
Abstract
Background
Whilst the management of blunt traumatic thoracic aortic injury has seen a paradigm shift to an ‘endovascular first’ approach, the limitations of thoracic endovascular aortic repair remain. An inadequate proximal landing zone limits the use of thoracic aortic stent grafts and in an emergent polytrauma setting, aortic arch debranching via open surgery may not be practical or feasible. A wholly endovascular approach to debranching utilising ‘off-the-shelf’ stents and parallel graft techniques may represent a possible solution. Hence, we sought to perform a systematic review investigating the use of chimney graft techniques alongside thoracic aortic stenting in blunt traumatic thoracic aortic injury.
Methods
We performed the systematic review in accordance to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines. Searches were performed on Medline (PubMed), Web of Science and Scopus to identify articles describing the use of chimney grafts in traumatic aortic transection (PROSPERO: CRD42017082549).
Results
The systematic search revealed 172 papers, of which 88 duplicates were removed resulting in 84 papers to screen. Based on title, abstract and full text review, six articles were included for final analysis. There were nine patients in total with an average age of 41 (three females, five males, one unspecified), all with significant polytrauma, secondary to the mechanism of injury. A variety of stents were used between centres, with techniques showing a predominance to stenting of the left subclavian artery (77%, n = 7). The technical success rate was 82%, with two (18%) cases of type 1 endoleaks, of which one resolved spontaneously.
Conclusions
Despite the encouraging results, this by no means provides for a firm conclusion given the small sample size. Patients should still be judiciously selected on a case-by-case basis when employing the chimney graft technique. Larger cohort studies are needed to establish these findings.
Keywords
Introduction
Blunt traumatic thoracic aortic injury (BTTAI) is a rapid deceleration injury, typically sustained in motor vehicle crash or a fall from height. 1 It encompasses a spectrum of injurious pathology, from small intimal defects to full-thickness aortic transections with rupture. First proposed in 2009 2 and subsequently adopted by the Society for Vascular Surgery (SVS), 3 injuries are stratified to four categories based on a grading system: grade I (intimal tear), grade II (intramural haematoma), grade III (pseudoaneurysm) and grade IV (rupture). Epidemiological studies have shown that mortality is estimated to be as high as 84% for those before reaching the hospital, 4 and of those who do survive to make it to the hospital, mortality remains dismally high at 32%. 5 However, a rapid advancement of care has taken strides during the last two decades.
Open surgical repair has been the cornerstone of treatment for BTTAI since 1959. However, Parodi et al. 6 and Volodos et al. 7 propounded endovascular aneurysm repair (EVAR) as a minimally invasive treatment for abdominal aortic aneurysms. It has since evolved rapidly and is now heralded as the safest treatment for BTTAI.8–11 This is also reflected in the recommended guideline from the SVS, which currently recommends thoracic endovascular aneurysm repair (TEVAR) over open surgical repair or non-operative management for grades II, III and IV BTTAI. 3 However, the endovascular approach carries a small but appreciable rate of neurological, procedural-related and overall mortality. 12 In addition, the longevity of TEVAR for young patients with poor compliance and consequent loss of follow-up remains to be elucidated. 2
In such rapid deceleration injuries, polytrauma is common and BTTAIs untreated are a surgical emergency and potentially fatal. The chimney graft technique may be a viable alternative in such urgent cases that are either unfit for open repair or have poor sealing zone for standard graft repair. The implantation of a chimney stent graft was first reported in the literature in 2003. 13 This approach allows for extension of the proximal landing zone quickly, particularly in emergency situations where a traditional open surgical aortic arch debranching would be inappropriate. If the innominate or left common carotid arteries require coverage, preemptive revascularisation is mandatory. However, the level of evidence supporting left subclavian revascularisation in such patients is weak, although it may be associated with a decreased risk of paraplegia.
