
Abstract
Objectives
Aortic dissection involving the ascending aorta and aortic arch is a serious condition. Treatment using traditional surgical methods has certain disadvantages. This study investigated the effectiveness of thoracic endovascular repair of aortic dissection using an external prefenestrated stent.
Methods
We present a series of aortic dissection cases involving the ascending aorta and aortic arch treated with an external prefenestrated stent.
Results
Postoperative follow-up of the patients showed that all stents were released at the proper position and that branch vessels were not occluded, and there were no instances of type I endoleak. One patient died suddenly one week after surgery; another experienced retrograde type A aortic dissection in the second week; and type I endoleak occurred in one patient in the first week, although this resolved within six months. No serious complications such as cerebrovascular events, acute spinal cord ischemia, and paraplegia occurred during the perioperative period. All patients had false lumen thrombosis in the ascending aorta and aortic arch.
Conclusion
Prefenestrated stent grafting is a feasible treatment option for repairing an entry tear in the ascending aorta.
Introduction
Aortic dissection and/or penetrating ulcers involving the ascending aorta and aortic arch are serious conditions that undermine overall health. 1 In Stanford type A aortic dissection, the entry tear is located in the ascending aorta and aortic arch, or else originates in the descending aorta with retrograde dissection to the ascending aorta and aortic arch. 2 In contrast, Stanford type B aortic dissection occurs at the distal end of the left subclavian artery (LSA). 3 The standard treatment for type A aortic dissection is open surgery, despite high mortality and complication rates.4,5 The deep hypothermic circulatory arrest required during the procedure can cause severe trauma and may be fatal, especially in patients of an advanced age; who have previously undergone heart or aortic surgery; or have neurologic dysfunction, hypertension, or myocardial ischemia. 6 In cases requiring closure of the distal end of the ascending aorta (zone 0), branched vessels are transplanted to the ascending aorta using the “branch first” technique of aortic arch replacement, with thoracic endovascular aortic repair (TEVAR) performed simultaneously or in stages.7,8 Aortic clamping and suturing of the bypass increases the risk of retrograde aortic dissection. 9 Additionally, ascending aorta replacement is required for lesions involving the ascending aorta. 1
In previous studies, we performed prefenestrated stent grafting and stent placement at branched vessel openings to promote revascularization of the left common carotid artery (LCA) and LSA, which achieved good clinical results in patients requiring coverage of the initiating part of the LSA (zone 2). In this study, we investigated the intermediate-term effects of TEVAR with prefenestration stent grafting on aortic arch dissection (penetrating ulcer) requiring coverage of zones 0 and 1.
Methods
Patients
Written, informed consent was obtained from each patient and ethics approval for this study was obtained from our institution. The study cohort included nine patients (seven males and two females, aged 32–74 years) who underwent TEVAR with prefenestrated stent grafting for aortic dissection (penetrating ulcer) involving the ascending aorta and aortic arch between April 2016 and June 2017 at the Department of Cardiovascular Surgery, General Hospital of Ningxia Medical University. Aortic dissection of nine patients was due to poor hypertension control combined with a history of hypertension, and family history of hypertension was excluded. All patients did not have the characteristic manifestations of Marfan syndrome. The aortic tissues from patients used for pathological examination were not obtained because of the endovascular repair surgery. There were eight cases of hypertension, one case of right radial artery occlusion, and one case of left renal artery infarction. Patients’ clinical information was shown in Table 1. Endovascular repair was considered for a 65-year-old female patient with a history of TEVAR surgery for Stanford type B aortic dissection located at the distal end of the ascending aorta (zone 0) who refused surgery. The entry tear was located in zone 2 in seven cases and in the proximal descending aortic (zone 3) in one case. Preoperative computed tomography angiography (CTA) (Philips Extended Brilliance Workspace 4.5, Brilliance iCT; Philips, Amsterdam, The Netherlands) showed that none of the patients was eligible for standard TEVAR surgery. The main manifestations in all patients were refractory hypertension, cerebrovascular disease (transient ischemic attack or stroke), persistent or recurrent chest and/or back pain, pleural effusion and compression symptoms, and progressive aortic dilation.
Clinical information of the patients.
