
Abstract
Objectives
Visceral arterial aneurysms may be treated using open surgery or endovascular repair, but the best approach remains controversial. This was a retrospective study aiming to compare open surgery and endovascular treatment strategies for visceral arterial aneurysms.
Methods
The study included all 93 patients who were admitted with visceral artery aneurysms between January 2001 and January 2011 at the Department of Vascular Surgery, Changhai Hospital, Shanghai, China. All cases underwent either open or endovascular procedures. Overall survival and adverse events were compared between the groups. Success rate, blood loss, length of surgery, and length of hospital stay were also compared. The patients were followed up at three, six, and 12 months then every year until April 2014.
Results
Open surgery was performed on 34 patients and endovascular procedures on 59. There were no differences in characteristics of the patients between the open surgery and endovascular groups. The perioperative complication rate was 52.9 and 13.6% in the open surgery and endovascular groups, respectively. Mean follow-up was 36.8 months (range: 11 months to 10 years). The one- and five-year survival rates were 100 and 60.6%, respectively, in the open surgery group, compared to 100 and 84.5% in the endovascular group. Multivariate analysis for factors related to overall survival showed that there was a significant relationship with the treatment approach (HR = 0.479, 95%CI: 0.278–0.825; P = 0.008) and the presence of false aneurysm (HR = 2.929, 95%CI: 1.388–6.180, P = 0.005).
Conclusions
Endovascular repair could be considered as an effective method for visceral artery aneurysm. Endovascular repair showed lower perioperative complication rates and better long-term survival.
Introduction
Visceral artery aneurysm is an arterial disease with a low prevalence (0.3–2%).1,2 Some aneurysms are incidental findings, but some patients are admitted for emergency surgery after aneurysm rupture and these patients have poor outcomes, with mortality rates around 20–70%.2,3 The increasing use of imaging examinations has improved the incidental detection rate of visceral artery aneurysms, while the development of percutaneous intervention techniques has improved their treatment.3,4
Although visceral artery aneurysms may involve different areas of various arteries, they can be considered as a single entity because their pathogenesis is similar. In addition, their location has no significant role in the prognosis of visceral artery aneurysms. 5 However, since the prevalence of visceral artery aneurysms is low, many questions remain unanswered regarding the treatment indications and approaches. There is a wide range of treatment options available to the surgeon. The traditional approach is open surgical repair, 3 and a study has shown in a small group of patients that this method was successful and without complications during postoperative follow-up. 6 It is believed that open surgery should be performed for confirmed visceral artery aneurysms to avoid adverse events caused by aneurysm rupture.7,8 The risk of rupture of splenic artery aneurysms is the lowest, but the risk is significantly increased in pregnant women and the mortality rate reaches 75%, 9 requiring open surgery. However, the main disadvantage of open surgery is the surgical trauma. Nevertheless, the recent and rapid development of endovascular techniques has greatly expanded their indications for the treatment of visceral artery aneurysm, and many patients have benefited from these procedures.4,10 Among others, the surgical trauma is less important, but stents may be contraindicated in cases of varicosity, if the anchorage area is improper, or if there is a possibility of obstructing a branching artery.
At present, few studies reported the middle- or long-term follow-up after open surgery or endovascular techniques for visceral arterial aneurysm. Therefore, this study aimed to evaluate the treatment strategies for visceral arterial aneurysms by retrospectively analyzing the cases treated at a single center over 10 years.
Materials and methods
Patients
This was a retrospective study of patients treated between January 2001 and January 2011 at the Department of Vascular Surgery, Changhai Hospital, Shanghai, China. The study included all patients admitted for visceral artery aneurysms during the study period. The patients had to have been surgically treated at the center. Patients with connective tissue diseases were excluded. This study was approved by the Ethics Committee of Changhai hospital (# CH2011012).
Diagnostics and preoperative preparations
The type and diameter of the visceral artery aneurysm were confirmed through computed tomography angiography (CTA) imaging at hospital admission. Treatment indications included (1) true artery aneurysm with a diameter >2 cm, (2) false artery aneurysm, 11 (3) young female patients who want to have children (to avoid aneurysm rupture during pregnancy), 12 or (4) patients with acute abdominal pains and imaging suggestive of visceral arterial aneurysm. 13
Summary of treatments
The treatment approach was decided after comprehensive evaluation (physical examination and imaging) of the relationship between the location of the aneurysm and the peripheral tissues, and the patients’ cardiopulmonary function.
