
Abstract
Objective
Peripheral artery disease is a major clinical co-morbidity that can significantly affect quality of life, especially in the presence of diabetes mellitus and older age. The focus of this literature review is on medical management, through anti-platelet and anti-coagulation, of peripheral artery disease prior to undergoing surgical or endovascular management.
Method
Extensive electronic literature search performed in four major databases (PubMed, SCOPUD, Embase and Ovid) to identify the published randomized and non-randomized studies that compared and discussed the management of peripheral artery disease with different anti-thrombotic agents.
Results
A total of 17 studies were identified to meet the inclusion criteria of this review. Among them, 4 were systematic review and meta-analyses, 1 was observational study and 12 were randomized controlled trials. The reported outcomes in each study are summarized and reported separately within this review.
Conclusion
Peripheral artery disease is a complex and multifactorial clinical condition. The use of dual anti-platelets, such as aspirin and clopidogrel, are the key in preventing major cardiovascular events as well as stroke and death. Utilization of anti-coagulation such as direct oral anti-coagulants’ as additional parameters for the prevention of disease progression, is paramount. Eventually, the choice of either dual-antiplatelet therapy or combined anti-coagulation with anti-platelets should be carefully considered, particularly following the most recent published debatable studies.
Introduction
Peripheral arterial disease (PAD) is commonly known by the pathogenic effects of atherosclerosis in the lower limb(s). There is a spectrum of clinical manifestation in the disease, ranging from patients with abnormal ankle-brachial pressure index (ABPI) readings who are completely asymptomatic, to those suffering with painful and debilitating limb ischaemia, sometimes requiring surgical intervention, or even amputation. 1 Over 200 million patients are estimated to suffer from the disease worldwide, with as many as 30% of over 70-year-olds afflicted in some way by the condition.1,2
Alongside the local atherosclerotic features in PAD, this patient cohort is also affected by arterial disease elsewhere; the most lethal outcomes being major acute cardiovascular events (MACE) such as myocardial infarction (MI) and stroke.3–5 This means those with PAD can carry a significant risk of morbidity and mortality likened to the increased risk of those with established coronary artery disease (CAD). 6
The management of PAD, as with CAD, is via risk assessment and reduction, to both limit the natural progression of the disease, and prevent adverse cardiovascular events. The cornerstone of which, is lifestyle intervention, such as diet modification, exercise regimes and smoking cessation. To complement this, pharmacological therapies are used to address specific atherosclerotic factors such as the effects of hypertension and hypercholesterolaemia, namely with angiotensin converting enzyme (ACE) inhibitors and statins, respectively. 7 However, where guidelines regarding antithrombotic treatment in CAD offer clear recommendations, this guidance is less transparent in the use of antiplatelet/anticoagulant in PAD. 6
Clinical guidelines in the United States (ACCF/AHA) and Europe (ESC/ESVS) recommend the use of single anti-platelet therapy (SAPT), namely low dose aspirin for anti-thrombotic therapy in PAD.7,8 However, sub-groups of larger studies have given therapeutic precedence to clopidogrel in certain patient cohorts 9 and studies exist elsewhere involving dual-antiplatelet therapy (DAPT), 10 direct oral anti-coagulants (DOACs) 11 and newer anti-platelet agents. 12 This conflicting evidence is further mystified by the fact that these studies are often set apart by involving different patient populations with varying ‘defined standards’ of PAD and a paucity of studies involving those with asymptomatic PAD.13,14
Furthermore, while the risk of adverse cardiovascular events is often seen as comparable between those with CAD and those with PAD, evidence suggests CAD versus non-CAD patients are at a 1.5–2× fold increased risk of MACE, compared to PAD versus non-PAD patients, where the risk is as high as 4–10× fold. 15 This may be due to a smaller proportion of PAD patients being actively managed compared to CAD, and adherence to therapy being poor in those with PAD. 2 This paper reviews the current available evidence of anti-platelet and anti-coagulant therapies in patients with PAD with the aim of shedding light on the optimum management of this demanding clinical burden.
Literature search methodology
An electronic literature search was performed in six major databases as PubMed, EMBASE, SCOPUS, Ovid, Google Scholar and Cochrane. The search keywords used were ‘peripheral arterial’ OR ‘vascular disease’ OR ‘antiplatelets’ OR ‘anticoagulation’ AND ‘single therapy’ OR ‘dual therapy’ OR ‘asymptomatic’. Inclusion criteria included randomized studies, and those that included patients whom had not undergone surgical/endovascular interventions. Articles that were case reports, general reviews, expert opinion, or exclusively post-surgical interventions were excluded, as they would not provide enough merit to be included in this review.