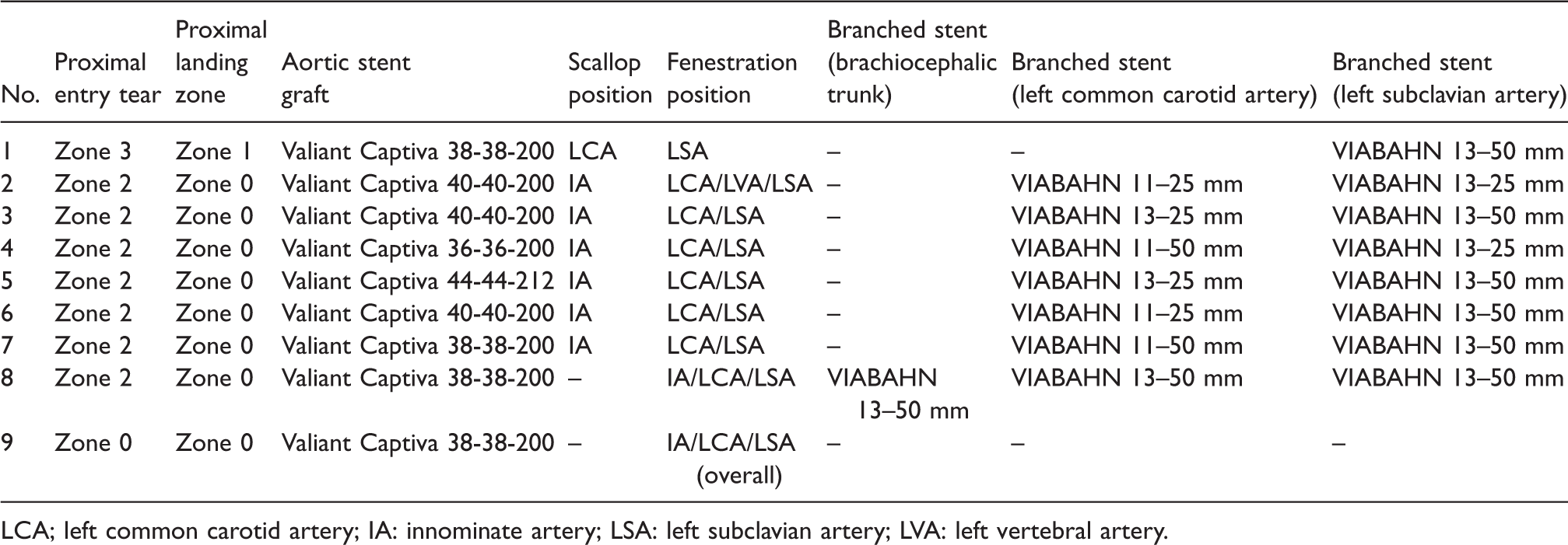
LCA; left common carotid artery; IA: innominate artery; LSA: left subclavian artery; LVA: left vertebral artery.
Stent modification
Multiangle measurements obtained from the coronal and sagittal planes in the preoperative CT angiography were used for three-dimensional (3D) reconstruction and visualization of aorta anatomy and origin of branched vessel openings in the aortic arch, which allowed accurate localization of fenestration and slotting positions. Additionally, a solid model of the aortic arch was 3D-printed as necessary for auxiliary branch selection.
Aortic stents Captivia (5–10% oversizing) (Medtronic, Minneapolis, MN, USA) were maneuvered to the proper positions and fenestration was performed using the hot melt technique with low-energy on the tectorial membrane of stents corresponding to the openings of the innominate artery (IA), LCA, and LSA. And the effective diameter of the openings was less than the planned diameter of Viabahn stent to prevent postoperative type III endoleak. The stents were loaded back into the conveyor system after repositioning the stent markers (Figure 1). One of the markers at the proximal end of the original thoracic aortic stent graft was removed to the front or rear end edge of the opening, and this marker can still be clearly displayed under fluoroscopy.

Extracorporeal prefenestrated stent graft used in endovascular repair of ascending aorta–aortic arch lesions.
Surgical procedure
TEVAR was performed on all patients under local anesthesia. Then the right or left common femoral artery and left brachial artery were punctured with the Seldinger technique. The intraoperative localization of the orifice of LSA relies on the catheter from the left brachial artery to the ascending aorta, which went through the LSA, as a marker. The right brachial artery was punctured at the same time if the IA was needed for branched stent grafting. A capture guide wire was first used to establish a path from the brachial artery to the femoral artery, and the Gore Viabahn stent (0–5% oversizing), a self-expanding intravascular stent graft system, was then introduced through the femoral artery to the opening of the branch artery.
