
Abstract
Objectives
The frequency and implications of peripheral artery disease (PAD) in some risk groups are not entirely characterized in Latin America. We studied PAD prevalence, risk factors, and six-month outcomes in stable outpatients with a history of a recent acute coronary syndrome (ACS), or at high coronary risk.
Methods
We recruited 830 outpatients in 43 Mexican sites (median age: 64.8 years; 57.8% men). Inclusion criteria were age >18 years, and ACS within 30 days, or age <55 years plus ≥2 major vascular risk factors, or age ≥55 years plus ≥1 vascular risk factors. Patients received standardized assessments at baseline and six-month follow-up for medical history, ankle-brachial index (ABI), and the Edinburgh Claudication Questionnaire (ECQ).
Results
ABI <0.8 was found in 10.5%, <0.9 in 22.5%, >1.3 in 4.8%, and >1.4 in 3.6%, without differences according to sex or selection criteria. Positive ECQ was found in 7.6%. ABI <0.9 was directly associated with age, diabetes, ACS, and chronic kidney disease, but inversely associated with BMI >27. The six-month case-fatality and atherothrombotic events rates were 1.6% and 3.6%, respectively. In patients with ABI <0.9 and ABI <0.8, the six-month case-fatality rates were 2.5% (p = 0.27) and 5.4% (p = 0.03), respectively. In a Cox proportional-hazards model, baseline factors associated with death were age ≥65, ABI <0.8, and ACS.
Conclusions
Subclinical PAD is more common than symptomatic claudication in high-risk coronary outpatients. Low ABI is associated with reduced short-term survival in patients with recent ACS or at high coronary risk.
Keywords
Introduction
Along with coronary artery disease (CAD) and cerebrovascular disease (CVD), significant atherosclerosis of the lower limbs, known as peripheral artery disease (PAD), represents a major form of chronic atherothrombosis leading to increased morbidity and mortality worldwide.1,2 Although PAD is erroneously considered a condition with a relatively benign prognosis, a significant proportion of patients with either symptomatic (i.e. with claudication) or asymptomatic PAD would also have involvement of another arterial bed.3–5 Polyvascular disease imposes the highest risk for new or recurrent cardiovascular events around the world.6–8
PAD prevalence and its clinical implications vary widely according to the group at risk. It is now recognized that high-risk patients with symptomatic or asymptomatic atherosclerosis harbor a markedly different prognosis provided PAD is present or not. Furthermore, the polyvascular condition is more frequent in patients who present with PAD, than in those with CAD or CVD presentations.3–5 PAD can, therefore, be considered a marker of disseminated atherosclerosis. These facts represent the main foundation of the INDAGA studies, a series of three multicenter registries designed to assess PAD in high-risk stable outpatients attending Internal Medicine, Cardiology, and Neurology clinics in Mexico. In this report, we sought to describe the prevalence of PAD, risk factors, and six-month outcomes in high-risk stable outpatients with a recent history of acute coronary syndromes (ACS) or with major coronary risk factors.
Methods
Study settings
The INDAGA registries (from the Spanish
Before initiation, several meetings were held, in which all participating investigators received training on PAD epidemiology, risk factors, diagnosis and treatment, as well as the proper use of the Doppler technique and calculation of ABI. All operational study definitions were reviewed, and a study manual (printed and electronic) was provided to each investigator. A total of 40 cardiologists recruited consecutive patients in their private practice. Each patient had two visits with a minimum interval of six months of follow-up between visits. Cardiologists treated patients at their discretion according to current guidelines and were asked to measure ABI in all patients to identify concomitant PAD.
Inclusion criteria
Adult outpatients accepting participation by signing informed consent were considered for recruitment. Inclusion criteria were: (a) age >18 years and acute chest pain suggestive of angina lasting for >20 min or associated with changes of ST-segment elevation of 0.1 mV in two continuous leads on EKG, submitted or not to reperfusion therapy within 30 days of event onset. (b) Patients with non-ST-segment elevation ACS or changes in T wave within 30 days of percutaneous coronary intervention (PCI) or not. (c) Patients aged ≥55 years with a history of angina, positive exercise stress test, or previous MI. (d) Patients aged ≥55 years with a previous ischemic event and type 2 diabetes with at least one atherothrombotic risk factor, or age <55 years with two risk factors seeking cardiologist care.