Current clinical guidelines
The European Societies of Cardiology (ESC) and Vascular Surgery (ESVS) provide joint guidance for the diagnosis and treatment of peripheral arterial diseases. Specific guidance for lower extremity PAD recommends long-term single anti-platelet therapy in those who have symptomatic PAD, have undergone revascularization or post infra-inguinal bypass surgery (evidence class/level = I/A). SAPT is not supported in those with asymptomatic PAD, due to a lack of evidence in this field (III/A). Importantly, clopidogrel may be supported as an alternative to aspirin as first-line SAPT, this uncertainty owing to conflicting evidence/opinion (IIb/B) and only in carotid artery disease is DAPT recommended for at least one month post-carotid artery surgery (I/B). 7
The use of OACs is indeed recommended in patients with concomitant PAD and atrial fibrillation (AF), if the CHA2DS2-VASc score is ≥2 (I/A). Beyond this recommendation, support for DOACs in PAD dwindles, specifically mentioning those with lower CHA2DS2-VASc scores (IIa/B), post-revascularization surgery (IIa/C) and long-term use of OACs with SAPT (IIb/C). 7
Joint American Heart Association (AHA) and American College of Cardiology (ACC) guidelines (2016) offer a slightly wider scope of anti-platelet treatment recommendations in PAD. In those with symptomatic PAD, both low dose aspirin (75–325 mg) and clopidogrel (75 mg) are supported as first line options for SAPT in this patient group (I/A). Additionally, there is ‘reasonable’ recommendation for the use of anti-platelet therapy in those who are asymptomatic with an ABPI of ≤0.90 (IIa/C-EO), albeit with ‘uncertain usefulness’ in asymptomatic patients with ABPI above this value (IIb/B-R). Beyond these recommendations however, guidance mirrors that of European Societies, with less support for DAPT (IIb/B-R) and OACs (III: Harm/A) in PAD. 8
It is evident that beyond the use of SAPT, namely with aspirin, in symptomatic PAD, there is no concrete or universal support in European, UK or US guidelines for the vast alternative range of anti-platelet and/or anti-coagulation combination options currently available. There are several trials and studies that compare the use of different agents in PAD. Table 1 provides a summary of the main studies found in the literature relating to this topic.
