
Abstract
Objectives
Anatomic variations of the extracranial carotid artery are rare. Persistent primitive hypoglossal artery appears with a reported incidence between 0.03% and 0.2%. We report a case of recurrent transient ischemic attacks originating from proximal internal carotid artery stenosis associated with ipsilateral persistent primitive hypoglossal artery and give a review of the existing literature.
Methods
A 78-year-old patient with a medical history of two previous transient ischemic attacks consulted our emergency department with an acute left hemispheric stroke. Intravenous thrombolysis permitted complete resolution of symptoms. Concurrent Computed Tomography (CT) and Magnetic Resonance (MR) angiography revealed an unstable plaque causing 50% stenosis of the left internal carotid artery with a persistent primitive hypoglossal artery dominantly perfusing the posterior circulation, and bilateral hypoplastic vertebral arteries.
Results
Uneventful carotid artery stenting using a proximal protection device was performed, and the patient was discharged after 12 days. Six months follow-up was uneventful with a patent stent in the internal carotid artery.
Conclusions
Treatment of symptomatic carotid artery stenosis in the presence of persistent primitive hypoglossal artery is challenging. Management should be driven by patients’ co-morbidities, the anatomical localization of the lesions and local expertise. In the case of a high origin of the persistent primary hypoglossal artery, carotid artery stenting with the use of a proximal cerebral protection device is probably the preferred and simplest approach.
Keywords
Introduction
Anatomic variations of the extracranial carotid artery are very rare. Among them, a persistent primitive hypoglossal artery (PPHA) is the second most frequent fetal carotid–vertebrobasilar anastomosis present in 0.03%–0.2% of cerebral angiograms in adults. 1 It originates from the internal carotid artery (ICA) at the level of C1–C3 and enters into the intracranial space through the hypoglossal canal, joining the basilar artery at the base of the skull. 2
Usually, carotid–vertebrobasilar anastomoses are present in the early stage of embryonic development and regress by the 30th or 40th day of development with the formation of the posterior communicating arteries. Underdevelopment of the latter can lead to the persistence of theses anastomoses with a hypoplastic or aplastic ipsilateral vertebral artery. 2 In these circumstances, PPHA is often the only arterial supply to the posterior circulation. Consequently, arterial embolization from concomitant carotid disease, in the presence of a PPHA, can result in ischemic stroke in both the anterior and posterior circulation and the management of ischemic stroke in this unusual setting can be challenging.
We present a case of recurrent transient ischemic attacks (TIAs) in a patient with proximal ICA stenosis associated with an ipsilateral PPHA, treated by carotid artery stenting (CAS), while attempting to provide insight on the management based on a review of the rare relevant published cases.
Case report
A 78-year-old right-handed man with a medical history of hepatocarcinoma, hypertension, diabetes and chronic renal insufficiency was transferred to our emergency department 2 h after experiencing an acute left hemispheric stroke. Medical history contained two previous episodes of minor ischemic strokes over the past three years treated conservatively. At presentation, aphasia, right hemineglect, right homonymous hemianopsia and right-sided hemiparesis were documented. Initial National Institute of Health Stroke Scale (NIHSS) score was 6.
Emergency cerebral Computed Tomography Angiography (CTA) with perfusion mapping revealed a perfusion asymmetry with an increased mean transit time to the left temporal lobe, an unstable plaque causing a 50% stenosis of the left ICA, a PPHA and bilateral hypoplastic vertebral arteries. The PPHA originated 2 cm distal to the carotid bifurcation at the level of the C1–C2 vertebrae, entering the cranium through the hypoglossal canal and dominantly perfusing the posterior circulation (Figure 1).
