
Abstract
Introduction
Use of complementary and alternative medicine (CAM) therapies had been described in patients with disabling, chronic and painful conditions; these characteristics define the majority of vascular surgery (VS) entities. A lack of disclosure about CAM use from patients has been universally cited and may impact effective patient–doctor communication. Our primary objective was to describe CAM use, modalities, perceived benefits, safety, and associated factors among adult patients attending a VS outpatient clinic; we additionally explored patient’s attitudes about CAM disclosure with their primary vascular surgeon.
Methods
This cross-sectional study invited 223 consecutive outpatients to an interview where the ICAM-Q (International Complementary and Alternative Medicine Questionnaire) and the PDRQ-9 (Patient-Doctor Relationship Questionnaire-9 items) were applied. In addition, sociodemographics, vascular disease and treatment-related information, comorbidity, and disease severity characteristics were obtained. Appropriated statistics was used; multiple logistic regression analysis identified factors associated to CAM use. All statistical tests were two-sided, and a p value ≤ 0.05 was considered significant. IRB approval was obtained.
Results
Patients recruited were primary females (69%) and had a median age of 65 years (54–75). Most frequent vascular diagnoses were chronic venous insufficiency (36.2%) and peripheral artery disease (26%). There were 104 (46.6%) patients who referred CAM use, primarily self-helped practices (96%), and use of herbal, vitamins, or homeopathic medicines (23.7%). Overall, the majority of the patients perceived CAM modalities helpful and 94.6% denied any adverse event. Female sex (OR: 1.768, 95% CI: 0.997–3.135, p = 0.051) and hospitalization during the previous year (OR: 3.173, 95% CI: 1.492–6.748, p = 0.003) were associated to CAM use. The majority of the patients (77%) agreed about CAM disclosure with their primary vascular surgeon; meanwhile, among CAM users, up to 54.9% did not disclose it, and their main reasons were “Doctor didn’t ask” (32%) and “I consider it unnecessary” (16%). The patient–doctor relationship was rated by the patients with high scores.
Conclusions
CAM use is frequent and perceived as safe and beneficial among VS outpatients; nonetheless, patients do not disclose CAM use with their primary vascular surgeons, and a wide range of reasons are given by the patients that prevent effective and open communication.
Keywords
Introduction
Vascular surgery (VS) is a specialty that deals with the diagnosis and management of disorders of the arterial, venous, and lymphatic systems and that includes more than 30 entities.1,2 In addition to surgical and endovascular interventions, the management of VS patients includes the identification and modification of relevant risk factors as well as long-term pharmacological and non-pharmacological treatments; this requires the awareness of specialists to the potential of drug interactions and to patient’s adherence to their recommendations.3,4 Patients with VS-related conditions frequently experience pain, impaired function, disability, and multi-comorbidity.5–7 These are known to be associated with the use of alternative medicine. 8
Complementary and Alternative Medicine (CAM) is a group of diverse medical therapies, interventions, treatments, practices, and products that are not considered as part of conventional medicine. 9 CAM modalities have traditionally been classified into five categories: biology-based therapies such as herbal medicine; manipulative and body-based practices that involve chiropractors, acupuncturists, and physiotherapists; mind-body interventions such as spiritual healing, relaxation techniques, and praying; energy therapies such as yoga and Tai Chi; and whole medical systems highly represented by homeopathy.9,10 CAM therapies are gaining popularity worldwide with approximately 40–60% of adults using different CAM modalities in the United States.11,12 Studies have shown that patients with chronic conditions, poorer health status, and uncontrolled pain10,11 may be more likely to seek and use CAM. All of the above characteristics are almost universal in some VS-related diseases. Moreover, CAM treatments have the potential to interact with traditional drugs or to create treatments delays or withdrawals from traditional treatments. 13
Finally, in recent years, patient-centered care has been proposed as the optimal conceptual model of care for patients affected by chronic diseases. 14 It is defined as the clinical treatment provided by medical professionals, which focuses on respecting patients’ preferences, desires, and values. The model relies on a good patient–doctor relationship (PDR), which should have the following characteristics: continuity of care, patient and doctor agreement on the clinical problem and its treatment, and trust in open communication between the patient and the primary physician. 15 A good PDR is highly valuable in itself and also due to its positive impact on health outcomes. 16 Nonetheless, lack of disclosure about the use of CAM from patients has been universally cited, 17 which may subsequently affect the PDR.