After the intraoperative aortic angiography, under the preset fluoro angle measured through preoperative CTA scan, the distally restricted aortic stent was introduced into the descending aorta at a suitable position along the Lunderguist extra-stiff guide wire; we then introduced the fenestrated stent graft system to the ascending aorta. When in position, we slowly released the first two sections of the stent and observed the alignment of the fenestrations and branch vessels by angiography, followed by microadjustment. Pumping small doses of sodium nitroprusside was performed in advance 15–30 min before releasing the stent to maintain the invasive arterial systolic pressure between 100 and 120 mmHg. The rest of the stent graft was rapidly deployed and the proximal release device was then opened to fully deploy stent graft (Figure 2). Standard TEVAR requires a proximal landing zone of at least 1.5 cm. In patients with an entry tear of aortic dissection in zone 2, according to the principle of 1.5 cm proximal landing zone, the landing position is mostly located in zone 1. The Medtronic Valiant Captiva thoracic aortic stent graft used in the procedure had a proximal bare segment with 12 mm in length. Landing in zone 1 was prone to mechanical damage of the aorta, such as retrograde tearing type A dissection, because of the bare segment of the stent located in the ascending aorta and the aortic arch transition. The proximal landing zone was in zone 0 for patients with an entry tear in zone 2. The steps were as follows:
The Lunderguist extra-stiff guide wire (Cook Medical) and measuring catheter were introduced into the ascending aorta through the left or right common femoral artery, and the fenestrated stent graft was deployed in zone 2. The Terumo GLIDEWIRE (0.035”, 260CM) guide wire and MPA (multipurpose angiography)catheter were introduced into the LCA and LSA through the common femoral artery and exchanged with the Amplatz super stiff guide wire (Boston Scientific); the branched stent was then deployed through the LCA and LSA opening along the Amplatz guide wire. The Terumo GLIDEWIRE and MPA catheter were introduced to the arch through the common femoral artery, and the branched stent was deployed through the IA along the Amplatz guide wire.