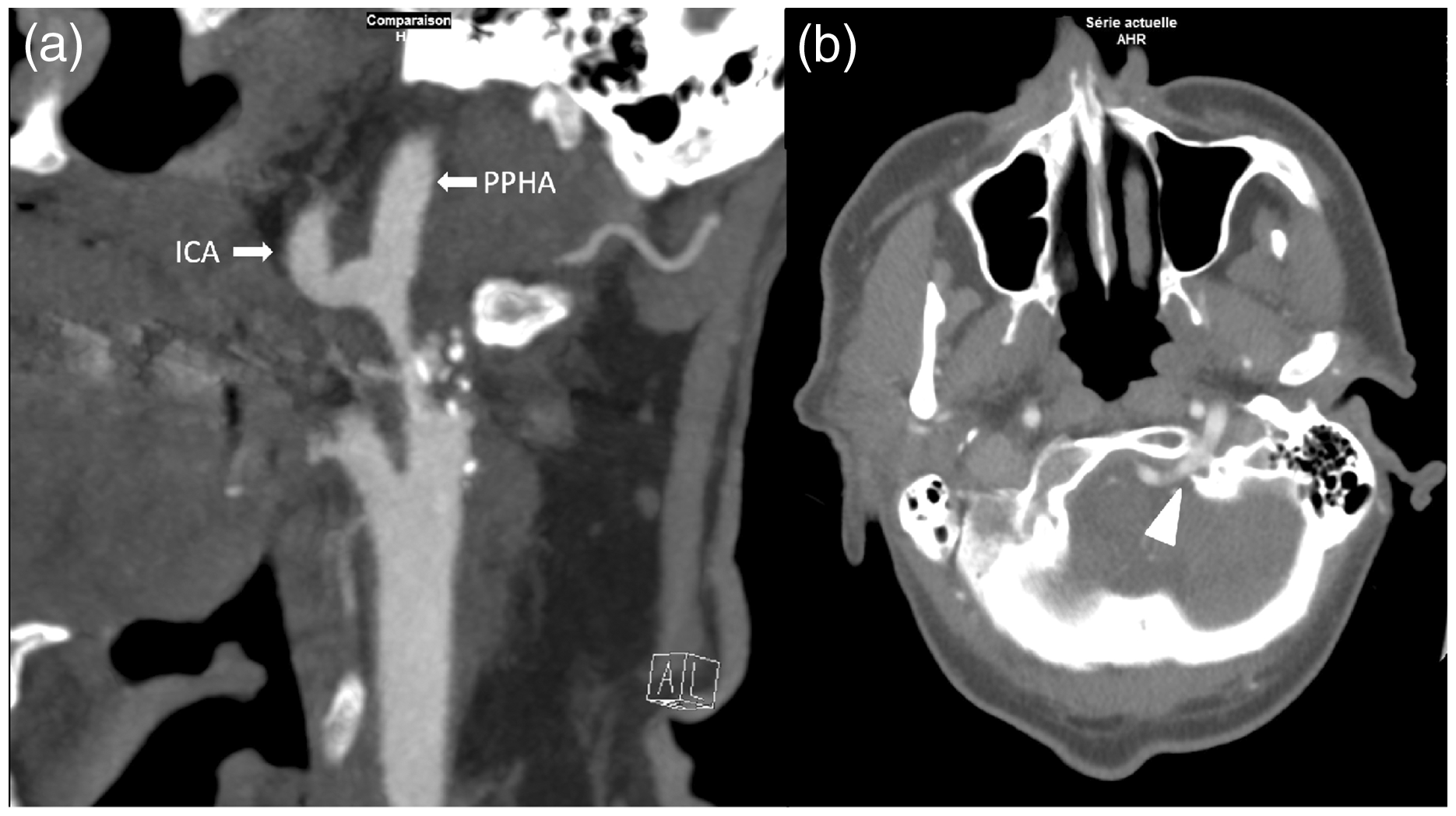
(a) CT angiography showing a 50% luminal stenosis of the left internal carotid artery extending from 2 cm above the carotid bifurcation up to the origin of the PPHA at the level of the C1-C2 vertebrae, (b) the PPHA enters the cranium through the hypoglossal canal (white triangle).
After rapid evaluation by the stroke team, intravenous thrombolysis with tissue plasminogen activator (tPA) was administrated within 20 min, with complete resolution of symptoms over the following hours. MR angiography revealed acute ischemic lesions in the territory of the left middle cerebral artery as well as chronic ischemic lesions in the left cerebellum, compatible with prior undiagnosed TIAs of the posterior circulation.
Following multidisciplinary discussion, the patient was transferred to a tertiary university center for CAS. The intervention was performed in the angiography suite under local anesthesia at nine days from the index event. After puncture of the right femoral artery, selective carotid angiography was performed using a 5 F Tempo JB3 catheter (Cordis, Miami Lakes, Florida, USA), confirming a 50% stenosis 2 cm distal to the carotid bifurcation, extending up to the PPHA–ICA bifurcation, so extending the stent distally was necessary for complete coverage. After proximal occlusion using a 9 Fr MoMa (Medtronic, Dublin, Ireland) device, the stenosis was crossed with a 0.0014 inches Asahi Sion guidewire (Asahi Intecc Co., Aichi, Japan) and a 7–10 × 40 mm Protégé tapered stent (ev3, Plymouth, MN, USA) was successfully placed (Figure 2). Jailing of the ICA was chosen because the PPHA had a more straight-forward, less tortuous direction, with the guidewire already in place.