Summary of the studies and trials the compares the use of anti-platelets and anti-coagulations and their reported outcomes.

*The original total cohort of the randomized controlled trial was 240 patients, however results from only 199 patients were analysed as they were the only ones that met the trial protocol.
Atherosclerosis and platelets in PAD
The preventative and symptomatic medical treatments that are offered for PAD are centred on its complex pathogenesis, with a large focus being on anti-platelet medication, as platelets play a pivotal role in the formation and rupture of atherosclerotic plaques. The intact arterial endothelium produces an abundance of substances including nitric oxide (NO) and prostacyclin, both potent inhibitors of platelet aggregation. 16 When this endothelium is damaged, the sub-endothelium is exposed. This now vulnerable, un-inhibited surface is in immediate contact with the contents of the lumen, including monocytes, lipids and platelets. 17 This results in atheroma formation, leading to stenotic arteries and to the symptoms and sequelae of peripheral arterial disease when occurring in the lower limbs.
Platelets are most deadly when the atherosclerotic plaque surface ruptures, activating the clotting cascade as well as encouraging more platelets to adhere to the already damaged arterial wall, eventually leading to thrombus formation and occlusion of the vessel. This is a key target in the medical management and prevention/progression of PAD and MACE. There are multiple pharmacotherapies currently available to prevent platelet aggregation/activation and thrombus formation. These pharmacotherapies and their mechanisms of action are summarized in Table 2 and Figure 1.
Mechanism of action of anti-platelets and anti-coagulants.
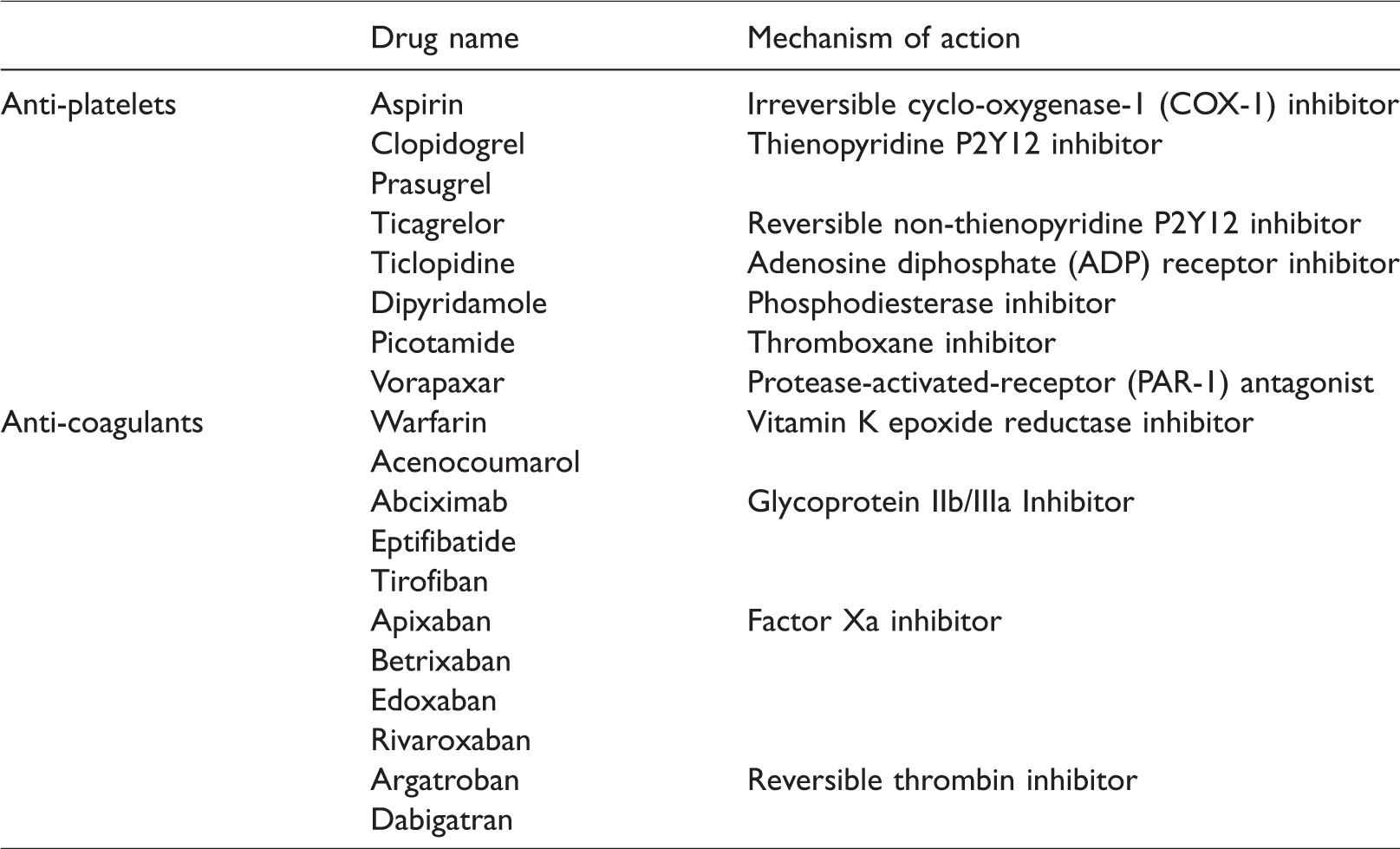
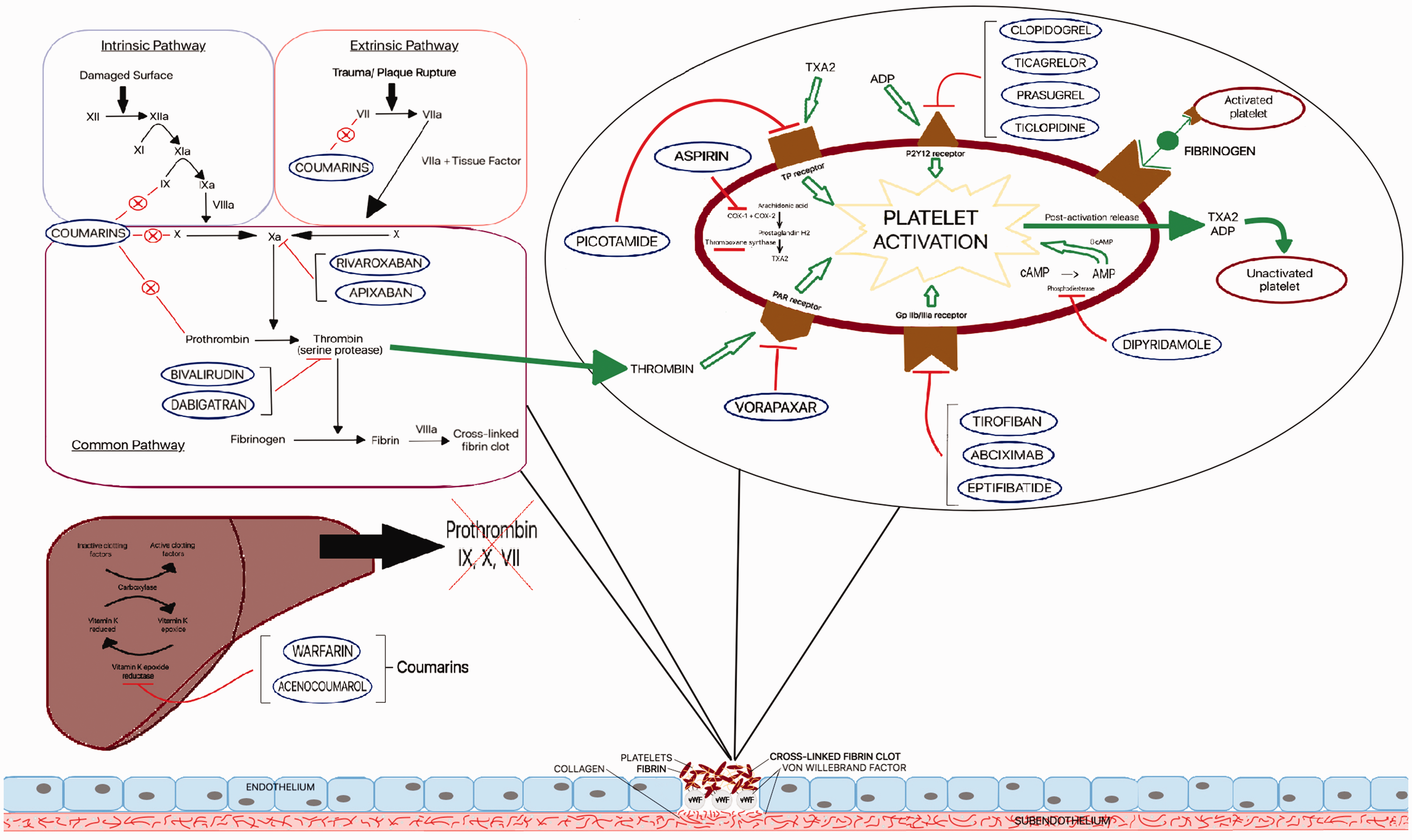
Mechanism of action.
Which anti-platelets to use?