Therein exist a few versions of the chimney graft technique. Conceptually, it involves the placement of a stent-graft alongside the aortic endograft in a parallel fashion to provide inflow to aortic branches that are covered fully or partially during the procedure (Figure 1). The sandwich technique was first employed to preserve the internal iliac arteries and subsequently the visceral arteries in thoraco-abdominal aneuruysms. 14 It utilises a tubular stent graft that is deployed to create an artificial neck for chimney graft implantation. Thereafter, the primary aortic stent graft is attached to another piece to exclude the whole aneurysm, resulting in the chimney grafts being ‘sandwiched’ between both aortic stent grafts. The periscope graft was first used to preserve the visceral arteries in a ruptured thoraco-abdominal aortic aneurysm15,16 and primarily involves a distally placed chimney graft to enable retrograde flow up to the side branches. The variation in technique nonetheless shares the common theme of being ‘sandwiched’ inside an endograft rather than inside a native artery.
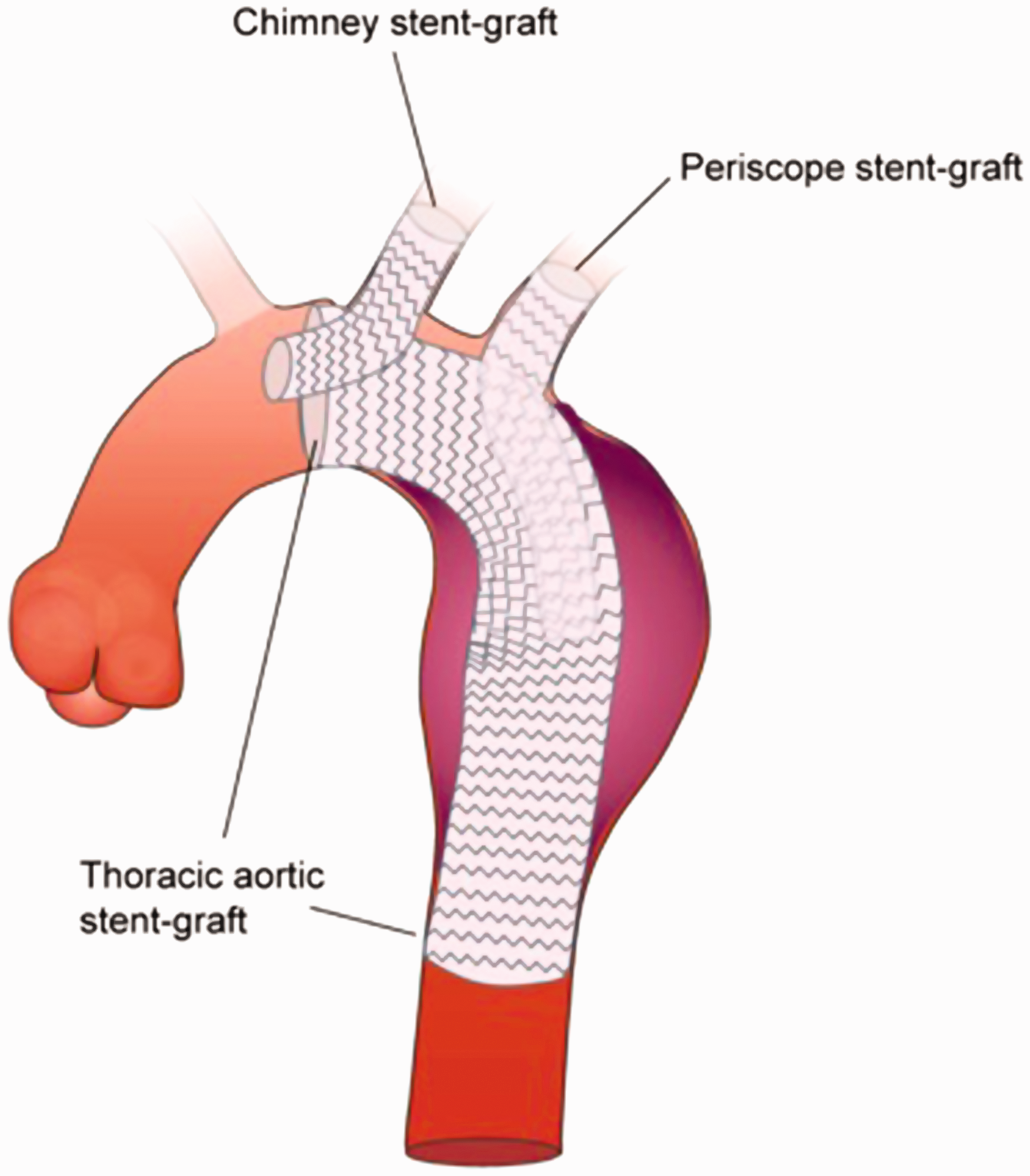
Chimney graft technique. Application of chimney technique on arch vessels, where the chimney graft is relatively short due to the seal zone distal to the origin of the carotid branch. Chimney grafts are brought up inside the proximal thoracic endograft, after which a second aortic graft overlaps to cover the branch origins and chimney grafts, hence forming the ‘sandwich technique’. As there is no seal zone distal to the subclavian as depicted in the picture, both the ‘periscope’ and ‘sandwich’ techniques can be employed to maintain subclavian flow.