Follow-up and observational indexes
Patients in both groups were followed up at the outpatient department of our hospital at three, six, and 12 months, and then every year. Follow-up was censored on April 2014 or death. The main observational outcomes were overall survival and adverse events. Clinical variables such as success rate (success was defined as a resolved aneurysm), blood loss, length of surgery, length of hospital stay, and complications were collected. CTA was used to evaluate all patients.
Statistical analyses
Continuous variables are expressed as means ± SD and were analyzed using the independent sample Student’s t-tests. Categorical variables are expressed as frequencies and percentages and were analyzed using the chi-square test. The Kaplan–Meier method was used for survival analysis and the differences between the two groups were assessed using the log-rank test. Cox multivariate analysis was performed to find factors related to overall survival. Differences were considered significant when the P-value was <0.05. All analyses were performed using SPSS 17.0 (IBM, Armonk, NY, USA).
Results
Characteristics of the patients
Ninety-three patients (47 males and 46 females; mean age of 49.1 ± 12.9 years) were included; 34 underwent an open surgery and 59 underwent an endovascular procedure. In the open surgery group, 28 patients underwent aneurysmectomy, two underwent aneurysmectomy and prosthetic vascular bypass, and four underwent aneurysmectomy and angioplasty. In the endovascular group, 33 patients underwent coil embolization, 26 underwent endovascular aneurysm exclusion, and two finally underwent open procedures because of abnormal anatomy of the parent artery.
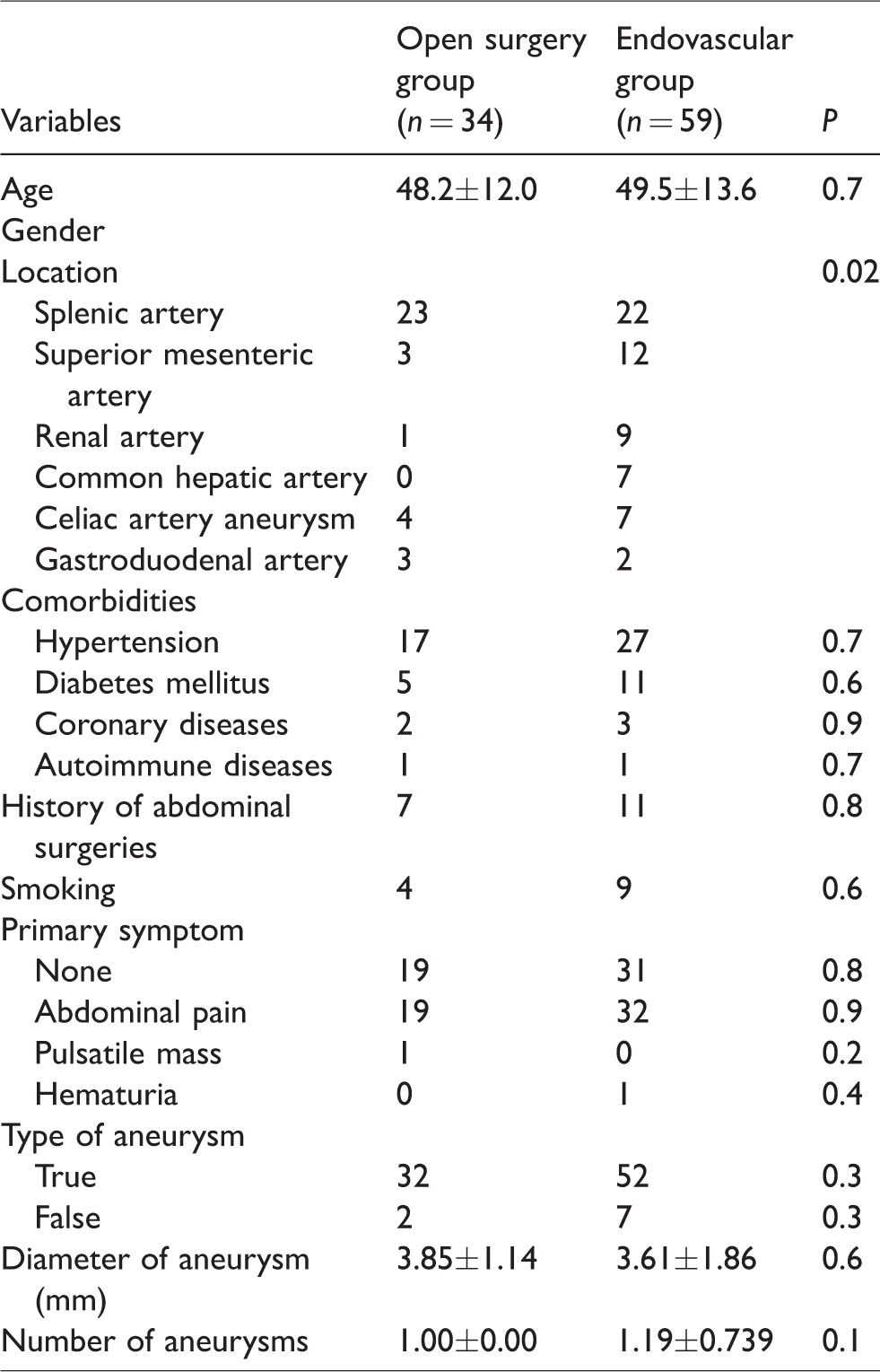