Patients with established PAD have a six times higher risk of cerebrovascular and cardiovascular events within 10 years than non-PAD patients. 18 Therefore, prevention of such life-threatening emergencies is crucial to provide stable management of this condition. Antiplatelets, to date, play an important and crucial role in reducing such risks, whilst stabilizing clinical symptoms and status of PAD in the long-term. 19
Aspirin
Aspirin became one of the very first anti-platelet agents used in patients with peripheral vascular disease. Despite innovation of new anti-platelet agents, it is counted as one of the most potent and safe medications to be used in patients with PAD.7,8 However, the effectiveness of aspirin in preventing clinical emergencies is a topic that is debated among international platforms with often controversial supporting evidence. 20
Initially described as acetyl salicylic acid (ASA), aspirin was first synthesized by Felix Hoffman in Germany in 1897. 21 It was in 1971 when its mechanism of action was revealed: aspirin irreversibly inhibits the activity of the cyclooxygenase-1 (COX-1) enzyme. Thromboxane A2 (TXA2) and prostaglandins also play a role in platelet activation and aggregation. They are both derived from the same precursor, arachidonic acid. Cyclooxygenase-1 catalyses the conversion of arachidonic acid to certain prostaglandins, and with the aid of thromboxane synthase, produce TXA2. Thus, inhibition of COX-1 leads to decreased platelet activation and aggregation by reducing the formation of these prostaglandins and TXA2 from arachidonic acid. 22
The use of aspirin has been supported and contradicted in many studies; it is a mainstay medication in cardiovascular disease management and prevention, however, with newer generations of anti-platelets which potentially offer greater potency, efficacy and safety, this remains controversial. 12 There is no doubting the benefit of aspirin as a secondary prevention treatment in patients with atherosclerosis and prior ischaemic stroke or acute myocardial infarction. 23 In addition to this, researchers have tried through several randomized controlled trials (RCTs) to identify the role of aspirin as primary prevention therapy in PAD patients. In a randomized controlled trial by Fowkes et al. 13 of 3350 patients who had established PAD with ABPI of ≤0.95 but were asymptomatic, aspirin had not resulted in a reduction of vascular events when compared to placebo or non-aspiring taking patients. Similarly, in an earlier RCT by Belch et al. 14 of 1276 patients who had diabetes mellitus and asymptomatic PAD, the authors reported no significant difference in the rate of fatal coronary heart disease or stroke between patients that received aspirin and those who did not (18.2% vs. 18.3%, respectively): hazard ratio 0.98 (95% confidence interval (CI): 0.76–1.26). Therefore, they concluded that aspirin has no role in primary prevention and reducing the rate of cardiovascular events or mortality in patients who have diabetes mellitus and established PAD but are asymptomatic.
There have been different studies and trials in patients that have initially presented with symptomatic PAD rather than complications associated with PAD. Among the key studies is the double blinded RCT from the critical leg ischaemia study (CLIPS) group, 24 in which they randomized 366 patients that had established PAD. The results showed a higher rate of major vascular events among the placebo group versus aspirin receiving patients (11% vs. 3.78%, respectively, p = 0.022) and similarly, a higher rate of critical limb ischaemia (4.4% vs. 2.7%, respectively, p = 0.014). The conclusion from their study suggested a reduction in the incidence of vascular events by 26% when using low-dose aspirin in patients with PAD and type 2 diabetes mellitus. This study was supported by an earlier RCT by Hess et al. 25 in 1985, where 240 patients were randomized into three groups: aspirin alone, aspirin and dipyridamole, and placebo. Over the period of 2 years, patients treated by aspirin alone showed less disease progression and worsening of PAD than those who were treated with placebo. Furthermore, patients who smoked and those with hypertension were the most beneficial group of cohorts from such treatment.
A systematic review and meta-analysis of randomized trials by Berger et al. 26 analysed 18 studies with a total of 5269 patients, showed that cardiovascular events arose in 8.2% versus 9.6% in patients taking aspirin versus placebo, respectively (pooled relative risk (RR): 0.75; 95% CI: 0.48–1.18). A significant reduction in nonfatal stroke was noted with aspirin (2.1% vs. 3.4%; RR: 0.64; 95% CI: 0.42–0.99), but no statistically significant reductions in all-cause or cardiovascular mortality, MI, or major bleeding.
Finally, in a more recent systematic review and meta-analysis of randomized trials by Mahmoud et al., 23 the authors reviewed outcomes in 6560 patients from 11 recent RCT’s. The primary endpoint was all-cause mortality while the primary safety outcome was major bleeding. Further reported outcomes included major adverse cardiac and cerebrovascular events (MACCE), myocardial infarction (MI), stroke and intracranial haemorrhage. Their results also showed that aspirin was associated with a similar rate of all-cause mortality (RR = 0.93, 95% CI = 0.8–1.1), MACCE (RR = 1.0, 95% CI = 0.83–1.20), MI (RR = 0.91, 95% CI = 0.67–1.23) and stroke (RR = 0.72, 95% CI = 0.43–1.22), major bleeding (RR = 1.59, 95% CI = 0.96–2.62) and intracranial haemorrhage (RR = 1.38, 95% CI = 0.59–3.21). Therefore, they ultimately concluded that the use of aspirin does not improve cardiovascular outcomes or worsen reported bleeding, and therefore its use is limited.
