
Abstract
Objectives
To describe our clinical experiences and recommend a management strategy for spontaneous isolated dissection of a visceral artery.
Methods
A retrospective study of patients from December 2005 to December 2015 was performed. Thirty-two patients had spontaneous isolated dissection of a visceral artery. Clinical features, computed tomography findings, the treatment method, and follow-up results were evaluated.
Results
There were 28 men and 4 women (mean age, 54 years). Dissection locations were the celiac artery in 10, superior mesenteric artery in 17, and celiac artery and superior mesenteric artery in 5 patients. Celiac artery stenosis existed with spontaneous isolated dissection of a visceral artery at a high rate. After diagnosis, the blood pressure of all patients was immediately controlled to a lower level. Three patients with arterial rupture and one patient with bowel infarction underwent operations for complications. Overall, the treatment of dissection involved drug therapy alone. The last follow-up computed tomography results of the true lumen residual ratio and the length of the dissected artery improved compared to the values on admission; the maximum diameter of the dissected artery did not enlarge. Eleven patients almost completely improved. No patients had any adverse event.
Conclusions
Most patients with spontaneous isolated dissection of a visceral artery can be first treated conservatively for dissection with strict blood pressure control and surveillance.
Introduction
Spontaneous isolated dissection of a visceral artery (SIDVA) without associated aortic dissection is rare, but it has become frequently identified because of the development of computed tomography (CT). 1 Different treatment options have been reported for managing SIDVA, including conservative management, 2 endovascular intervention, 3 and open surgery. 4 However, the optimal initial treatment for dissection remains controversial. The purposes of the present study were to analyze the clinical course of patients with SIDVA and to propose the optimal treatment for SIDVA, specifically for dissection itself.
Patients and methods
This retrospective study included 32 consecutive patients with symptomatic SIDVA at our hospital between December 2005 and December 2015. All patients presented with acute onset abdominal pain. The diagnosis of SIDVA was made according to multi-detector CT angiography (CTA) findings. Patients with concomitant aortic dissection were excluded from the study.
We retrospectively reviewed patients’ clinical features, history, complications on admission, CT findings, including the true lumen residual ratio (TLRR) (i.e. the minimum value of the true lumen size compared to the transverse section of the dissected artery), length of the dissected artery, and maximum diameter of the dissected artery, treatment modalities, and long-term follow-up results.
In patients with bowel ischemia, we assessed the blood flow of branches of the superior mesenteric artery (SMA) (i.e. the middle colic artery, jejunal artery, and inferior pancreaticoduodenal artery) and other visceral arteries (i.e. the celiac artery (CA) and inferior mesenteric artery (IMA)) on CT scans.
Values are presented as the mean ± standard deviation. Categorical variables were compared using the χ2 test, and continuous variables were compared using the Mann–Whitney U test. Statistical analysis was performed using SPSS software (Windows version 22.0; SPSS Inc., Chicago, IL).
This study was approved by an ethics committee (approval no.: 15-138).
Results
This study included 28 men and 4 women with ages ranging from 30 to 85 years (median age, 54 years). All patients were Japanese. A medical history of only hypertension was identified in 13 patients. No patients had a clinical history or family history of arterial dissections, connective tissue diseases, or viral/bacterial infections based on the results of our hematological examinations. Thirteen patients had an incorrect radiological interpretation by a local doctor at their first medical examination. At the time of admission, hypertension was detected in 19/32 patients, and bloody stool was found in 2/32. The laboratory data were not significant.
Initial CT findings at our hospital showed that the locations of dissection were the CA in 10, SMA in 17, and CA and SMA in 5 patients. The other renal, carotid, and iliac vessels were normal. The TLRR was 27.4 ± 18.1%. The length of dissection was 60.6 ± 19.5 mm. The maximum diameter of dissection was 11.5 ± 1.7 mm. Seventeen (53%) patients had SIDVA and CA stenosis, which were due to median arcuate ligament syndrome in 10 patients and atherosclerotic change in 7. Three patients had bowel ischemia, two had splenic infarction, and three had arterial rupture from the peripheral branch of the CA or SMA. According to the blood flow evaluation using CT angiography, in one patient with bowel ischemia who underwent resection of the necrotic transverse colon, the CA and IMA were patent; however, the blood flow of the middle colic artery and jejunal arteries disappeared, and the TLRR of the SMA main trunk was 10%. In two patients with bowel ischemia who did not undergo an operation, the TLRR of the SMA main trunk was 0%, but the blood flow of the visceral artery branches, including the CA and IMA, were patent.