Major risk factors investigated were: diabetes mellitus (fasting blood glucose ≥126/mg/dL, postprandial blood glucose ≥200 mg/dL or the need of insulin or oral glucose lowering drugs), hypertension (≥140/90 mmHg), hypercholesterolemia (total cholesterol ≥200 mg/dl), smoking habit (≥1 cigarettes per day), obesity [body mass index (BMI) ≥27 and ≥30], chronic kidney disease (CKD, estimated or measured glomerular filtration rate <60 mL/min/1.732), personal history of acute atherothrombotic events (CAD, CVD or PAD), and family history of atherothrombotic disease.
PAD was determined in the study cohort by calculation of ABI (systolic blood pressure in the ankle divided by a systolic blood pressure of the brachial artery) using a hand-held Doppler device with a 5–8 mHz probe. Systolic blood pressure measurements were obtained from each brachial, dorsalis pedis, and posterior tibial arteries. The upper limb systolic blood pressures (brachial arteries) were averaged to obtain the ABI denominator, but when the brachial arteries differed by ≥10 mmHg, the highest brachial artery pressure was used as the denominator. The ABI numerator was the highest pressure of either dorsalis pedis or posterior tibial from each lower extremity. The lowest ABI from both sides was used to classify the patient into an ABI category.7–11 ABI <0.9 was considered the criteria for the diagnosis of PAD.
Study endpoints
The INDAGA Cardiologists study had several goals both at baseline and at 6 months of follow-up. At baseline, the study aimed to determine the prevalence of PAD in patients with ACS and in patients with risk factors for atherothrombotic disease. Aims at six-month follow-up were to assess the occurrence of new acute atherothrombotic events (ACS, ischemic stroke and peripheral artery revascularizations or limb amputations), the rate of interventional revascularization procedures, as well as all-cause and vascular mortality.
Statistical analysis
Demographic information is presented as relative frequencies, or medians and interquartile range (IQR) or minimum and maximum, as appropriate. Pearson chi-squared statistics were used to compare frequencies of nominal variables. When less than five observations fell in a crosstabs cell, Fisher’s exact test was applied for p-value correction. Student t-test was used to compare continuous variables following a normal distribution between two groups. All p values were two-sided and regarded as significant if p < 0.05. SPSS v20.0 was used in all calculations in this report.
Results
Baseline characteristics
We included a total of 830 participants (57.8% men; median age: 64.8 years, range: 22–96 years). Among them, 707 patients reached the last follow-up visit at six months (61 abandoned the study shortly after recruitment, 51 patients had missing visits and 11 patients died before the last follow-up visit). Baseline characteristics were not different according to the sex of the participants. Abnormal low ABI was associated with age, diabetes, angina pectoris, current smoking, and CKD, but inversely associated with BMI >27 (Table 1). Moreover, the frequency of ABI <0.9 was different according to the inclusion criteria (Table 2).
Baseline demographic characteristics and risk factors of the INDAGA Cardiologists cohort (n = 830).
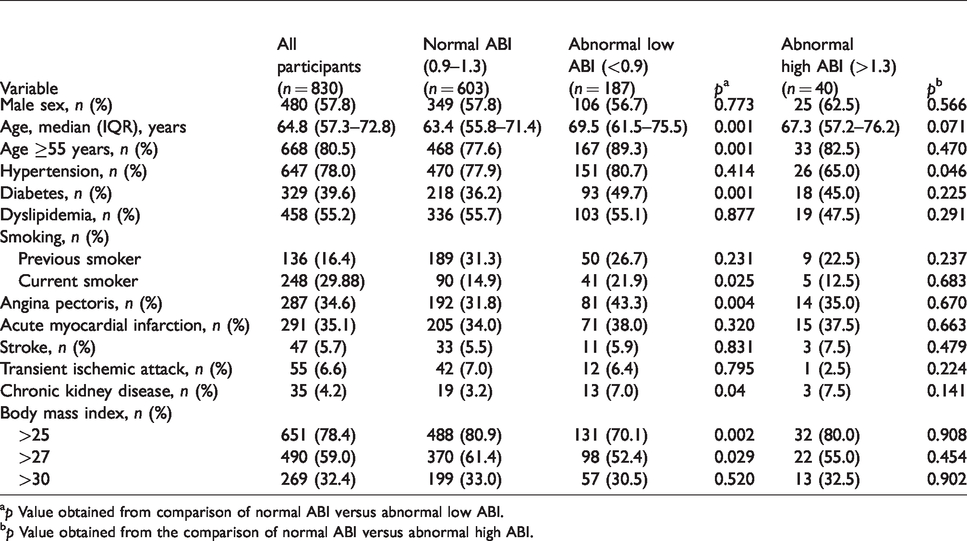
ap Value obtained from comparison of normal ABI versus abnormal low ABI.
bp Value obtained from the comparison of normal ABI versus abnormal high ABI.