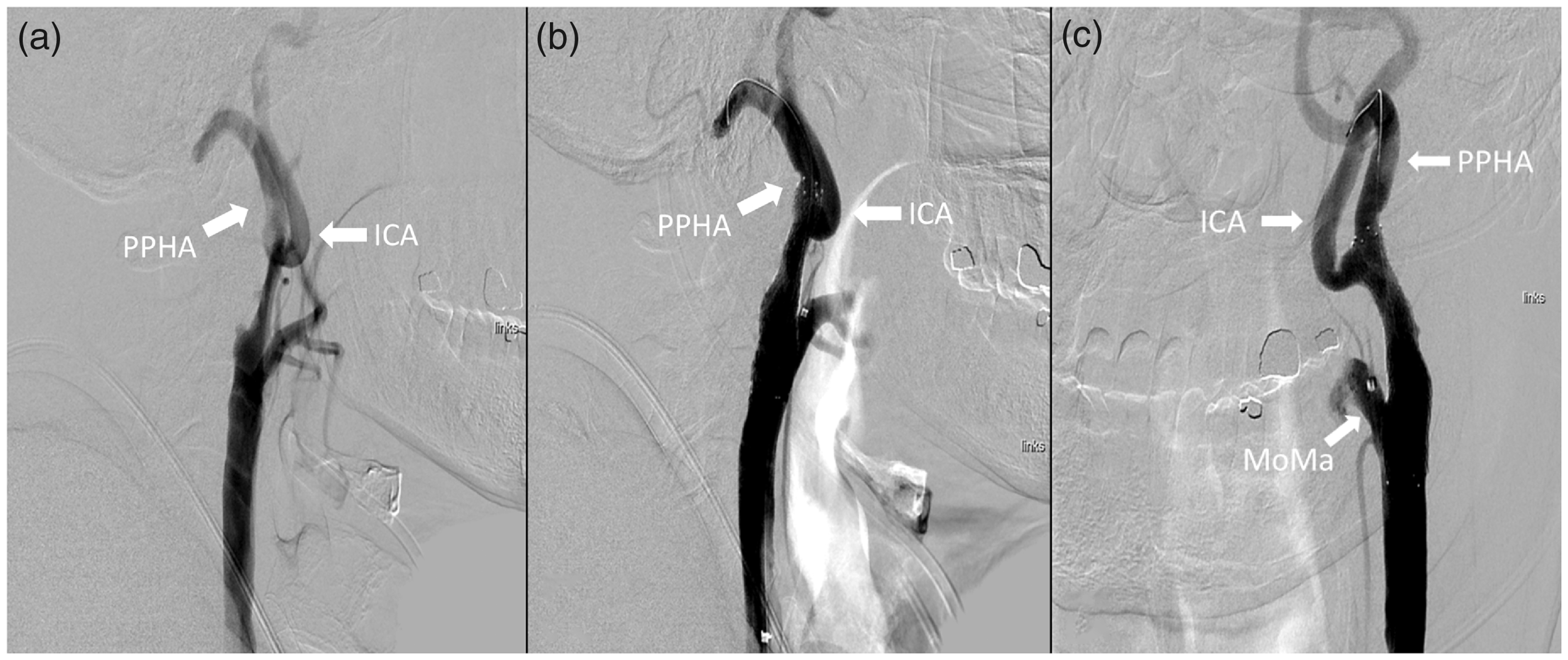
(a) Selective angiography of the left carotid artery showing an ulcered atheroma in the left ICA extending over 2 cm from the carotid bifurcation, up to the origin of the PPHA. (b) Stent deployment with the guidewire in the PPHA. (c) Final angiography in frontal view showing patency of both the ICA and the PPHA, with complete coverage of the lesion. Notice the balloon exclusion tip of the MoMa device placed in the ECA.
There were no peri-/post-interventional neurologic events. Carotid duplex was performed four months after stenting, which showed no stent restenosis and no flow disturbance due to ICA jailing. At six months follow-up, he remained asymptomatic with a patent stent in the ICA on CTA (Figure 3).