Adenosine diphosphate receptor antagonists (P2Y12 inhibitors)
Clopidogrel
Clopidogrel is an adenosine diphosphate (ADP) receptor antagonist, also known as a P2Y12 inhibitor. This class can also be subclassified into thienopyridines (such clopidogrel and prasugrel) and the nonthienopyridines (such as ticagrelor). Clopidogrel works by inhibiting the interaction between ADP and the platelet P2Y12 receptor. This receptor plays a key role in stimulating the activation of the glycoprotein IIb/IIIa (GP IIb/IIIa) receptors. These, when activated, produce TXA2 and encourage platelet aggregation. Thus, their down regulation has an anti-platelet and anti-aggregation affect.27,28 The very first study that supported the use of clopidogrel in clinical practice for PAD was clopidogrel versus aspirin in the patients at risk of ischaemic events (CAPRIE) trial in 1996. 9 This study was a well-designed RCT that compared the efficacy of clopidogrel (75 mg once daily) against aspirin (325 mg once daily) in patients with PAD who were at a high risk of an ischaemic event. The study included 19,185 patients (who had either recent myocardial infarction (MI), recent ischaemic stroke or symptomatic PAD), who were followed over 1–3 years with mean follow-up of 1.9 years. The primary endpoints were ischaemic stroke, MI or death from vascular cause. The analysis showed a statistically significant 8.7% RR reduction (p = 0.043; 95% CI: 0.3–16.5) in the composite endpoint of MI, stroke and vascular death in the clopidogrel group. In a further subgroup analysis of the PAD population that were included in the study, the average event rate per year was 3.71% in the clopidogrel arm compared to 4.86% in the aspirin arm, resulting in a 23.8% RR reduction (p = 0.0028; 95% CI: 8.9–36.2) and thus, confirmed its usefulness in this cohort.
However, despite such positive evidence being reported, there are many limitations in using clopidogrel such as developing clopidogrel resistance, which can be affected by many risk factors as diabetes, smoking and chronic kidney disease.29–31 This limitation does not respond to increases of dose to 150 mg per day, and it is deemed ineffective in these circumstances. 32 In such cases, a stronger anti-platelet option is advised. Although, clopidogrel is still considered one of the most useful medical therapy options, there are no further reported studies comparing clopidogrel alone or versus aspirin, but rather studies published of comparing clopidogrel against other P2Y12 inhibitors.
Ticagrelor
Ticagrelor is another P2Y12 inhibitor; it is reversible and belongs to the nonthienopyridines group of ADP receptor antagonists. The role of ticagrelor in cardiovascular disease therapy became more evident when it was used in patients with acute coronary syndrome (ACS), where it was proven that ticagrelor is more beneficial than clopidogrel in patients with ACS. 33 However, this fact was not fully explored in patients with PAD until the recently reported RCT of Effects of Ticagrelor and Clopidogrel in Patients with Peripheral Artery Disease (EUCLID) 34 and later reported by Hiatt et al. 35 The EUCLID trial compared outcomes in using ticagrelor versus clopidogrel in a total of 13,885 patients with symptomatic PAD. Ticagrelor was used at a dose of 90 mg twice a day in 6930 patients while clopidogrel was used at a dose of 75 mg once a day in 6955 patients in a multi-centre, international, parallel blinded study. The primary outcomes were cardiovascular death, MI or ischaemic stroke. Other outcomes included were acute limb ischaemia, need for revascularization, overall disease progression and quality of life. Among both groups, there were no statistically significant differences in the primary outcomes (10.8% receiving ticagrelor versus 10.6% receiving clopidogrel, hazard ratio, 1.02; 95% CI: 0.92–1.13; p = 0.65). Additionally, there was no significant difference in the rate of acute limb ischaemia (1.7% of the patients, hazard ratio (HR) = 1.03; 95% CI = 0.79–1.33; p = 0.85), and major bleeding occurred in 1.6% of the entire cohort (HR = 1.10; 95% CI = 0.84–1.43; p = 0.49). However, it was clear from the subset of the data that ischaemic stroke was higher in patients that received clopidogrel (2.4%) than those who received ticagrelor (1.9%, HR = 0.78, 95% CI = 0.62–0.98, p = 0.03). Nevertheless, the ultimate outcomes from the RCT was a non-superiority of ticagrelor to clopidogrel in reducing major cardiovascular events, and it showed similar bleeding risks that is comparable to clopidogrel.
Other anti-platelets being used in PAD patients
Vorapaxar
As a protease activator receptor-1 (PAR-1) antagonist, vorapaxar functions by inhibiting the interaction of thrombin with the PAR-1 receptor, thus inhibiting platelet aggregation. The main study that reported vorapaxar’s use in this capacity is the Thrombin Receptor Antagonist in Secondary Prevention of Atherothrombotic Ischemic Events-Thrombolysis in Myocardial Infarction 50 (TRA 2P-TIMI 50) trial, 36 which was a double blinded placebo-controlled trial, evaluating vorapaxar for the secondary prevention of atherothrombosis in 26,449 patients. The primary endpoint included a composite of cardiovascular death, MI or stroke. The principal safety endpoint was bleeding, with the study utilizing the Global Utilization of Streptokinase and t-PA for Occluded Coronary Arteries (GUSTO) criteria.
In the PAD cohort, there was no significant difference in the rates of cardiovascular death, MI or stroke (11.3% vs. 11.9%; HR = 0.94; 95% CI = 0.78–1.14; p = 0.53). However, the vorapaxar group of patients showed a significant reduction in limb ischaemic events (vorapaxar 2.3% vs. placebo 3.9%; HR = 0.58; 95% CI = 0.39–0.86; p = 0.006) and the need for peripheral artery revascularization (vorapaxar 18.4% vs. placebo 22.2%; HR = 0.84; 95% CI: 0.73–0.97; p = 0.017). Bleeding occurred more frequently with vorapaxar compared with placebo (7.4% vs. 4.5%; HR = 1.62; 95% CI = 1.21–2.18; p = 0.001).