Differences of an abnormal ankle-brachial index (ABI) according to sex and main characteristics of the inclusion criteria.
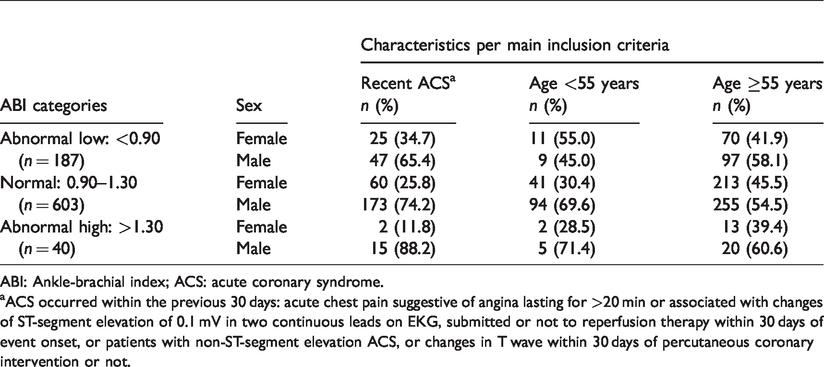
ABI: Ankle-brachial index; ACS: acute coronary syndrome.
aACS occurred within the previous 30 days: acute chest pain suggestive of angina lasting for >20 min or associated with changes of ST-segment elevation of 0.1 mV in two continuous leads on EKG, submitted or not to reperfusion therapy within 30 days of event onset, or patients with non-ST-segment elevation ACS, or changes in T wave within 30 days of percutaneous coronary intervention or not.
Association of the ankle-brachial index (ABI) and six-month case fatality rate in bivariable analyses (n = 707).
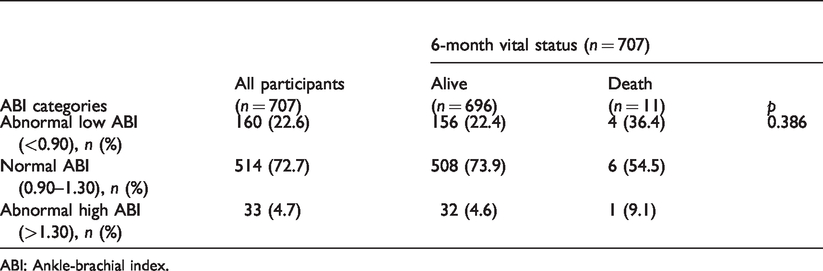
ABI: Ankle-brachial index.
PAD prevalence and risk factors
At baseline, ABI <0.9 was found in 22.5% of patients and ABI <0.8 in 10.6%. Abnormal high ABI (non-compressible arteries) was found in 4.8% with a cutoff of >1.3 and in 3.6% with a cutoff of >1.4. The frequency of an abnormal low ABI was progressively higher in advanced age categories (Figure 1).