After diagnosis, treatment plans of all patients involved controlling the blood pressure immediately to a lower level (100–120 mmHg), which is similar to the treatment for type B acute aortic dissection, and we administered an analgesic in the intensive care unit. Nineteen patients with a higher blood pressure in the emergency department received a β-blocker and calcium blocker for blood pressure control, and six took an anticoagulant drug (heparin from 10,000 unit/day) to maintain the peripheral blood flow and avoid thromboembolic complications. Then the antihypertensive drugs were administered orally within a few days, and the anticoagulant drugs were stopped after confirming peripheral flow on a CT scan after a few days. There were no defined indication criteria for the use of anticoagulant drugs. These drugs were only used in patients for whom the primary doctor deemed appropriate. Antiplatelet therapy was not used in our study.
Eight patients had complications (arterial rupture from the peripheral branch of the CA or SMA in three, bowel ischemia in three, and splenic infarction in two) with dissection. Among them, three patients with arterial rupture underwent transcatheter arterial embolization, and one patient with bowel necrosis underwent bowel resection. Other patients underwent conservative therapy. In all patients, the treatment of dissection only involved medication. After conservative treatment, the abdominal pain was relieved presently and analgesics could be stopped.
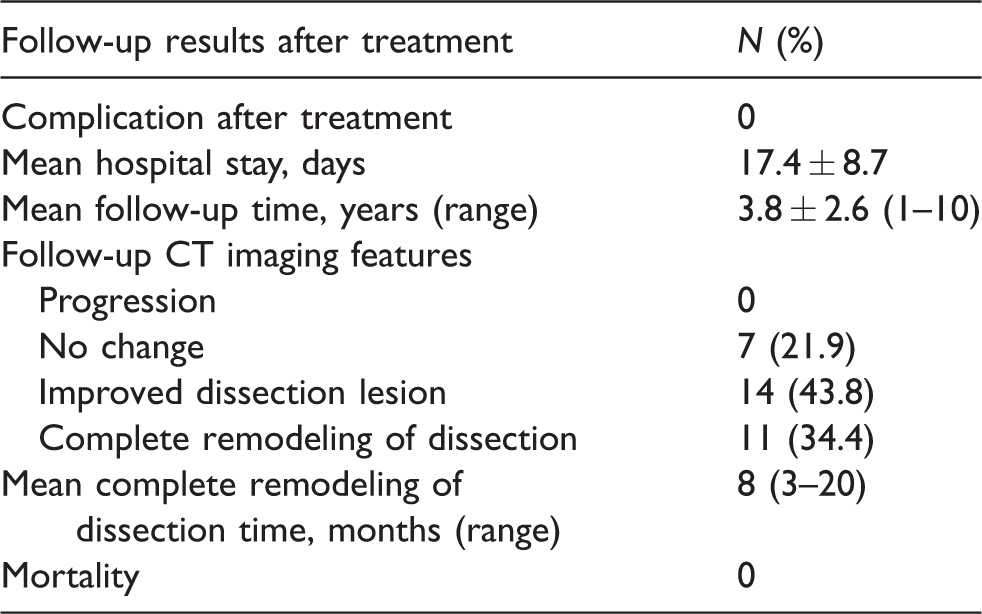
After treatment, CT imaging indicated the following changes. On the final CT scans, the TLRR was 73.7 ± 27.5%, length of dissection was 17.6 ± 19.5 mm, and maximum diameter of dissection was 9.0 ± 2.5 mm. The last follow-up results of the TLRR and length of the dissected artery improved compared to those at the time of admission, and the maximum diameter of the dissected artery did not increase (p < 0.01; Table 1). The CT findings of 11 patients almost completely improved within a mean period of eight months (range, 3–20 months) (Figures 1 and 2). No patients had any adverse event during the follow-up period of 1–10 years. Follow-up results after treatment are shown in Table 2.