General characteristics of the patients are summarized in Table 1. Of the 93 patients, 50 were found with visceral artery aneurysms during routine physical and imaging examinations, 41 for obvious abdominal pain, one for abdominal pulsatile mass (splenic artery aneurysm), and one for hematuria (renal artery aneurysm). There were no differences in age, gender, and comorbidities between the open surgery and endovascular groups (all P > 0.05).
Characteristics of the patients.
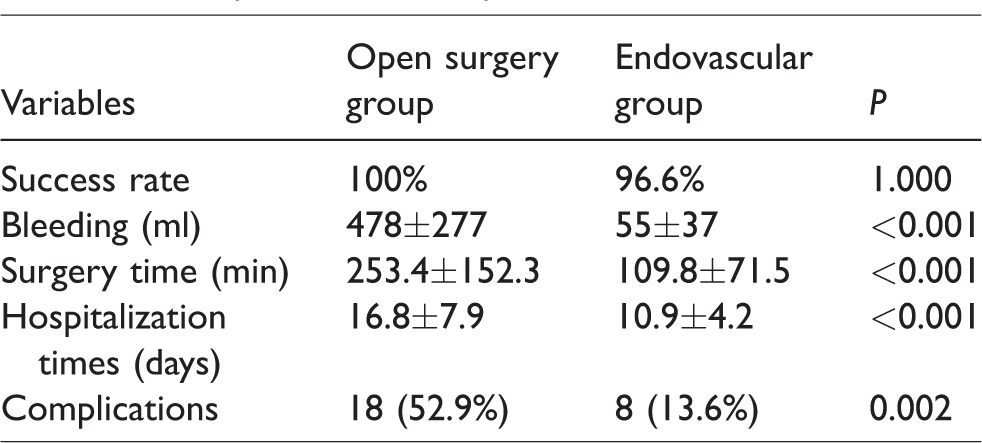
Comparison of the operative data.
Perioperative data
The success rate in the endovascular group was 96.6% (57/59). One case of splenic artery aneurysm finally had to undergo open surgery because it was found to have a common trunk with a common hepatic artery aneurysm; because the orifice of the splenic artery aneurysm involved the common orifice and endovascular embolism might have led to the occlusion of the hepatic artery, splenic ligation was then performed. The other case had a superior mesenteric artery aneurysm, which had an orifice in the splenic artery toward the aneurysm lumen during operative imaging; since the selective embolization of the splenic artery failed, superior mesenteric artery aneurysmectomy was performed. Both cases successfully underwent open procedures.
The amount of bleeding was 478 ± 277 ml for the open surgery group and 55 ± 37 ml for the endovascular group (P < 0.001). Mean surgery time was 253.4 ± 152.3 min for the open surgery group and 109.8 ± 71.5 min for the endovascular group (P < 0.001). Mean hospitalization was 16.8 ± 7.9 days for the open surgery group and 6.9 ± 4.2 days for the endovascular group (P < 0.001). In the open surgery group, a patient with false superior mesenteric artery aneurysm died 10 days after surgery due to graft infection after aneurysmectomy and prosthetic revascularization. No deaths occurred in the endovascular group during the perioperative period.