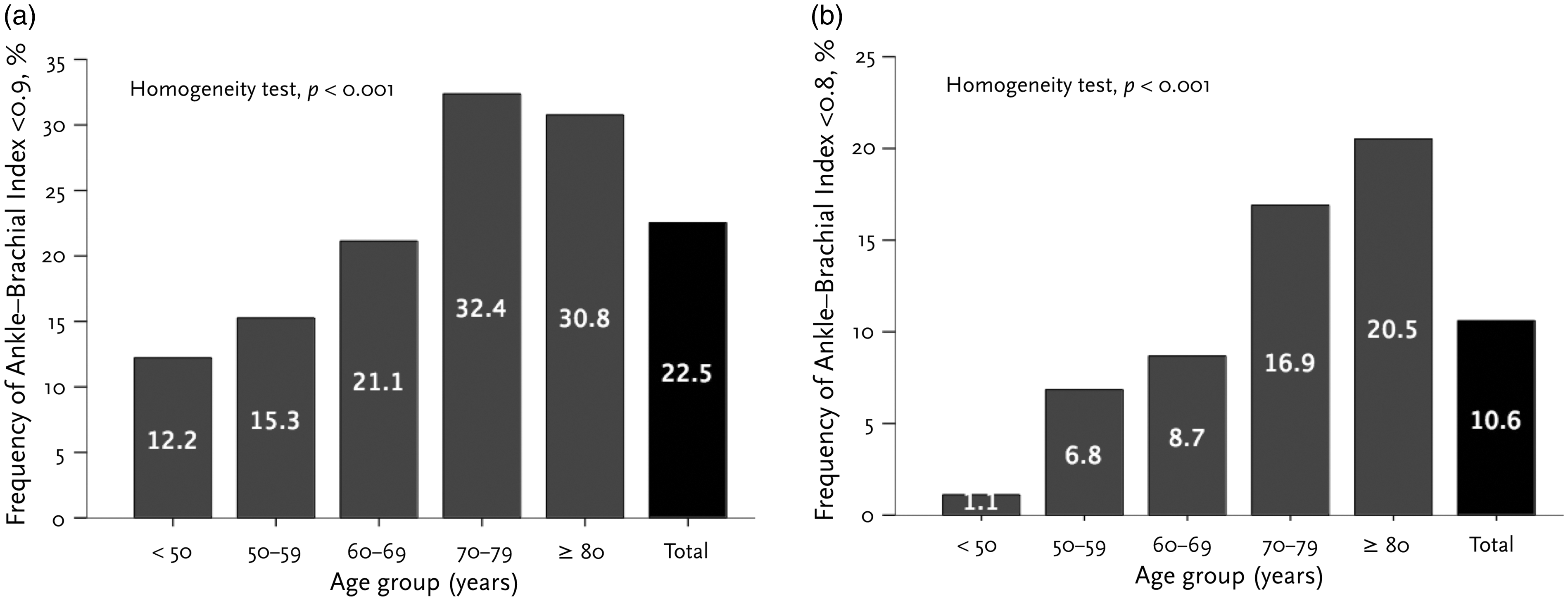
Distribution of and abnormal low ankle-brachial index according to age, for an ABI <0.9 (a) and <0.8 (b).
Outcomes
The six-month case fatality rate among the 707 participants who remained at the end of the study was 1.6% (Figure 2). Baseline ABI <0.9 was not significantly associated with the risk of death (six-month case fatality rate 2.5% vs. 1.3%, for ABI <0.9 vs. ≥0.9, respectively; p = 0.28) (Table 3). However, baseline ABI <0.8 was significantly associated with a higher six-month case-fatality rate (5.4% vs. 1.1%, for ABI <0.8 vs. ≥0.8, respectively; p = 0.02). In a Cox proportional-hazards model adjusted for demographic and known atherothrombotic risk factors, baseline characteristics associated with six-month death were age ≥65 years, ABI <0.8 and recent ACS (Harrell’s c-statistic of the model: 0.695, 95% CI: 0.511–0.879; p = 0.026) (Table 4). Actuarial analyses with the Kaplan–Meier method showed that ABI <0.8 is significantly associated with a shorter survival at a six-month follow-up (Figure 3). Vascular outcomes (acute coronary syndrome, ischemic stroke, lower-limb revascularization) occurred in 30 (3.6%) patients at a six-month follow-up. Vascular outcomes or death occurred in 31 (3.7%) participants. Angor pectoris was observed during follow-up in 18 (2.5%) patients, myocardial infarction in six (0.8%), transient ischemic attack in four (0.6%), ischemic stroke in one (0.1%), acute mesenteric ischemia in one (0.1%) and peripheral artery occlusion leading to limb amputation in one participant (0.1%).

Six-month case fatality rate according to ankle-brachial index cutoffs.