Changes of TLRR and dissected artery.
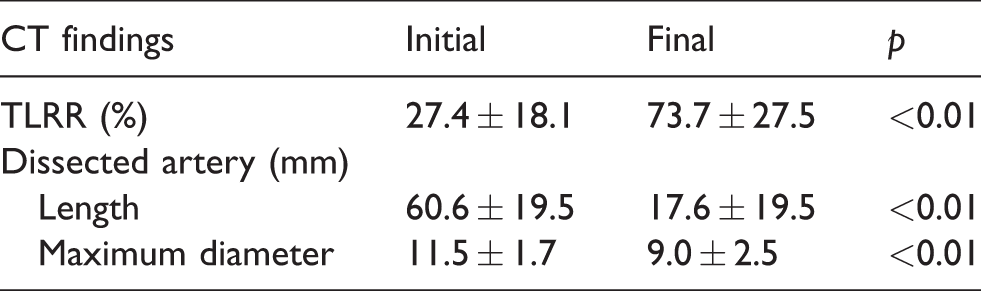
CT: computed tomography; TLRR: true lumen residual ratio. Mann–Whitney U test.
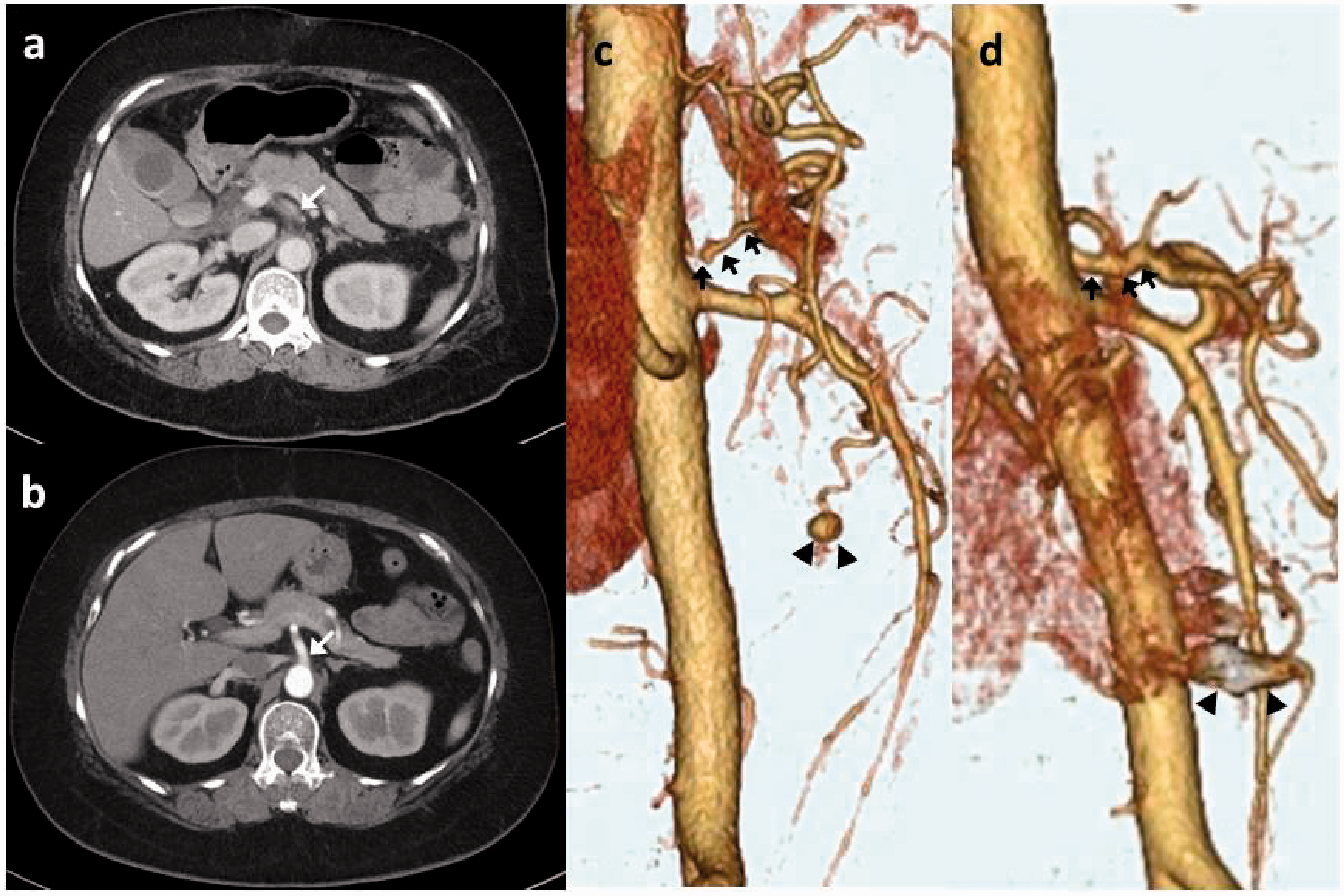
Celiac artery (CA) dissection. (a) Initial and (b) final axial computed tomography (CT) scans. (c) Initial and (d) final three-dimensional CT images. Arrows indicate the CA. Arrowheads indicate an aneurysm and an aneurysm filled with a coil. The dissected artery almost achieved complete remodeling.
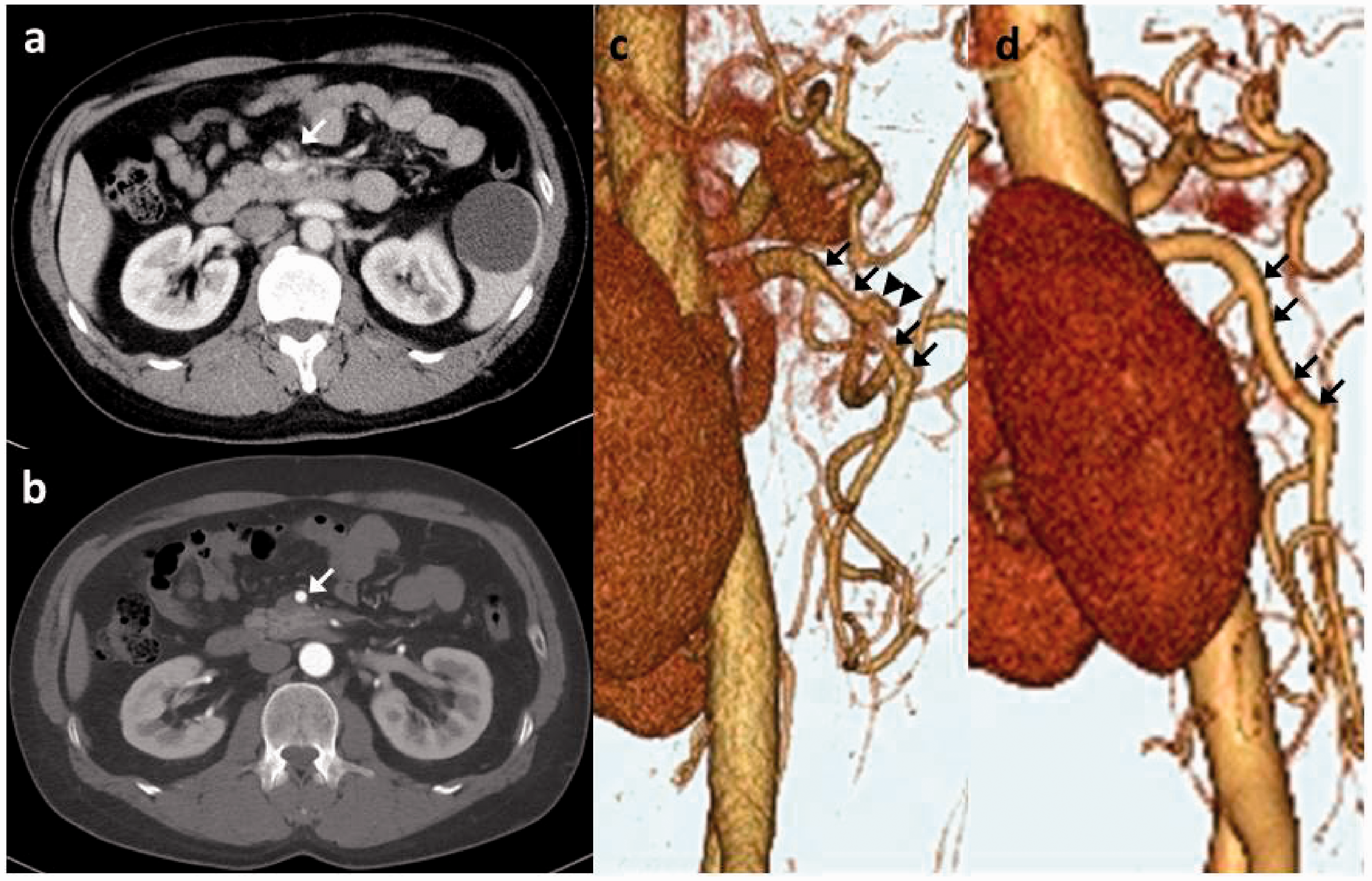
Superior mesenteric artery (SMA) dissection. (a) Initial and (b) final axial computed tomography (CT) scans. (c) Initial and (d) final three-dimensional CT images. Arrows indicate the SMA. Arrowheads indicate an ulcer-like projection. The dissected artery almost achieved complete remodeling.
Follow-up results after treatment.
Discussion
SIDVA without associated aortic dissection is considered rare. However, there have been an increasing number of reports of SIDVA since improvements in technology and the widespread use of CT imaging for abdominal pain. 1 As a well-established, noninvasive method for evaluating vascular anatomy and pathology, CTA has been shown to be as accurate as conventional angiography. Additionally, advances in CTA have improved diagnosis and prognosis.