However, a subset analysis of patients for assessing for occurrence of acute limb ischaemia (ALI) showed that Vorapaxar reduced first ALI events by 41% (HR = 0.58; 95% CI = 0.39–0.86; p = 0.006) and reduced total ALI events by 41% (94 vs. 56 events; risk ratio = 0.59; 95% CI = 0.38–0.93; p = 0.022). 37
Picotamide
Picotamide, a derivative of methoxy-isophtalic acid, is an antiplatelet drug whose pharmacological properties consist mainly of inhibiting both thromboxane receptors and TXA2 synthase, thereby reducing platelet aggregation. 38 In contrast to aspirin, it does not affect cyclooxygenase activity. Utilization and assessment of the use of picotamide in PAD patients has been performed in two major trials. The first trial was by Balsano et al. through the ADEP trial 39 in which a total of 2,304 patients with PAD were randomly allocated through a double-blind, placebo-controlled study into receiving either picotamide 300 mg three times a day or placebo, with further follow-up for 18 months. Some of the key analysed events during the follow up period were cardiovascular death, MI, stroke, or amputation, while less serious events were also analysed, in the form of unstable angina, transient ischaemic attack, renal failure, and peripheral vascular disease deterioration. Their results showed a statistically borderline significance when comparing total major and minor events between both groups in the ‘intention-to-treat’ stage (risk reduction = 18.9%; p = 0.056, log-rank test). However, this was much more significant in the ‘on-treatment’ stage of the study in which there were much less major and minor events in picotamide receiving patients (3.8% vs. 4.2% and 6.3% vs. 8.9%, respectively, risk reduction, 23%; p = 0.029, log-rank test). A further subgroup analysis of 438 patients with diabetes mellitus showed a 45.2% RR reduction in the combined outcomes of major and minor cardiovascular events that was statistically significant between both cohorts (p = 0.022). Therefore, picotamide was considered as a relatively safe medicine that reduces cardiovascular complications in patients with PAD.
The second study that has assessed the use of picotamide is the DAVID trial. 40 This was a multi-centre, randomized, double blinded controlled trial that compared the use of aspirin vs. picotamide for the prevention of major cardiovascular events and mortality in patients with established PAD and diabetes. The study enrolled 1209 patients to receive either picotamide 600 mg twice a day or aspirin 320 mg once a day over a period of 2 years. The mortality rate was significantly lower in picotamide treated group of patients (3% vs. 5.5%, 95% CI = 0.31–0.98%) with a RR reduction of 45% and 2.5% absolute risk reduction in 2 years. However, the combined endpoint of mortality and morbidity had a slightly lower incidence in the picotamide group, but this did not reach statistical significance. It is worth noting that the incidence of gastrointestinal bleeding was lower in the picotamide treated group. Nevertheless, the rates of vascular mortality or major ischaemic cardiovascular events were not reduced by picotamide when compared with aspirin use, and thus the study limits itself in the reported outcomes. These outcomes are possibly the result of the bias due to the high proportion of patients (about 20% in each group) who left the study because of non-fatal events, which may have underestimated the real incidence of the secondary endpoints. Additionally, it is possible that the sample size of the study was insufficient to detect any difference in these endpoints between the two groups.
Overall, the data from these two trials remain controversial and debatable. Although the use of picotamide in patients with PAD is demonstrated as useful, especially in the presence of type 2 diabetes mellitus, it’s superiority in terms of preventing cardiovascular death, acute MI and ischaemic stroke remains unclear. Thus, a larger scale randomized trial is of critical use to determine the overall benefit of using picotamide over aspirin.
Monotherapy or dual antiplatelet therapy
It has been just under a decade since the use of two anti-platelets simultaneously have been explored through randomized controlled trials in patients with established PAD. 41 Several studies have shown that dual anti-platelet therapy (DAPT) over single anti-platelet therapy (SAPT) is more beneficial and can reduce the rate of ischaemic vascular events, however this comes at the expense of increased risk of bleeding and other potential side effects.10,42,43
There have been several randomized controlled and observational studies comparing the outcomes in patients with PAD in using SAPT or DAPT. In a post hoc analysis of 3096 patients that were involved in the CHARISMA trial by Cacoub et al., 41 the authors compared the use of clopidogrel and aspirin versus aspirin alone in patients with established PAD (symptomatic or asymptomatic) but received only medical management. The primary endpoints were rate of cardiovascular death, acute MI or stroke. These events were noted at a higher rate in patients with aspirin only, but did not reach statistical significance (HR = 0.85; 95% CI = 0.66–1.08; p = 0.18). In subset and isolated event analysis, it was noted that the MI rate was higher in the aspirin alone group, 3.7% compared to 2.3%, respectively (HR = 0.63; 95% CI = 0.42–0.96; p = 0.029), similar outcomes were reported for the rate of hospital admissions for ischaemic events (16.5% vs. 20.1%, respectively, HR = 0.81; 95% CI = 0.68–0.95; p = 0.011). Furthermore, the rate of moderate-severe bleeding did not differ significantly between the treatment groups, however the rate of minor bleeding was higher in the DAPT group 34.4% vs. 20.8% (odds ratio = 1.99; 95% CI = 1.69–2.34; p < 0.001). Hence, the reported outcomes from this study favour the use of DAPT over SAPT in patients with PAD for providing lower cardiovascular events, at the expense of a slight increase in chances of minor bleeding.
A further retrospective observational study by Armstrong et al. 44 compared the effect of DAPT (aspirin and clopidogrel) versus aspirin alone in patients with established and symptomatic PAD. A total of 629 patients were involved in the analysis, they either had claudication or critical limb ischaemia and the duration of assessment was 3 years, with endpoints of major cardiovascular adverse and limb events. The sample of patients that were taking DAPT was much larger than aspirin alone (n = 348 vs. n = 281, respectively). There was higher rate of adverse events in total in the aspirin group (29% vs. 20%), this was adjusted with propensity matching of the included patients and yet, DAPT showed lower rates of major cardiovascular events and mortality rates than aspirin alone (HR = 0.65; 95% CI = 0.44–0.96, and HR = 0.55; 95% CI = 0.35–0.89, respectively). Based on the reported outcomes from their study, DAPT seems to be associated with lower major cardiovascular events and mortality rates in patients with symptomatic PAD.