Multivariable analysis on factors associated with the six-month case-fatality rate: a Cox proportional-hazards model. a
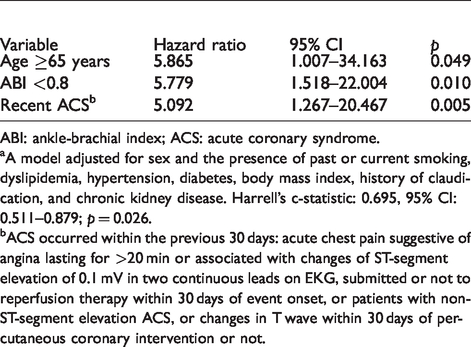
ABI: ankle-brachial index; ACS: acute coronary syndrome.
aA model adjusted for sex and the presence of past or current smoking, dyslipidemia, hypertension, diabetes, body mass index, history of claudication, and chronic kidney disease. Harrell’s c-statistic: 0.695, 95% CI: 0.511–0.879; p = 0.026.
bACS occurred within the previous 30 days: acute chest pain suggestive of angina lasting for >20 min or associated with changes of ST-segment elevation of 0.1 mV in two continuous leads on EKG, submitted or not to reperfusion therapy within 30 days of event onset, or patients with non-ST-segment elevation ACS, or changes in T wave within 30 days of percutaneous coronary intervention or not.
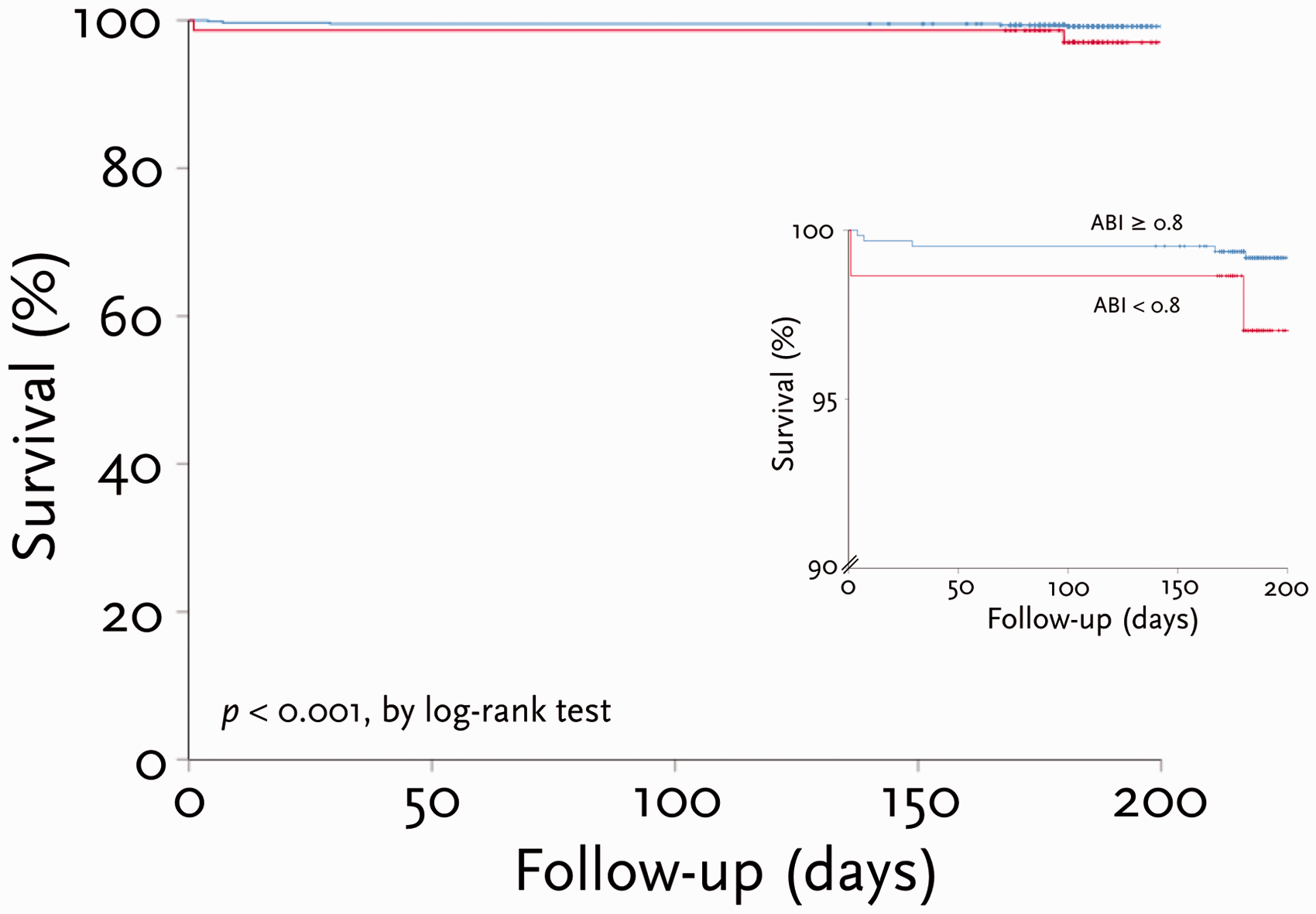
Kaplan–Meier actuarial analysis on the six-month survival as a function of an abnormal ankle-brachial index (ABI) <0.8 or ≥8.