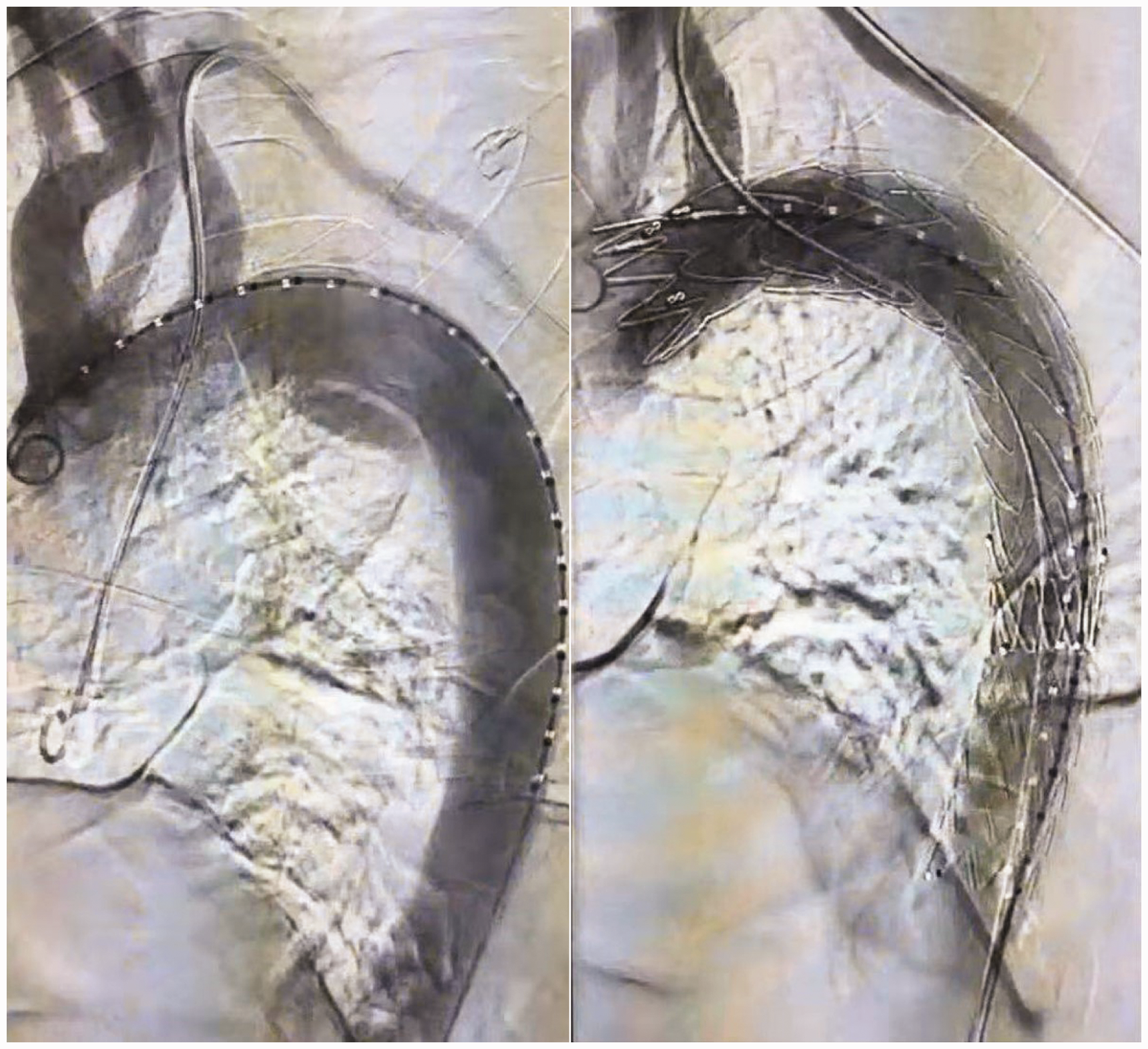
Intraoperative aortic angiography showing the aortic arch before (left) and after (right) fenestrated stent graft deployment.
The decision of whether to introduce the balloon catheter was made based on the shape of the deployed stent. The results were observed immediately through the intraoperative angiography of the ascending aorta. Successful repair was marked by intact proximal release of the aortic stent, with no type I endoleak and all branches were patent.
Postoperative treatment and follow-up
The patients received a subcutaneous injection of low-molecular-weight heparin as an anticoagulant after the operation, and gradually transitioned to oral enteric-coated aspirin tablets (100 mg/day) as antiplatelet treatment. A mean arterial pressure >90 mmHg was maintained post-surgery to ensure a blood supply to the spinal cord. 10 Aortic CTA was performed 1, 6, and 12 months after surgery to evaluate false lumen thrombosis and aortic remodeling.
Results
The total operation time was 130–180 min, with an average of 152.22 (±17.81) min. In the early stage of the operation, it took more time to modify and reload the stent to the delivery system. As the learning curve is mastered, the operation time is further shortened. The dose of contrast agent ranged from 100 to 160 mL, with an average of 133.33 (±19.36) mL (data not shown). All stents were deployed at the proper position and those in branch vessels were unobstructed. There was no evidence of a type I endoleak after surgery by CTA (Figure 3). There was one case of sudden death in the first week after surgery involving a 55-year-old male with an entry tear located in zone 2. We made a scallop in the IA, with LCA and LSA fenestration and branched stent grafting. The proximal landing zone was located in zone 1. Postoperative angiography showed complete exclusion of the proximal entry tear and no occlusion of the branched stent.