SIDVA should be considered in the differential diagnosis of acute abdominal pain. 5 If patients have only mild pain at the initial medical examination, CTA is rarely performed. In these cases, physicians are unable to diagnose SIDVA. In our study, the number of patients who were misdiagnosed was also large (13 (40.6%)). Therefore, CTA should be performed for acute abdomen, if the diagnosis is unclear.
There are no definite causes of SIDVA. However, the risk factors that have been suggested include hypertension, atherosclerosis, fibromuscular dysplasia, cystic medial necrosis (secondary to Marfan or Ehlers–Danlos syndrome), trauma, pregnancy, infection, and vasculitis (e.g. Takayasu arteritis, polyarteritis nodosa, and giant cell arteritis).6–12 The differential diagnosis of isolated spontaneous visceral dissection should include segmental arterial mediolysis (SAM). Typical findings include dissection, aneurysm, stenosis, occlusion, and hemorrhage caused by lytic degeneration of the arterial media. Visceral arteries are most commonly affected, and involvement of the intracranial, pulmonary, coronary, renal, and iliac arteries is rare. 13 The major causes of SIDVA are divided into histological and hemodynamic change. The former such as SAM is difficult to diagnose without histological diagnosis. However, the latter can be diagnosed by angiography.
In our study, 17/32 (53.1%) patients had SIDVA along with CA stenosis and post-stenotic dilatation on CT. CA stenosis was defined as up to 75% stenosis, because patients with up to 75% stenosis had a large pressure difference between the abdominal aorta and CA, and increased SMA flow.14,15 A main cause of CA stenosis was CA compression from the median arcuate ligament, and another cause was atherosclerotic change. Among patients with CA stenosis due to these two causes, three patients underwent angiography. In all these patients, branches of the CA domain were enhanced through the pancreaticoduodenal artery by SMA angiography. Thus, there is a possibility that patients with CA stenosis can develop dissection or aneurysm of the SMA domain because of a high flow of the SMA, which supplies an inadequate CA domain flow. However, every time patients with CA compression breathe, damage is inflicted on the CA. 16 Therefore, we speculate that there is a possibility that CA compression leads to CA dissection. In summary, CA stenosis involved with CA compression suggests the high possibility of one of the causes of SIDVA. We believe that SIDVA is caused primarily after aneurysmal degeneration. In the future, it is necessary to consider the optimal treatment of CA stenosis as the fundamental treatment of SIDVA.