The primary objective of this study was to describe the use of CAM, its modalities, perceived benefits, safety, and its associated factors among adult outpatients currently being attended at the VS department in our institution. We also aim at exploring patients’ attitudes to disclosure of CAM use to their primary vascular surgeons and the potential association between CAM use and the PDR.
Methods
Ethical considerations
The internal review board of the Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán (INCMyN-SZ) approved the study (reference number: SCI-3043-19-20-1). All the patients included in the study provided written informed consent.
Study design, setting, and study population
This cross-sectional study was performed between September 2019 and March 2020 at the outpatient clinic of the Department of Vascular Surgery of the INCMyN-SZ, located in Mexico City. The VS outpatient clinic attends to 50 − 60 patients daily, three days per week.
During the study period, consecutive patients with at least six months of follow-up at the VS outpatient clinic were invited to participate. The exclusion criteria included patients on palliative care and those with unstable comorbid conditions requiring significant changes in their treatment or hospitalization at the beginning of the study.
Patient’s assessments and data collection
Patients underwent in-person interviews for the purposes of socio-demographic data collection, primary diagnosis of vascular disease and disease duration, vascular disease-related treatment, comorbidity, and severity of the characteristics of the disease (surgery indication/intervention during the previous year and hospitalization during the previous year). This has been presented in Table 1. In addition, the Spanish version of the following questionnaires and scales were applied: The International Questionnaire on use of Alternative and Complementary Medicine (ICAM-Q),18,19 the patient–doctor relationship questionnaire-9 items (PDRQ-9), 15 the Health Assessment Questionnaire (HAQ), 20 and two visual analogue scales (VAS): one for pain (pain-VAS) 21 and one for adherence to treatment.
Comparison of characteristics between patients with and without recent (past three months) CAM use.
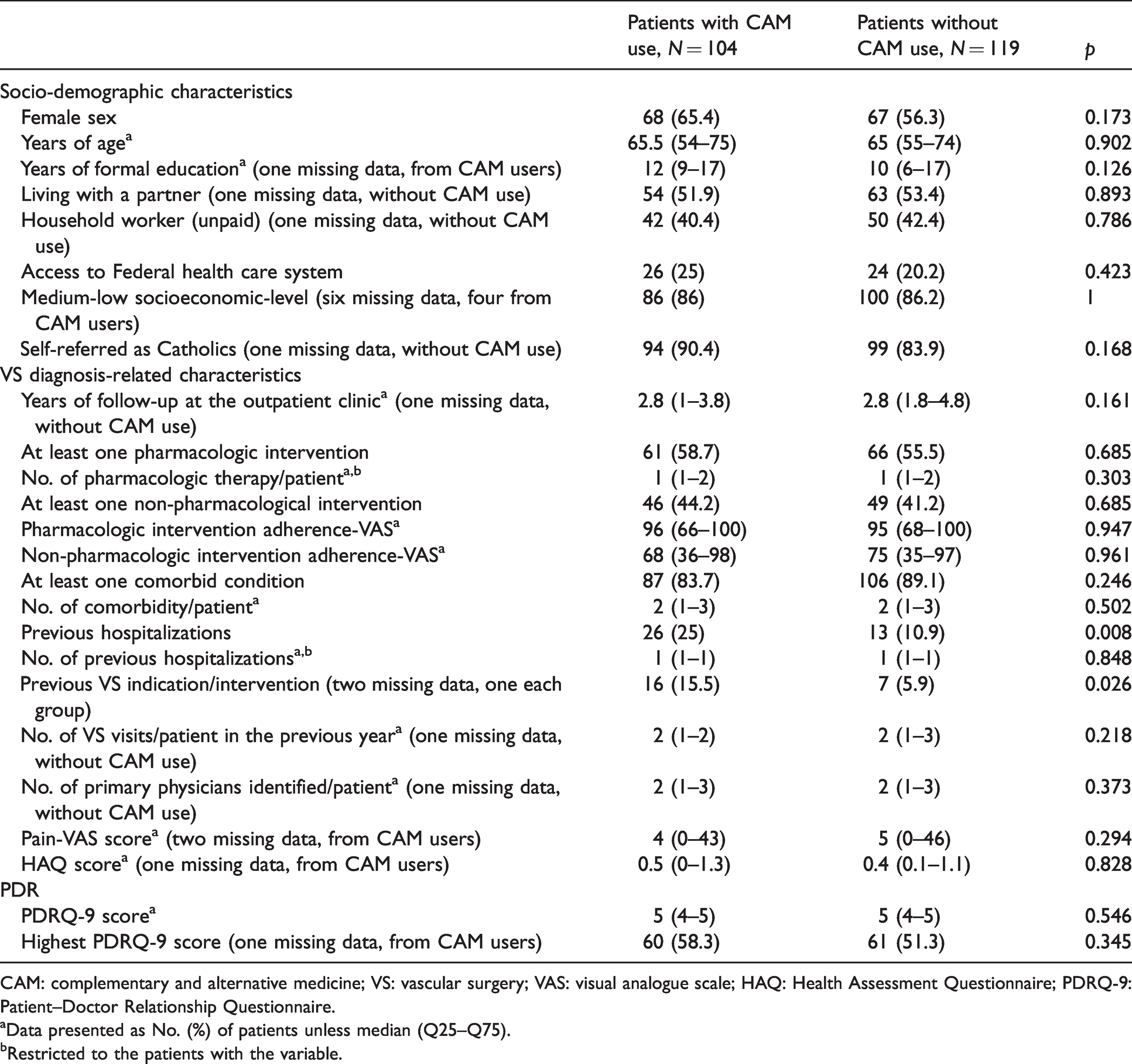