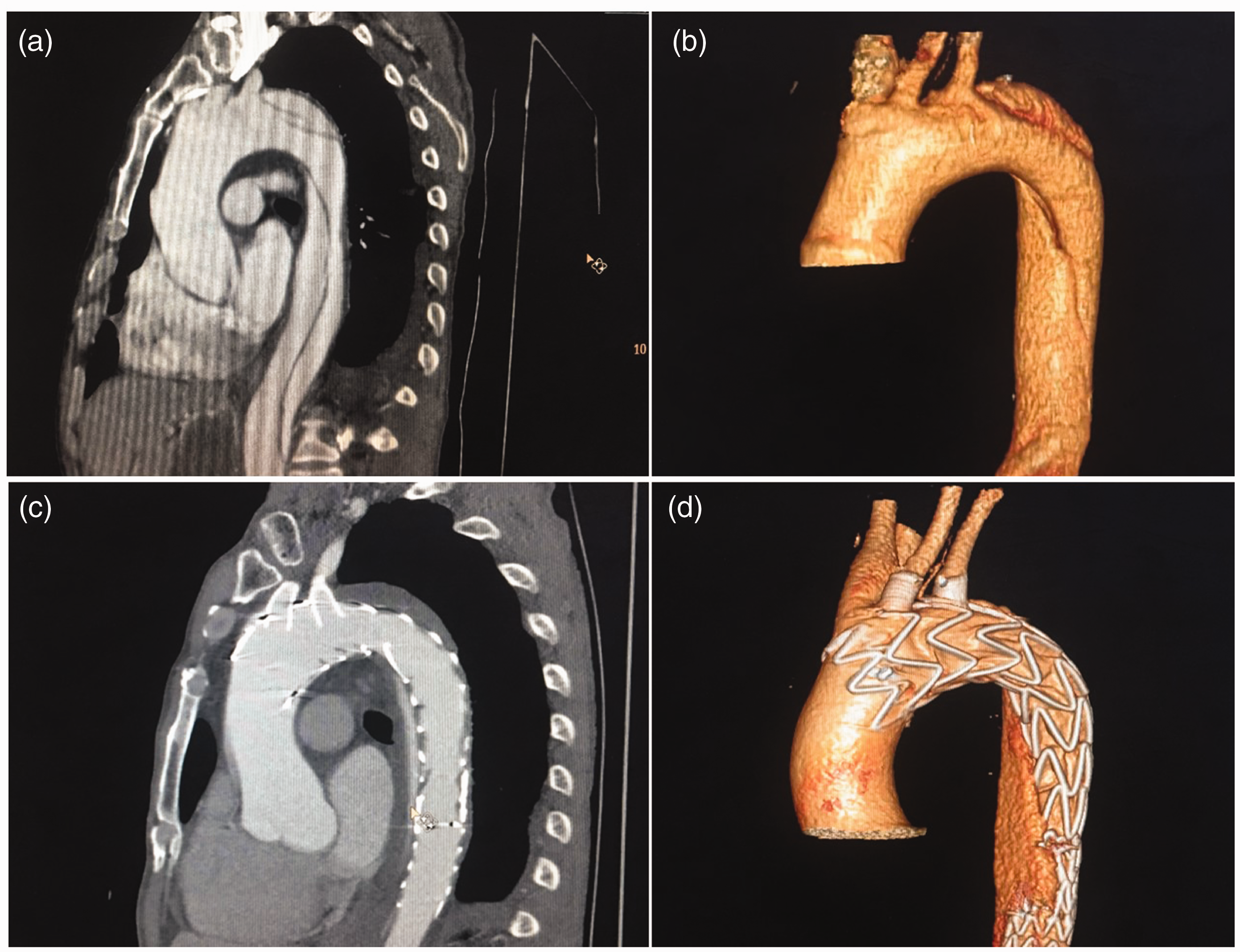
Demonstration of fenestrated endovascular repair before and after the procedure. (a and b) Preoperative CTA showing aortic dissection with entry tear located at the opening of the LSA. (c and d) Postoperative CTA showing that there was no occlusion of the stents in the aorta, LCA, and LSA, with thrombosis in the false lumen.
There was one case of retrograde aortic dissection in the second week after surgery involving a 46-year-old male with an entry tear located in zone 3 and slotting in the LCA, who underwent LSA fenestrated and branched stent grafting. Retrograde type A dissection (RTAD) was observed two weeks after surgery. The entry tear was located on the side of greater curve at the proximal end of the stent and did not involve the coronary artery. The patient was then treated by embolization of the ascending aortic false lumen with Interlock-35 coils (Boston Scientific), resulting in a decrease in contrast agent density in the postoperative CT angiography. Postoperative follow-up showed that no ascending aortic dissection had developed. A type I endoleak was observed one week after surgery in one case, but diminished within six months without any treatment. One patient underwent surgical treatment for biliary pancreatitis 12 months after the endovascular surgery. One patient developed renal insufficiency 36 months after surgery and received no further treatment. As of July 2020, the follow-up period ranged from 48 to 51 months, with an average of 46.5 (±4.47) months. Except for patients with sudden death, no patients died during the follow-up period.
There were no serious complications such as cerebrovascular events, acute spinal cord ischemia, and paraplegia during the perioperative period. All patients were followed up for 2–15 months; during this time, fenestration positions were aligned with branched vessel openings, there was no occlusion of branched stents, and no deaths or complications. All patients had false lumen thrombosis in the ascending aorta and aortic arch (Table 2).
Post-operative follow-up results.