The optimal treatment strategy remains controversial because the etiology and pathophysiologic mechanisms of the disease have not yet been clearly established. Variable therapeutic approaches for dissection, including conservative treatment, endovascular therapy, and surgery, have been used as treatment methods.
The rate of conservative treatment in all patients in the current series is similar to that in another series (95% (18/19 patients)). 17 In a recently documented series of 17 patients, observation without anticoagulation treatment was reported in 3 (17.6%) patients, anticoagulation treatment in 12 (70.6%), and endovascular stenting in 2 (11.8%). 18 Of the 28 patients in another series, 19 were managed conservatively without anticoagulation therapy, 6 with endovascular stent insertion, and 3 with surgery. 19 The gradual improvement after successful conservative treatment is similar to that in a recent report 20 on the natural history of spontaneous isolated dissection of the SMA (SIDSMA). In their report, among 58 consecutive patients with SIDSMA, 46 received conservative management (12 patients received antithrombotic therapy and 34 received no antithrombotic medication) and follow-up with CTA. They reported that follow-up CTA findings showed a decrease in the size of the false lumen in 19 (41.3%) patients, complete remodeling of dissection in 7 (15.2%), and no change in 20 (43.5%) patients. Therefore, 56.5% of patients had morphologic improvement or complete remodeling after conservative management within a median time of 8.2 months. Additionally, they noted that SIDSMA with a patent false lumen showed a propensity for no change on follow-up CTA. As previously stated, the therapeutic regimen should be based on clinical symptoms, and conservative management is feasible in most cases. SMA stenosis cannot be an indication for invasive treatment, because stenosis of the true lumen has been seen to improve after the acute stage of dissection. 21 In some reports, isolated CA dissection has also been initially treated with conservative therapy safely.22,23 There is no consensus on optimizing blood pressure to achieve adequate visceral perfusion. 24 At our hospital, the blood pressure of all patients was controlled to a lower level (100–120 mmHg) using a treatment similar to that for type B acute aortic dissection to decrease hemodynamic stress on the dissected artery. Currently, since there is no consensus regarding treatment, it is best to use anticoagulation and antithrombotic therapy, although there may be possible negative effects. 25 Therefore, our recommendation for management of an incidental asymptomatic SIDVA when the CTA was performed for unrelated indications is also conservative therapy with blood pressure management.
Surgical or endovascular treatment may be reserved for patients who remain symptomatic despite optimal medical treatment and for those with complicated dissection (i.e. the progression of dissection, aneurysmal formation, ischemia, or rupture). 26 Complications of dissection such as ischemia or bleeding are considered poor prognostic features. 27 Endovascular therapy offers safe and quick therapy for patients with SIDVA. The first description of this approach by Leung et al. was followed by multiple reports of successful treatments by several authors describing complete resolution of the pain in most cases.28,29 At the six-month follow-up, stent patency was found in 100% of patients. However, there are some reports of failure. One author reported a failure rate for endovascular interventions of up to 50%, and another author reported stent misplacement in the false lume. 30 The indication for open surgery should also be limited. No recent reports have indicated that operative management should be performed first for the dissected artery itself. Additionally, it seems that if open surgery is performed, the risk of operative revision is up to 28.6%, and the mortality rate is significantly increased compared to that of other therapeutic options. 12
According to our study’s findings, 4/32 (12.5%) patients underwent surgical or endovascular treatments, 3 underwent transcatheter arterial embolization, and 1 underwent bowel resection for bowel necrosis at the time of admission. However, no patients underwent surgical or endovascular treatment for dissection. After treatment, no patients deteriorated during the follow-up period. Furthermore, the natural remodeling rate was up to 30%. Therefore, patients with SIDVA should be first treated conservatively for dissection with strict blood pressure control and surveillance.
The limitations of this study were its single center, retrospective design, and small sample size. It is necessary to continuously investigate and determine the optimal treatment for SIDVA in the future.
Conclusions
Most patients with SIDVA can be first treated conservatively for dissection with strict blood pressure control and surveillance. Additionally, CA stenosis suggests the high possibility of one of the causes of SIDVA. It is necessary to investigate this topic further.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.