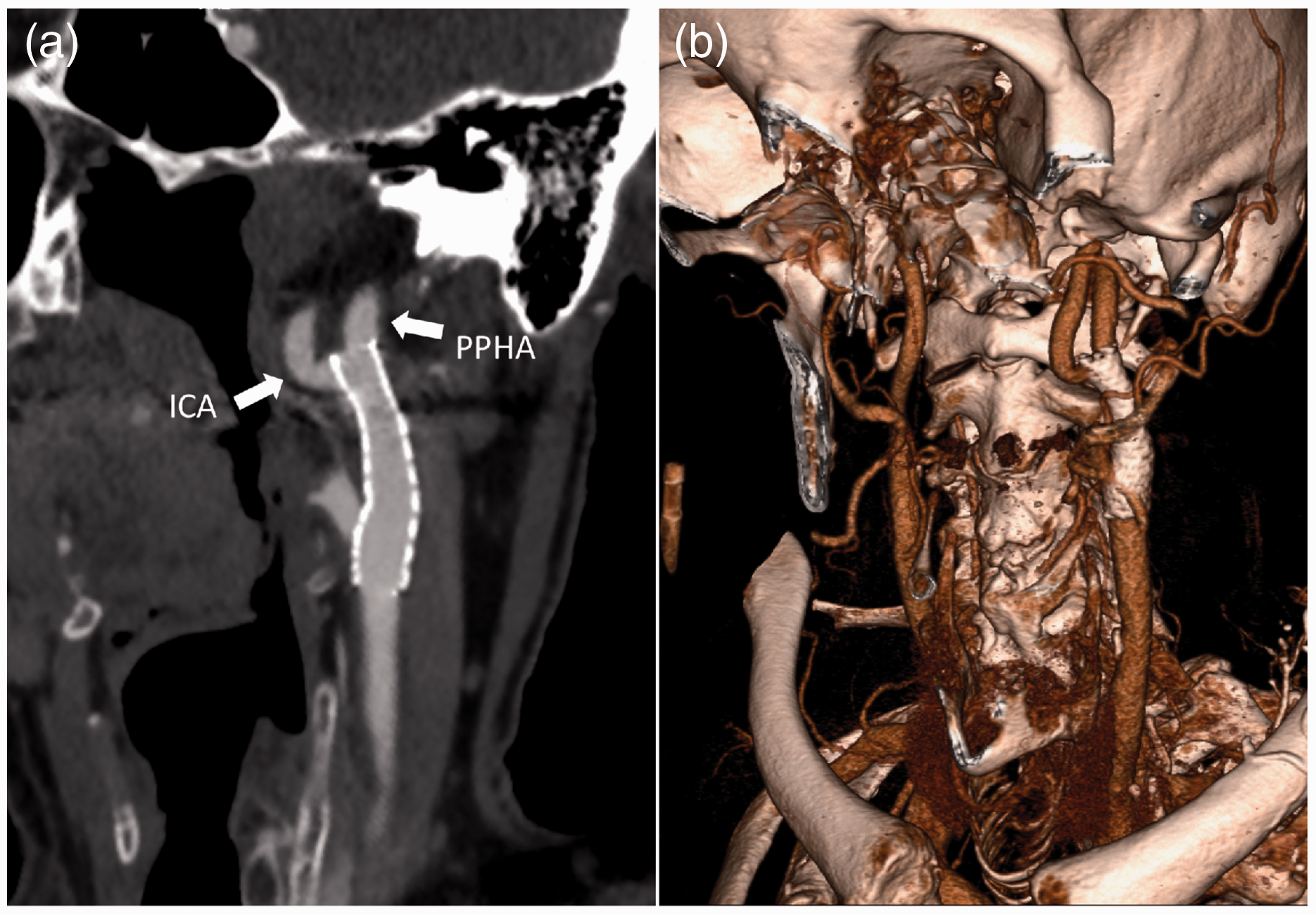
(a) Six months follow-up CT angiography showing excellent position of the stent, with partial jailing of the ICA due to anatomical reasons, and complete coverage of the symptomatic atherosclerotic lesion. (b) 3D reconstruction providing the topographical overview.
Discussion
Management of carotid artery stenosis in the presence of PPHA requires special considerations, mostly due to the frequently high anatomic localization of the lesion, and the fact that the posterior cerebral blood supply often depends entirely on the hypoglossal artery.