Discussion
Approximately two-thirds of aortic dissections (penetrating ulcer) involve the ascending aorta and aortic arch. The condition is more common in men, with a mean age at onset of 63 years old. 11 The main risk factors include hypertension, aortic dilation, congenital cardiovascular defects, and hereditary connective tissue diseases. Open surgery is currently the gold standard treatment for aortic arch diseases, with the aim of removing the primary intimal tear, repairing the ascending aorta, and restoring the functionality of the aortic valve. 4 However, open surgery requires deep hypothermia to stop blood circulation, which leads to severe surgical trauma and has a high risk of mortality. 12 Perioperative endovascular therapy can potentially reduce mortality, and about 32–50% of aortic dissections are amenable to endovascular repair.10,13
One challenge in the endovascular repair of ascending aorta and aortic arch dissection is that the proximal end of the stent is close to the aortic valve and coronary artery orifice, with the distal end potentially affecting blood flow in the branch vessels of the aortic arch. Accurate stent deployment, which is critical for the success if the procedure, is hindered by strong hemodynamic forces in the ascending aorta and iliac artery that distort the shape of the arch. 14 Multi-angle measurements of coronal and sagittal planes can facilitate accurate selection of the stent fenestration position; repositioning the stent marker ensures that it is aligned with the opening of the LSA, LCA, and IA. Rapid and continuous stent deployment fashion can also prevent stent distortion and displacement caused by rapid blood flow within the arch. 1 Selective adenosine-induced cardiac arrest or temporary pacemakers can prevent post-stent hopping caused by heart contraction during stent release.15,16 In this study, controlled hypotension was used to reduce cardiac output, but the ascending aorta still had large amplitude of motion and made a mild premature jump during the rapid release of the stent, although it did not affect the functioning of the aortic valve or blood flow in the coronary artery and branched vessels of the aortic arch. Blood pressure and cardiac output were reportedly decreased by ventricular tachycardia when the delivery system contacted the left ventricular wall, which was beneficial for rapid and accurate stent release. 17 In this study, the anterior vertebra of the tip set of the delivery system entered the left ventricle through the aortic valve but did not touch the left ventricular wall; therefore, ventricular tachycardia was not induced.
RTAD is a serious postoperative complication caused by angulation of the aortic arch, connective tissue disease, proximal landing position, ascending aorta diameter >4 cm, and increased stress on the aortic wall. There was one case of RTAD in this study in which the landing area was in zone 1; CTA revealed that the entry tear was located on the side of greater curve at the proximal end of the stent. Notably, in eight cases, proximal landing zone was in zone 0, and no RTAD occurred. Thus, landing in zone 1 may be the reason for the RTAD. Increasing the length of the proximal landing zone and extending it to the straight portion of the ascending aorta can potentially reduce morbidity associated with RTAD.9,18 On the other hand, applying the stent with a bare segment at the proximal end remains controversial as it may increase the risk of RTAD. 19
General anesthesia is recommended for standard TEVAR procedure. However, the stiff guide wire and stent in the distorted aortic arch may cause plaque rupture and stroke. Therefore, local anesthesia was used in our study, which allowed us to monitor the patient’s state of consciousness throughout the operation and detect any disturbance that caused by cerebral infarction due to plaque detachment. However, the disadvantages are also obvious. The patient’s intraoperative coordination will interfere with the procedure, and it is not conducive to respiratory control for aortic angiography.
The clinical staff participated in this study were cardiovascular surgeons, and there are about 30–40 aortic patients undergo open surgery in our center every year. The basis of our endovascular repair with two fenestrations is that we have already mastered the single-branch fenestration technique for the treatment of aortic lesions with hostile proximal landing zone. Since 2014, we have completed about 150 cases of extracorporeal pre-fenestration endovascular repair surgery, and the procedure has been formulated in a process. The corresponding fenestration equipment has been developed to facilitate the procedure. On this basis, we only tried to carry out two or three pre-fenestrations. It must be admitted that this type of procedure can only be an individualized therapy, and we believe that it cannot be carried out routinely at this unless new devices for delivery and deployment of the customized fenestrated stent graft were developed in the future. For patients with unsuitable anatomy, we prefer open surgery or hybrid technique.
The limitations of this study include a small sample size, short follow-up time, and lack of comparison between results achieved by open surgery, hybrid procedures, or chimney techniques. Unfortunately, we paid less attention to the radiation dose during the procedure. The imaging equipment that we use (PHILIPS DSA FD20 system) did not record the radiation dose during the operation, resulting in the lack of data in this part. In addition, cases of aortic dissection (penetrating ulcer) involving the proximal ascending aorta and aortic arch were not included in our study, although they are worth investigating in future work.
In conclusion, extracorporeal pre-fenestrated stent grafting is a feasible endovascular treatment option for an entry tear involves ascending aorta and aortic arch, although a longer follow-up period is needed to substantiate these results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Project of Science and Technology Development of Ningxia Hui Autonomous Region in 2018 (Grant No.: 2018BEG03029).