studies was performed and no reliable conclusion can be obtained at this time.
The optimal treatment for ISR has not been established yet. CEA with stent removal is more invasive but seems a safe and durable choice for patients without high risk for surgery. Endovascular interventions might be suitable for other patients. Effects of DEB on restenosis seem superior to PTA but further studies are warranted to support the results. Biofactor-eluted stent could enhance endothelial repair and reduce in-stent neointima formation, which may become a potential strategy for preventing ISR.
Conclusion
The reported ISR incidences after CAS vary widely due to inconsistencies in definitions, follow-up schemes, and detecting measurements. Neointimal hyperplasia may be the principle mechanism underlying ISR after CAS. Currently, endovascular and surgery approaches remain as the mainstays for treating ISR.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.