The judicious selection of treatment involves a weighted calculation of risks posed by the various modalities, given the lack of supportive evidence and prospective validation as well as inadequate and specific guidelines from well-established vascular societies including the European Society of Cardiology and the Eastern Association for the Surgery of Trauma.17,18 To address this paucity of data, we seek to gather real-world evidence on the role of parallel chimney grafts in the endovascular management of blunt traumatic thoracic aortic injuries.
Methods
This review has been prospectively registered in PROSPERO (CRD42017082549). We conducted our systematic review in accordance to the Preferred Reporting Items of Systematic Reviews and Meta-Analyses statement. 19 An electronic search of the public domain databases, Pubmed, Web of Science, SCOPUS and OvidSP, was performed in November 2017 with restrictions limited to language alone.
In order to further determine the indication and role of the chimney technique in aortic transection repair, a repetitive and exhaustive combination of the following search terms were applied: (‘Aortic Injury’ AND ‘Chimney’), (‘Aortic Injury’ AND ‘Periscope’), (‘Aortic Injury’ AND ‘Snorkel’), (‘Aortic Transection’ AND ‘Chimney’), (‘Aortic Transection’ AND ‘Periscope’), (‘Aortic Transection’ AND ‘Snorkel’), (‘Blunt Traumatic Thoracic Aortic Injury’ AND ‘Chimney’), (‘Blunt Traumatic Thoracic Aortic Injury’ AND ‘Periscope’), (‘Blunt Traumatic Thoracic Aortic Injury’ AND ‘Snorkel’). The database search was supplemented by a search of the reference lists of included studies as well as utilizing the related articles function provided in each database.
Inclusion and exclusion criteria
We considered papers that discussed the use of chimney technique in the branches of the aortic arch repair. We excluded papers which exclusively discussed abdominal thoracic lesions as well as studies which discussed other endovascular or open surgical approaches. Studies involving aneurysm repair or the chimney technique of the juxta-renal branches were excluded from our review. Papers discussing only the secondary conditions of BTTAI (e.g. late renal syndrome, stroke, etc.) have also been excluded, except in cases where it is not the primary focus of the study. We have also excluded data when they are unclear whether the injury in question is thoracic or abdominal.
Study selection
Three reviewers (AMTLC, RC, IWJY) screened and assessed the studies independently for inclusion. We resolved conflicts by appeal to a fourth author. The studies were first screened by their titles and abstract, where criteria were purposely broad to include any relevant studies. We then retrieved the full-text articles for review if we could not confirm the relevance of the studies for inclusion. If disputed, NS would be the arbiter to resolve differences in study inclusion.
Data extraction and analysis
Using a standardized Pro forma, four authors (AMTLC, RC, IWJY, KP) independently extracted details of study population, interventions and outcomes. We contacted the primary author in the event of missing data in a published report. Since the majority of included studies were case reports with significant inter-study heterogeneity, we were unable to meta-analyse the data, but instead undertook narrative analysis with pooled prevalence rates.
Results
Original database searches results revealed 165 papers, with addition of seven papers from other sources. Of these 172, 88 duplicates were removed resulting in 84 papers remaining for title and abstract screening. A further 48 were excluded on the basis of their title and abstract, resulting in 36 full-text articles being reviewed in their entirety. Of these 36, 30 were excluded for inadequate data, resulting in six articles for final inclusion detailing nine cases (Figure 2).