Since the above two studies, there have been several high-level evidence studies in the form of systematic review and meta-analysis aiming to understand the use of DAPT over SAPT in patients with PAD. The latest of which, by Beiswenger et al., 45 reviewed 14 studies in their analysis, 10 of which were RCT’s and 4 were observational studies. A total of 6276 patients were analysed, 3134 in DAPT and 3142 in SAPT group. The endpoints were major adverse cardiovascular events (MACEs), major adverse cardiovascular and cerebrovascular events (MACCEs), major adverse limb events (MALEs) and mortality rates or survival rates were reported appropriately. The pooled rates of MACEs were significantly lower in patients receiving DAPT (RR = 0.79; 95% CI = 0.68–0.91, p = 0.002), similarly, the rate of MALEs was much lower in the DAPT cohort, but this didn’t reach statistical significance (RR = 0.70; 95% CI = 0.49–1.01, p = 0.06). This was probably and largely affected by the extreme heterogeneity in one of the included studies (I2 = 69%), therefore it must be interpreted with caution. Furthermore, the results from the 8 included studies showed much lower mortality rates in the DAPT cohort patients with PAD (RR = 0.57; 95% CI = 0.45–0.72, p < 0.00001). Additionally, the use of DAPT did not increase the rate of major, severe or fatal bleeding rates among the cohort (RR = 0.98; 95% CI = 0.68–1.41, p = 0.92). Therefore, the analysis of MACEs, MALEs and mortality rates from the included study suggest that using DAPT is superior to SAPT in symptomatic PAD patients and therefore should be encouraged.
In another systematic review and meta-analysis by Navarese et al., 46 the authors identified 10 studies with a total of 65,983 patients to be included in their study. However, the key disadvantage in this study is the overlap with most of the studies that were included in the study by Beiswenger et al., having been published within a very similar timeframe. Nevertheless, they have noted a significant reduction in mortality rate (11%) in DAPT group of patients and overall, a lesser mortality rate (21.59% vs. 22.69%, RR [95% CI] = 0.89 [0.86–0.92]; p < 0.001; I2 = 0%). Patients that received DAPT had a lower rate of limb revascularization (10.16% vs. 13.18%; RR [95% CI] = 0.80 [0.69–0.92]; p = 0.002; I2 = 6%). Interestingly, there was no difference in the rate of myocardial infarction between DAPT and SAPT patients (RR [95% CI] = 1.08 [0.71–1.63]; p = 0.72; I2 = 83%). Finally, although the rate of major adverse bleeding was higher in DAPT patients, this didn’t reach statistical significance (RR [95% CI]: 1.21 [0.87–1.68]; p = 0.26; I2 = 0%). Based on those significant findings, DAPT should be considered in patients with symptomatic PAD as it provides better outcomes when compared with aspirin alone. The ideal choice would be aspirin and another anti-platelet agent as the mainstay of antiplatelet therapy in such a high-risk cohort of patients.
All these findings were also supported by an unpublished recent systematic review and meta-analysis by Petrescu et al. 47 reporting supremacy of DAPT over SAPT, and the use of aspirin with a second anti-platelet should be considered as the therapeutic gold-standard in patients with PAD, regardless of whether they undergo invasive revascularization or not.
Role of anti-coagulation therapy in PAD patients
Anti-coagulant therapies have also been explored in patients with PAD, however its beneficial role in this cohort of patients has been debated due to the high-risk of bleeding, as well as doubts over safety and efficacy. Patients with established PAD have a higher level of circulating tissue factor, exaggerated thrombin production, and further reduced fibrinolytic potential when compared to healthy individuals, and this is consistent with possible underlying prothrombin status.48,49
There are two major types of anti-coagulants that are currently involved in managing patients with PAD. The first are vitamin K epoxide reductase inhibitors, namely Warfarin, and the second are directly acting oral anticoagulant agents (DOAC). These include the direct thrombin inhibitor, dabigatran, and factor Xa inhibitors, namely apixaban, edoxaban and rivaroxaban (among others).
The main study that elaborated the role of vitamin K antagonists in patients with PAD was the Warfarin Antiplatelets Vascular Evaluation (WAVE) trial. 50 This study was a randomized controlled study that enrolled 2161 patients and randomized them into either receiving anti-coagulation with an anti-platelet, or anti-platelets alone. The mean follow-up was 35 months for the cohort of patients. The key primary outcomes were MI, stroke or death from cardiovascular events. The results from the study have shown that the use of combination therapy with anti-coagulation was no better at preventing major cardiovascular complications than antiplatelet therapy alone (combination therapy group 12.2% and antiplatelet therapy alone 13.3%; 95% CI = 0.73–1.16; p = 0.48). Additionally, the secondary endpoints of MI, stroke, severe ischaemia of the coronary or peripheral arteries, or death from cardiovascular causes did not differ significantly between treatment groups (15.9% in the combination therapy group vs. 17.4% in the antiplatelet monotherapy group; HR = 0.91, 95% CI = 0.74–1.12; p = 0.37). Also, the combination therapy was associated with a significantly higher incidence of life-threatening bleeding (4.0% vs. 1.2%; 95% CI = 1.84–6.35; p < 0.001) and moderate bleeding (2.9% vs. 1.0%; 95% CI: 1.43–5.58; p = 0.002). Hence, this study determined that adding a vitamin K epoxide reductase inhibitor into the treatment regime of a patient with PAD, does not add any further effectiveness than anti-platelets alone, but rather it increases the risk of life-threatening bleeding.