Among all patients, 18 (52.9%) complications were found in the open surgery group postoperatively, compared to eight in the endovascular group (13.6%) (P = 0.002). The operative data were analyzed in table 2.
Overall survival
Ninety patients were followed up on the long term. Mean follow-up was 36.8 ± 13.2 months. Both groups had a one-year survival of 100%, but three- and five-year survival were 81.3 and 60.6% for the open surgery group compared to 94.8 and 84.5% for the endovascular group, respectively (Figure 1).
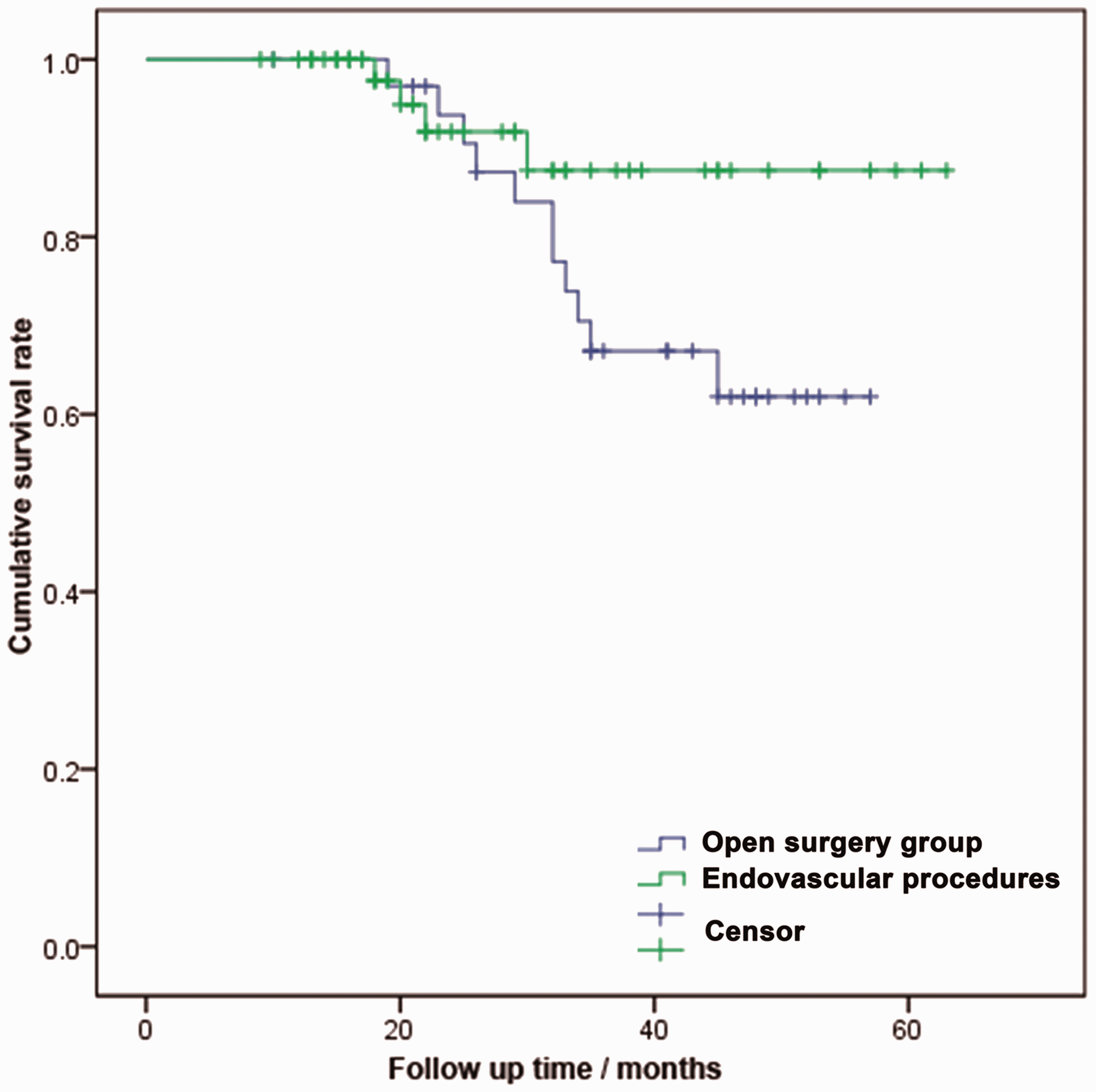
Survival analysis of the visceral artery aneurysm patients during long-term follow-up. The open surgery group is shown in blue and the endovascular procedures group is in green. Vertical lines represent censored data. Survival was significantly different between the two groups (P = 0.013).