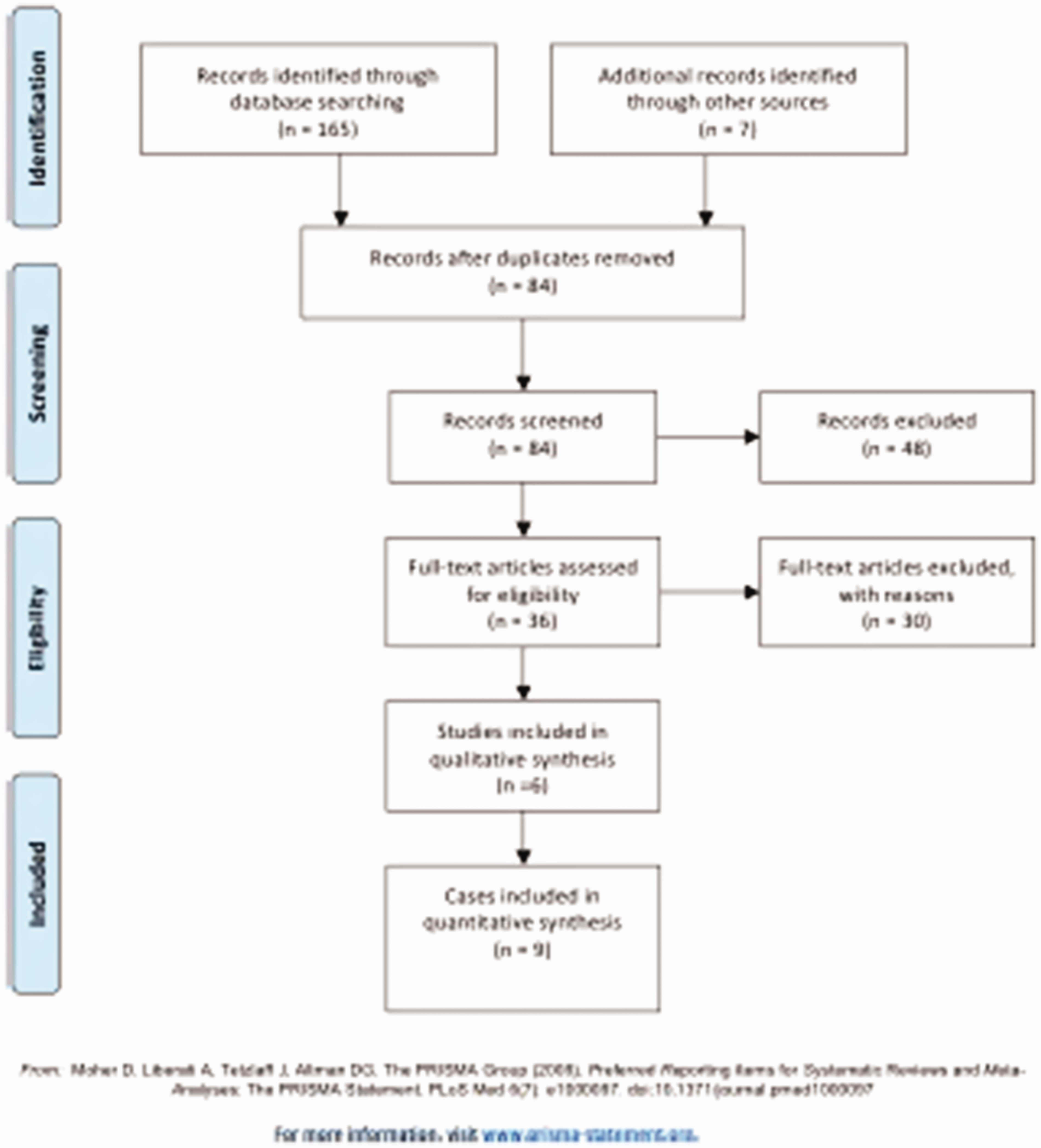
PRISMA flow diagram of search strategy.