Recent advances in anticoagulant therapy
As for DOAC therapy medications in patients with PAD, there have been very recent advances in using such therapy from the Cardiovascular Outcomes for People Using Anticoagulation Strategies (COMPASS) trial. 51 The study comprised of a multi-centre, double-blind, randomized placebo-controlled trial over 602 clinical sites across 33 countries, involving 27,395 patients with stable atherosclerotic vascular disease. These participants were randomized into three main groups of either (1) 2.5 mg of rivaroxaban twice-daily plus aspirin 100 mg daily, (2) 5 mg rivaroxaban twice-daily monotherapy or (3) aspirin 100 mg once daily monotherapy. The primary endpoints were cardiovascular death, stroke or myocardial infarction. The trial was terminated early due to its satisfaction by the investigators and superiority of rivaroxaban plus aspirin group over aspirin alone after a mean follow up of 23 months. The rates of primary adverse outcomes were higher in aspirin alone group compared with rivaroxaban plus aspirin patients (5.4% vs. 4.1%, HR = 0.76; 95% CI = 0.66–0.86; p < 0.001; z = −4.126). Unsurprisingly, major bleeding complications were higher in the combined therapy group than aspirin alone (3.1% vs. 1.9%; HR = 1.70; 95% CI = 1.40–2.05; p < 0.001). However, the authors highlight there were no differences in fatal or critical organ bleeds between the groups. It is also worth noting that mortality rates were higher in the aspirin alone group compared to combined therapy (4.1% vs. 3.4%, HR = 0.82; 95% CI = 0.71–0.96; p = 0.01; threshold p value for significance = 0.0025). In conclusion, the study supported the use of a DOAC with aspirin as it provides better cardiovascular outcomes at the expense of an increased risk of major bleeding.
Anand et al. 52 later published a sub-group analysis of patients with PAD in the COMPASS trial. A total of 7470 patients with a median duration of treatment of 21 months were included in the analysis. The primary composite endpoint was cardiovascular death, myocardial infarction, or stroke. Patients in the combination therapy group had a lower rate of such complications when compared with aspirin alone group (5% vs. 7%; HR = 0.72, 95% CI = 0.57–0.90, p = 0.0047). Similarly, there were also lower rates of major adverse limb events including major amputation (1% vs. 2%; HR = 0.54, 95% CI = 0.35–0.82, p = 0·0037). As with the full COMPASS trial, patients in the combination therapy group had higher rates of major bleeding compared to aspirin alone, which was mainly gastrointestinal, 3% vs. 2%; HR = 1·61, 95% CI = 1.12–2.31, p = 0·0089), but again, there were no differences in fatal and critical organ bleeds. It is worth noting that the COMPASS and sub-group analysis both demonstrated favourable outcomes with a combined therapy regime, not only compared to aspirin alone, but also to singular rivaroxaban therapy, suggesting an additive effect of DOAC and antiplatelet therapy.51,52 In addition to this, a further lower limb PAD sub-group analysis investigated the effect of this combination versus aspirin alone on lower limb PAD complications, whereby, once more, the rivaroxaban combination demonstrated better rates of MALE, amputations and other vascular interventions individually p = 0.01, p = 0.02, p = 0.03, respectively and indeed in total outcomes (HR = 0.76, 95% CI = 0.61–0.96, p = 0.02). 53
Thus, again, this evidence suggests that combined DOAC therapy has a positive role in reducing major adverse cardiovascular events when compared to aspirin alone, not only in stable cardiovascular disease, but specifically to those with PAD, however this comes with a higher chance of gastrointestinal bleeding.37,52
Understandably, the COMPASS trial has given clinicians a new perspective on the potential benefits of combined low-dose DOAC and aspirin therapy in preventing MACE events in patients with cardiovascular disease, having been praised widely at its presentation at the European Society of Cardiology 2017 Congress and published in some of the field’s most prestigious journals thereafter. Having said that, the study is not without criticisms. While the COMPASS authors report a positive net benefit-risk analysis, others highlight that this analysis did not include the primary safety end-point of major bleeding. Further concerns are raised over the less impressive outcome of number needed to treat (NNT) of 76 and the potential expense and challenge of mass prescribing an expensive drug like rivaroxaban. Clinicians and guidelines, as always need to take these factors into account when handling new evidence, however overall there is no denying the potential impact the COMPASS study may have on the management of cardiovascular, and indeed, peripheral arterial disease.
Conclusion
PAD is a complex and multifactorial clinical condition. The use of dual anti-platelets, such as aspirin and clopidogrel, are the key in preventing major cardiovascular events as well as stroke and death. Utilization of anti-coagulation such as DOAC’s as additional parameters for the prevention of disease progression, is paramount. Eventually, the choice of either DAPT or combined anti-coagulation with anti-platelets should be carefully considered, particularly following the most recent published debatable studies.
Supplemental Material
Supplemental material for Anti-platelet and anti-coagulant therapy in peripheral arterial disease prior to surgical intervention
Supplemental Material for Anti-platelet and anti-coagulant therapy in peripheral arterial disease prior to surgical intervention by Amer Harky, Perry Maskell and Mika Burgess in Vascular
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.