Since the first published case of carotid endarterectomy (CEA) in the presence of PPHA in 1978, 3 17 more cases have been reported in the literature (Table 1).4–20 The majority of patients were treated for symptomatic stenosis. Data on the perioperative use of a shunt showed that a common carotid artery (CCA) to PPHA shunt were placed in six cases, 3 , 10 , 14 , 15 , 18 , 20 a CCA–ICA in four cases, 5 , 19 while Hatayama et al. 8 reported the placement of a T-shaped shunt to both the ICA and PPHA. Three cases were performed without shunting, 6 , 7 , 9 , 12 while shunt usage on the remaining two cases was not reported. 4 , 16 Most of the authors provided no detailed information on the reason to choose the shunting target artery, which is one of the main perioperative issues, especially in patients with high lesions operated under general anesthesia. After 2009, there are only three relevant reported cases of CEA, 11 , 12 , 20 suggesting a swift in practice towards endovascular treatment.
Reported cases of CEA in the setting of PPHA.
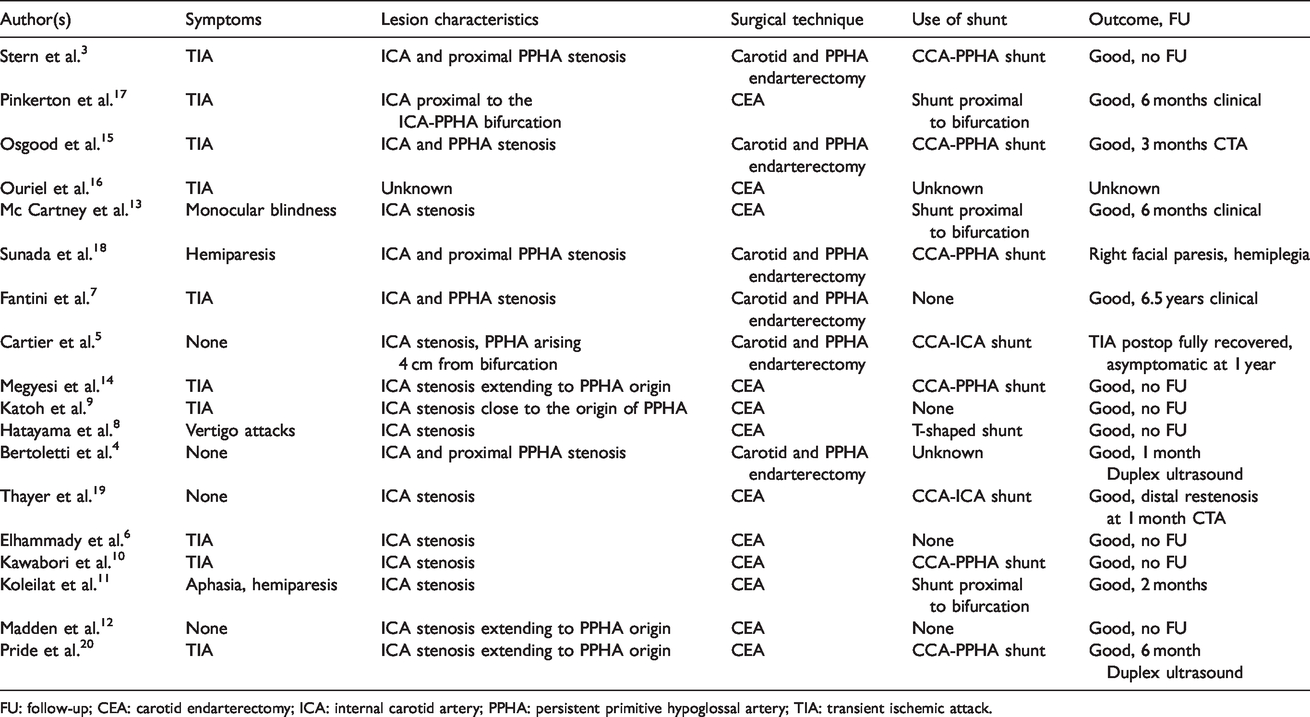
FU: follow-up; CEA: carotid endarterectomy; ICA: internal carotid artery; PPHA: persistent primitive hypoglossal artery; TIA: transient ischemic attack.
Table 2 summarizes the reported cases of CAS in the context of PPHA. Since the first published case of CAS in the presence of PPHA in 2008, 21 nine more cases have been reported in the literature.22–30 All cases but two were treated for symptomatic stenosis. Although the need for cerebral protection during CAS is well established, the choice between proximal occlusion devices, flow-reversal or distal filters is still debated and usually based on anatomic criteria, plaque characteristics and local expertise.
Reported cases of CAS in the setting of PPHA.