A summary of patient characteristics, stent characteristics and clinical outcomes is detailed in Table 1. From the nine cases examined,20–25 patients had an average age of 41 (three females, five males one unspecified). All patients had significant poly-trauma, secondary to the mechanism of injury. A variety of stents were used between centres, with the majority stenting the left subclavian artery (LSA) (77%, n = 7). We have also identified a rare case of left common carotid artery coverage, 20 and an even rarer case of innominate artery coverage. 21 Baldwin et al. 20 reported the ‘double-barrel’ technique as a rescue procedure after inadvertent coverage of the left common carotid artery, where the left common carotid artery was exposed via a cut-down incision in the lower neck followed by retrograde catherization. This differs from stent deployment in the innominate artery, which is performed with the back end of the stent positioned proximally to the right carotid artery orifice. There were no complications associated with LSA coverage and stroke. In the five cases where length of stay was documented, the average was 21 days post-procedure (range: 9 days–1 month). Moreover, throughout the nine cases, 66% withstood no complications on follow-up (n = 6), whilst three demonstrated post-procedure endoleak (1×Type 1, 1×Late 1B, 1×Type 2 – Type 2 was left untreated without further complication), of which two resolved with or without intervention, a positive outcome nonetheless. Coilage was performed to resolve one of the endoleaks. 21 Another patient presented with a rupture of a distal Type 1B endoleak six months after a successful treatment; however, the cause was not established. 22 In a case report describing the periscope graft technique, 24 a low-flow Type 2 endoleak was observed on angiography and manometry but was not treated given stable haemodynamics. It was unclear whether the endoleak was treated successfully. Based on the aforementioned, the technical success rate was 82% taking into account two patients who suffered from Type 1 endoleaks.
Patient characteristics, stent characteristics and clinical outcomes.
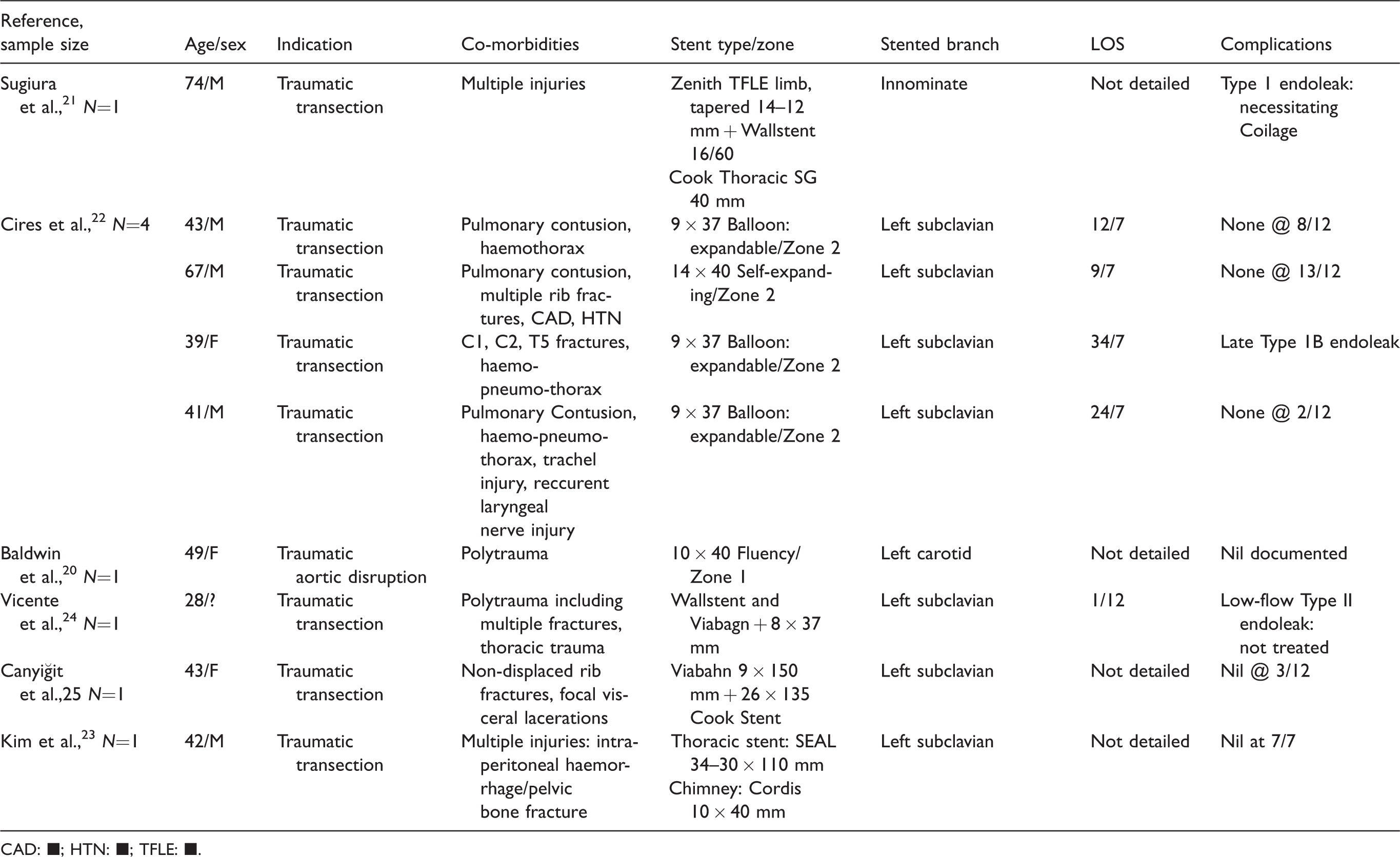
CAD: ■; HTN: ■; TFLE: ■.