Discussion
Our study suggests that subclinical PAD is more prevalent in patients with high coronary risk than with patients with symptomatic atherothrombosis of the lower limbs. Moreover, the present report shows that abnormal low ABI is associated with a higher probability of death, as compared with high-risk participants with normal ABI, even in the very short term. These data encourage routine clinical investigation for other forms of atherothrombotic disease in different vascular beds in patients with recent ACS. This approach may lead to a better stratification of the atherothrombotic risk by identifying the patient with polyvascular atherosclerotic disease.12–14 The finding that most six-month deaths were associated with an acute atherothrombotic event (i.e. coronary, cerebrovascular, or peripheral) reinforces the notion that a complete assessment of atherothrombosis risk is mandatory following an acute occlusive arterial event. These findings are in line with previous observations on the importance of risk assessment.14–19
PAD is very often under-recognized in clinics despite its high prevalence.1,19 In part this underdiagnosis may be due to a relatively asymptomatic course in the first part of the disease history, or to the fact that PAD may cause mild or nonspecific clinical manifestations. However, insufficient diagnosis of PAD in patients at high atherothrombotic risk or in individuals with recent acute ischemic events could be due to the lack of recognition that atherosclerosis is a widespread systemic inflammatory disease. An ischemic recurrence is more prevalent within the same arterial bed than in arteries outside the primary bed, but the presence of more than one arterial territory affected significantly increases the risk of death.20–22
In the present study, as well as in the previous INDAGA Internists study, 6 a very high proportion of patients with ABI <0.9 were reported as asymptomatic or with minimal discomfort attributable to PAD. Therefore, the determination of ABI may help to identify patients with a high vascular risk profile who may be a candidate for maximal medical treatment and surgical revascularization. Our results showed that the factors associated with abnormal ABI were age, diabetes mellitus, smoking, and history of cardiovascular or cerebrovascular events. These observations need confirmation in future studies focused on patients with a history of cerebrovascular disease. Another important finding of this study is the inverse relationship between PAD and BMI, the so-called obesity paradox.23–25 This apparent reduction in the risk of death in patients with high BMI may be due to an epiphenomenon between a reduced lean mass and chronic atherosclerotic disease, rather than the true protection of an excessive adipose tissue. 26
The present results are relevant for the clinical practice to emphasize that high-risk patients should be screened for PAD, even in those individuals without claudication symptoms. PAD screening helps to identify patients who may benefit from surgical revascularization of the lower limbs or best medical management with statins, angiotensin converting enzyme inhibitors and antithrombotics, as indicated by atherothrombosis severity and comorbid conditions. Moreover, as demonstrated in the COMPASS trial, this population with PAD would experience the highest benefit with low-dose anticoagulation with rivaroxaban plus aspirin, and therefore, should be assessed for the candidacy of such therapy according to the COMPASS selection criteria.27–29 To maximize benefit and to avoid negative interactions, these therapeutic strategies should be considered in the context of the new antithrombotic regimes for patients with recent ACS, such as dual antiplatelet therapy and triple antithrombotic therapy that includes a non-vitamin K antagonist oral anticoagulant (NOAC) plus dual antiplatelet therapy. 30
The most important limitation of this study was the relatively small sample size that may impair the detection of small but clinically meaningful differences. This registry also had a short follow-up period to observe a high number of atherothrombotic outcomes. Such a low number of events would require a larger sample size; therefore, this study might be underpowered to detect relatively infrequent vascular outcomes (such as peripheral artery revascularizations, limb amputations, and hospitalizations due to ischemia). Other non-traditional risk factors such as metabolic, anthropometric, and genetic variables would certainly add further risk prediction to this analysis.