The multivariate analysis for factors related to overall survival is shown in Table 3. After adjustment, the endovascular treatment method (HR = 0.479, 95%CI: 0.278–0.825, P = 0.008) and the presence of a false aneurysm (HR = 2.929, 95%CI: 1.388–6.180, P = 0.005) were independently associated with overall survival.
Cox multivariate analysis for overall survival.
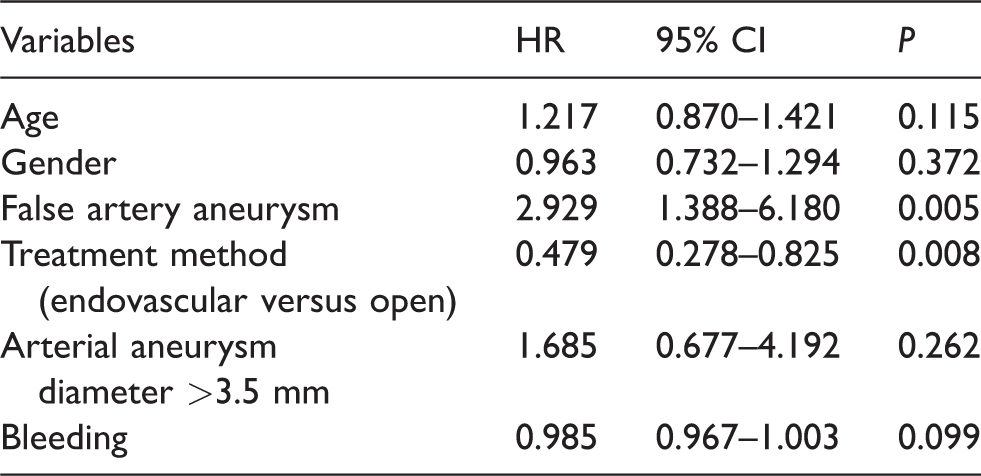
CI: confidence interval; HR: hazard ratio.
Subgroup analyses
The one-year total embolization success rate for the endovascular splenic artery aneurysm subgroup was 60%, and this rate increased to 90% at three years. Embolization success is defined as the absence of contrast agent into aneurysm.
In the superior mesenteric artery aneurysm subgroup, three patients with coil embolization were totally embolized at one year, seven patients with endovascular exclusion had a significantly decreased aneurysm diameter, and two patients who underwent open surgery recovered well and CTA suggested the vessels without stenosis or aneurysm dilatation.
In the renal artery aneurysm subgroup, one patient who underwent open surgery died from cerebral infarction at 26 months after surgery.
In the celiac artery aneurysm subgroup, one patient who underwent an open procedure died three years postoperatively from respiratory failure caused by severe pneumonia and one patient died five years after surgery in a traffic accident.
In the gastroduodenal artery aneurysm subgroup, prosthetic vessels and bare stents showed patency during follow-up except for one patient who underwent open surgery, who was diagnosed with gastric cancer one year after surgery; he died during the second year.
Discussion
The aim of this study was to evaluate retrospectively the treatment strategies for visceral arterial aneurysms over 10 years at a single center. The perioperative complication rate was 52.9 and 13.6% in the open surgery and endovascular groups, respectively. The one- and five-year survival rates were 100 and 60.6%, respectively, in the open surgery group, compared to 100 and 84.5% in the endovascular group. Multivariate analysis for factors related to overall survival showed that there was a significant relationship with the treatment approach and the presence of false aneurysm.