No studies documented migration/compression/occlusion of chimney grafts through observation periods. Where documented, computed tomography (CT) was used as peri-operative imaging in order to visualise the degree of damage and extent of comorbidities.
Discussion
This systematic review of real-world evidence sought to investigate the efficacy of chimney grafts in patients with BTTAI. We concede the inherent limitations of this present review given the paucity of large and well-designed studies.
BTTAI is associated with a high mortality, previously quoted from 8–15% 26 up to 70–85% in others, 27 and it is the second most common cause of death following blunt mechanisms of injury. 28 Given the high surgical risk in this population, a minimally invasive technique is warranted. 29
We have identified a variation in the coverage of thoracic blood vessels, with the LSA most commonly covered. Although it is mostly germane to cover LSA, it also occurs rarely with the left carotid artery and even more rarely with the innominate artery, both of which were identified in our review. Coverage of these vessels requires adjunct procedures to maintain perfusion to the brachiocephalic vasculature. Surgical debranching in both open repair and hybrid procedures carries significant risks and burden associated with sternotomy, and is heightened in patients with comorbidities or previous cardiac surgeries. It is evident from our findings that surgical debranching was not performed in any patients, unsurprisingly given the emergent setting coupled with high surgical risks from polytrauma. Deployment of fenestrated grafts has been reported, but is limited by their availability especially in an emergent setting. Baldwin et al. first successfully reported the double-barrel stent technique to maintain patency of aortic arch vessels whilst reducing the need for surgical debranching procedures. 20 Since then, other techniques have emerged, including placement of a bare metal stent between the endograft and aortic wall combined with balloon angioplasty 30 to restore antegrade flow and pressure.
Specific guidelines have not been spelled out to encourage the use of chimney grafts for the repair of BTTAI, which accounts for the low number of cases reported in the literature. Hence, the findings from this review must be interpreted with prudence.