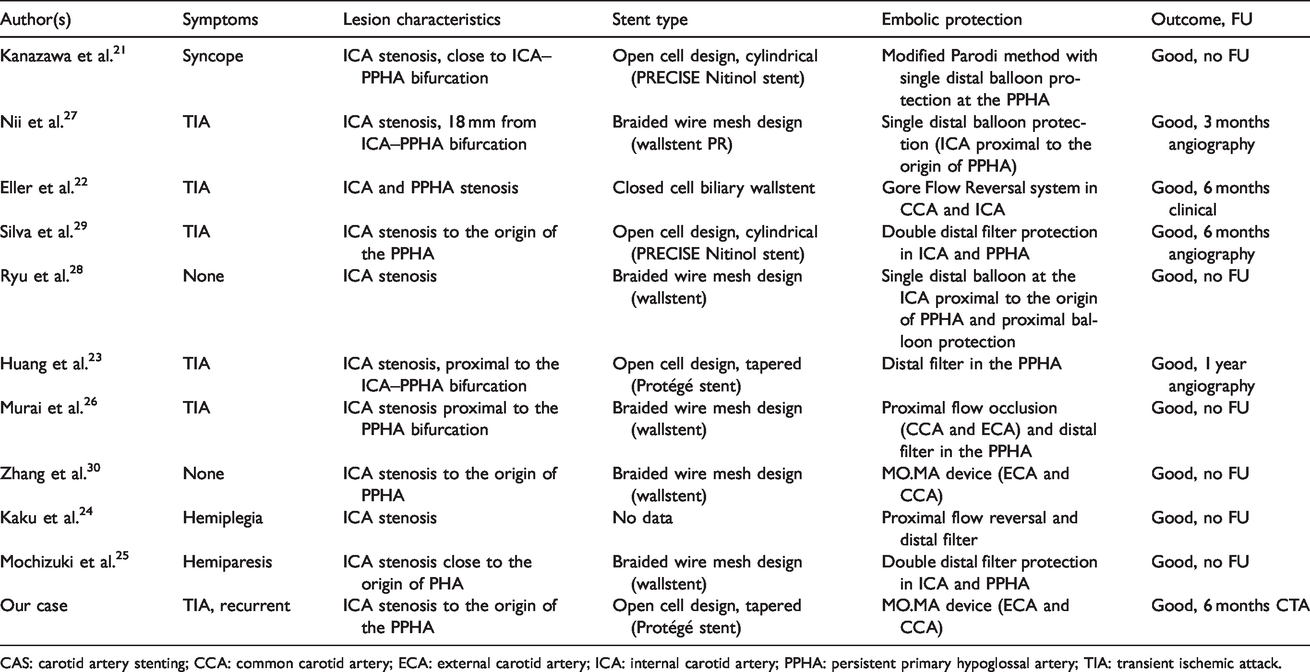
CAS: carotid artery stenting; CCA: common carotid artery; ECA: external carotid artery; ICA: internal carotid artery; PPHA: persistent primary hypoglossal artery; TIA: transient ischemic attack.
In this review, the data on the use of embolic protection methods show that distal balloon protection was used in three cases, 21 , 27 , 28 in one of them combined with proximal occlusion, 28 distal filter in four cases, 23 , 25 , 26 , 29 in one of them combined with proximal occlusion, 26 flow reversal system in two cases, 22 , 24 while Zhang et al. 30 reported the use of a MOMA device. Most of the authors employed a wallstent, 22 ,25–28, 30 in two cases a PRECISE Nitinol stent was placed, 21 , 29 a Protégé stent in one case, 23 while the type of stent used in the remaining case is not reported. 24
Our patient had recurring neurologic symptoms over the past three years despite best medical treatment, so the indication to intervene was barely argued. During discussion in the interdisciplinary vascular board, focus was put on the high localization of the lesion, which would necessitate CEA under general anesthesia and shunt protection. The extent of the unstable carotid plaque from the ICA to the PPHA bifurcation requires separate distal control of the PPHA and distal ICA, with an inherent uncertainty of which should be the target artery to shunt. This taken into account, along with the patients’ co-morbidities and preference, led us to propose an endovascular approach. Plaque extension and quality led to the decision to use a flow reversal device for cerebral protection, rather than a double distal filter, which would necessitate crossing twice an unstable carotid plaque. Using these endovascular techniques, clinical and neurological outcomes were excellent and uneventful.
Conclusion
Treatment of symptomatic carotid artery stenosis in the presence of a PPHA can be challenging. Management should be driven considering patient co-morbidities and clinical presentation, and the anatomical localization of the lesion as well as local expertise. In the case of a high origin of the PPHA, CAS with the use of a proximal cerebral protection device is probably the preferred and simplest approach.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.