The most common treatment approach for visceral artery aneurysm, especially for a false visceral artery aneurysm, is to prevent blood from entering the aneurysm lumen to avoid pressure on the aneurysm wall, which may cause rupture of the aneurysm. Open procedures often involve the ligation of the artery aneurysm. In our experience, a traditional open procedure is indicated when the preoperative imaging data show unfavorable structures of the aneurysm that is not suitable for endovascular treatment, or when the middle- and long-term outcomes of endovascular treatment are not satisfactory. In addition, when preoperative evaluation suggests that coil embolization may affect the distal blood supply to distal organs or compensatory dysfunction of organs, aneurysmectomy and revascularization should be used. A few studies have also reported that for patients with hepatic artery aneurysms and poor liver function, the patency rate of a graft by prosthetic vascular bypass is higher than that of a covered stent combined with coil embolization on the long term; therefore, prosthetic vascular bypass may have fewer effects on liver functions. 14
In 1998, our center began to treat abdominal aortic aneurysm by covered stent 15 and this yielded a favorable curative effect. Among 93 patients, a 96.6% success rate was achieved in the endovascular group, which was comparable to the 98% achieved in other studies.14,16 Therefore, endovascular treatments became the first choice for visceral artery aneurysm in our center because of the significant advantages seen in the endovascular group compared to the open surgery group (shorter surgery time, less bleeding, less time at the hospital, and decreased perioperative complication rates). Previous studies have also compared these techniques,4,17–20 but this study is the first to compare them in a Chinese population and with a long-term follow-up. During treatment approach selection for visceral artery aneurysms, endovascular treatment should first be considered for elderly patients and those admitted for emergency surgeries for aneurysm rupture16,21; otherwise, an open procedure might be considered.
However, since implantation of covered stents is affected by the length of the anchorage zone on both ends of the aneurysm and arterial dilatation, as well as the stent diameter, the use of a covered stent in not popular. Recently, covered stents of smaller diameters have shown more significant protective effects on blood supply to distal organs, which promotes the use of covered stents in the treatment of visceral artery aneurysms. Nevertheless, no consensus has yet been reached on antiplatelet and anticoagulation therapy after implantation of a covered stent because intrastent embolus is still the most dangerous risk of this method. Rossi et al. 22 reported intrastent emboli in four cases of endovascular exclusion of covered stents for celiac and splenic artery aneurysms within 24 months after surgery. In this present study, 26 patients received covered stents, among which one case of common hepatic artery aneurysm presented with acute intrasent embolus one day after surgery; there were no complications in the other patients during follow-up.
It is noticeable that patients with infectious false artery aneurysm have a higher incidence rate of graft infection compared to the other types of artery aneurysm, indicating that the use of anti-infectious treatments during the perioperative period might be warranted. In this study, one patient had a major infectious superior mesenteric artery aneurysm (diameter of 70 mm). Since the covered stent was unable to pass the varicose parent artery and because significant tissue adherence by preoperative imaging increased the difficulties of aneurysmectomy, abdominal aorta and superior mesenteric arterial bypass using an 8 mm prosthetic vessel combined to coil embolization was used to implant 12 spring coils and two pieces of gelatin sponge. On the fourth day after surgery, the patient had abdominal pain and fever of 39°C, and was diagnosed with graft infection but soon died after active treatments.
Since postoperative revascularization of the aneurysm lumen occurs usually within 30 days after surgery, postoperative imaging reexamination should be performed within 96 h to evaluate the blood supply of the parent artery and distal organs. Meanwhile, the primary symptoms and severity of the disease should also be taken into consideration. The postoperative reexamination time for patients with primary symptoms of aneurysm rupture should be earlier than for asymptomatic patients, even if operative imaging showed total exclusion for a few revascularizations found during short-term reexamination. Cochennec et al. 23 reported 11 cases of splenic artery aneurysm treated by endovascular method, and the revascularization rate was 5% at 30 days after surgery, supporting the need for postoperative short-term imaging reexamination. In this present study, revascularization six months after surgery was observed in one patient; it was then treated using secondary coil embolization.
The retrospective nature of this study means that it has some limitations. The wide range of techniques within the two groups and the long period over which the patients were included mean that it is difficult to directly attribute the risks and benefits of one method over another and no risk analysis could be performed. In addition, subgroups analyses were impaired by the small number of patients in some subgroups. We could also not effectively evaluate the aneurysms in terms of location or between true and false types of aneurysm. This was in part due to the low prevalence of visceral artery aneurysms, resulting in a small number of patients, although it is still higher than most previous studies.
In conclusion, endovascular repair could be considered as an effective method for visceral artery aneurysm. Endovascular repair showed lower perioperative complication rates and better long-term survival.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.