Spinal cord ischaemia remains a devastating complication of thoracic and thoraco-abdominal aortic repairs and as yet, the endovascular revolution has not blunted this risk. Fortunately, there were no complications associated with LSA coverage and stroke in this study, both of which ranks higher in the priority of concerns associated with chimney graft technique in the BTTAI setting. We now know that the development of spinal cord ischaemia following thoracic stenting is related to a number of different factors including but not limited to: length of aortic coverage, previous infrarenal aortic repairs and LSA coverage. Current strategies to mitigate this risk include judicious use of spinal drains, maintenance of a stable mean arterial pressure intra-operatively, staging the procedure if possible as well as left subclavian revascularisation. Therein exist other methods that aim to preserve the LSA. The combination of TEVAR with in situ graft fenestration (ISF) has been described in the literature, often employed as a bail-out option after unintentional coverage of the LSA, where a laser catheter is advanced through the LSA to fenestrate the graft and subsequent dilatation is performed on the fenestration with an iCast stent.31,32 Although it might be interesting to perform a comparative analysis of chimney grafts and ISF, there is evidently a paucity of studies, with sporadic case reports and series reporting the use of ISF in a BTTAI setting,33,34 much less so for comparative studies. This remains a knowledge gap, which future cohort studies should attempt to address. Nonetheless, our findings seem to be comparable to a recent systematic review of ISF, which reported a technical success rate of 93%; however, only one case of BTTAI was included in that study, hence permitting any meaningful comparison. 34
Advancements in techniques should be accompanied by developments in chimney-specific grafts; one such example is the Medtronic thoracic graft combined with long self-expanding parallel grafts. 35
When comparing our data to previous studies, they demonstrate a similar average age of 41 and mean hospital stay of 21 vs. 23 days. 28 Moreover, in those where pre-procedure imaging was recorded, CT scanning was employed, which is recognised as the imaging of choice in this setting. 36 Despite a high success rate, endoleak rates were significantly high, coupled with prolonged hospital stay, and thus we can hardly conclude that this may be a sound, non-invasive, successful technique for management of BTTAI. Nevertheless, bearing in mind the small sample size in our study, any conclusion cannot yet be established until larger cohort studies of BTTAI are published.
However, our results are comparable to a meta-analysis on chimney graft technique for aortic arch pathologies, with a pooled technical success rate of 91%. 37 The frequency of endoleaks was comparable to previously reported figures 38 ; however, we acknowledge that an endoleak which may be tolerable in an elective aneurysm setting may not be so in a BTTAI. Although the endoleak resolved spontaneously in one patient, it does not allow for a firm conclusion on whether this is the expected sequela in all untreated endoleaks. Nonetheless, endoleaks – particularly Type 1A – has often been described as the Archilles’ heel of the chimney graft technique, often due to ‘gutter’ formation, which are channels forming between the chimney graft and main aortic stent graft. This could also impede a good proximal seal leading to non-resolving endoleaks. 39 To prevent the formation of gutters, oversizing of the stent graft is necessary in order to allow for the main aortic body to surround the chimney. However, consensus surrounding the extent of oversizing has not been established, but some have recommended endograft oversizing by as much as 40%. 40 In vitro studies of two and three parallel-stent models have demonstrated improved endograft stent apposition when grafts were oversized by 30%; increased oversizing was associated with smaller gutters, albeit insignificant, but higher rates of infolding. 41 When faced with difficulty or uncertainty, surgeons can tap on precise geometric approximations to calculate the minimum main aortic graft diameter. 42 The panacea to preventing Type 1 endoleak is to create a minimum proximal neck length of 20 mm, and multiple authors have corroborated this dictum.43–45 This can be achieved by employing the periscope technique to extend the proximal seal zone as successfully reported by Vicente et al. 24 However, other factors must be considered, such as avoidance of bird-beaking along the lesser curve at the aortic apex, presence of atherosclerotic lesions and plaques within the arch. 45
As there are only nine patients in the study, the results of this review must be interpreted with caution bearing in mind the various inherent limitations. The inclusion of case reports negatively raises a significantly high risk of publication and selection bias. Penultimate of all, it is difficult to draw concretised conclusions from the analysis of only nine patients. This is aggravated by heterogeneity in reporting standards, particularly in defining key issues including: age, shock, time of stenting, degree of aortic curvature, calcium and thrombus, injury severity score; hence, we have not been able to obtain the aforementioned data due to overall poor reporting standards; this warrants the expeditious need for trauma-specific reporting guidelines. 46
Our recommendation is that in an emergency situation, when faced with a life-threatening BTTAI, coupled with an inadequate proximal landing zone with no scope to perform an open aortic arch debranching procedure, adjunctive chimney grafts provide a useful bail out strategy to maintain cerebral perfusion in normal and aberrant anatomy alike. Similarly, the scope of their use could be extended to revascularisation of the LSA in particularly high-risk patients such as those with dominant left vertebral arteries or previous infra-renal abdominal aortic aneurysm tube graft repairs.
Conclusion
Universal guidelines need to be developed to allow for definitive assessment of chimney graft techniques. Moreover, a multi-centre review of practice and outcomes would allow for true assessment of chimney graft efficacy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.