Conclusions
In conclusion, asymptomatic PAD is more prevalent than claudication in high-risk stable outpatients with ACS within the past 30 days, or at high cardiovascular risk. A very low ABI is associated with shorter survival and is predictive of relevant cardiovascular outcomes, even in the short term.
INDAGA Cardiologists investigators
Chávez Fernández JA (Mexico City), Alcocer Gamba A (Querétaro), Serna Zetina E (Torreón), Bautista López GR (Guanajuato), Virgen Carillo LR (Guadalajara), De los Ríos Ibarra MO (Culiacán), Cerda Rojas J (Aguascalientes), Montes Cruz ES (Mexico City), Ficker García G (Torreón), Ontiveros Godínez T (Guadalajara), Espinosa Vázquez RA (Mexico City), Cardona Muñoz EG (Guadalajara), Maldonado Villalón JA (Morelia), De la Cruz Estrella AE (Guadalajara), Garduño Martínez VG (Mexico City), Matadamas Hernández N (Acapulco), Vázquez Nájera J (Mexico City), Deloya Maldonado A (Acapulco), Calleja Chávez JM (Mexico City), Corona Tapia A (Mexico City), Solórzano Zepeda FJ (León), Álvarez López H (Guanajuato), Castañeda Mendoza R (Jalisco), Ortega Gutiérrez AA (Mérida), Ruíz Nieves RA (Puerto Vallarta), Medécigo Micete JM (Mexico City) , Cordero Contréras G (Saltillo), Álvarez Gil J (Guadalajara), Casares Ramírez M (Durango), Sánchez Landa C (Zacatecas), Velasco Sánchez R (Zapopan), Murillo Blanco PR (Mexico City), Ramírez Ríos SA (Tamaulipas), Martínez Bermudez P (Monterrey), Ramírez López JJ (Tampico), Guerra López A (Tijuana), López Padilla LA (Cuernavaca), Moreno Villa J (Guadalajara), De la Cruz Rivera A (Mexico City) , Jiménez Castellanos S (Culiacán), Quiroga Aguirre V (Tepic), Mendoza Ortega O (Tijuana), and Leiva Pons JL (San Luis Potosí).
Supplemental Material
sj-pdf-1-vas-10.1177_1708538120938921 - Supplemental material for Peripheral artery disease in outpatients with a recent history of acute coronary syndrome or at high atherothrombotic risk
Supplemental material, sj-pdf-1-vas-10.1177_1708538120938921 for Peripheral artery disease in outpatients with a recent history of acute coronary syndrome or at high atherothrombotic risk by Carlos Cantú-Brito, Erwin Chiquete, Javier F Antezana-Castro, Liz Toapanta-Yanchapaxi, Ana Ochoa-Guzmán, José Luis Ruiz-Sandoval and INDAGA Cardiologists Investigators in Vascular
Footnotes
Acknowledgements
The INDAGA registry enforces a no ghostwriting policy. Sanofi Mexico did not participate either directly or indirectly in the selection of patients, data capture, data analysis, manuscript drafting, or the decision to submit for publication. This manuscript was written and edited by the authors, who take full responsibility for its content.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C-B has received research grants from Sanofi, Ferrer Grupo and Bayer, speaker honoraria from Sanofi, Bayer, Boehringer-Ingelheim, Silanes, and Ferrer Grupo and has served in advisory boards organized by Sanofi and Bayer. EC has received research grants from Sanofi and Ferrer Grupo, speaker honoraria from Novartis, Boehringer-Ingelheim, Asofarma, Silanes, and Ferrer Grupo and has served in advisory boards organized by Genzyme. JFA-C has received research grants from Sanofi. JLR-S has received research grants from Sanofi and speaker honoraria from Sanofi, Boehringer-Ingelheim, and Ferrer Grupo.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Sanofi Mexico. The INDAGA registry enforces a no ghostwriting policy. Sanofi Mexico did not participate directly or indirectly in the selection of patients, data capture, data analysis, manuscript drafting, or the decision to submit for publication. This manuscript was written and edited by the authors, who take full responsibility for its content.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.