CAM: complementary and alternative medicine; VS: vascular surgery; VAS: visual analogue scale; HAQ: Health Assessment Questionnaire; PDRQ-9: Patient–Doctor Relationship Questionnaire.
aData presented as No. (%) of patients unless median (Q25–Q75).
bRestricted to the patients with the variable.
Instruments description
International Questionnaire on use of Alternative and Complementary Medicine (ICAM-Q). 19
The questionnaire has four main sections: (1) recent visits to different providers of CAM treatment within the past months (12 and 3 months, respectively); (2) CAM treatment received from a physician in the past 12 and 3 months, respectively, that includes any of the following five: manipulation, homeopathy, acupuncture, herbs, or spiritual healing; (3) consumption of medicinal products derived from herbs, vitamins, minerals, or homeopathic medicines within the past 12 and 3 months, respectively, and the main reason for their last use; and (4) self-helped practices implemented by patients that promote well-being in the past 12 and 3 months, respectively.
The frequency of use and level of benefit received were also explored. We provided an additional survey to patients, locally designed, to investigate the adverse events related to CAM use and patient perception about CAM disclosure with the attendant vascular surgeon.
Patient–Doctor Relationship Questionnaire-9 items. 15
The PDRQ-9 assesses the quality of the patient–doctor relationship during a medical encounter, through the quantification of the patient’s opinion regarding communication, accessibility, trust, and satisfaction with the doctor. The global score varies from 1 to 5 with higher scores translated into a better PDR.
Health Assessment Questionnaire. 20
The HAQ is a 20-item questionnaire that grades patient’s limitation to perform activities of daily living. Scale’s response varies from 0 (without disability) to 3 (severe disability to carry out the activity).
Adherence-VAS
Two 0–100 mm scales were used to assess adherence to pharmacologic strategies and to non-pharmacologic strategies, with 100 indicating the best compliance with either treatment, each.
Pain-VAS
The pain scale assessed “today” pain on a 100-mm horizontal VAS, with “no pain” at the left end and “worst possible pain” at the right end, with the latter corresponding to 100 mm. 21
Sample size calculation
We estimated the sample size to detect CAM use in the VS outpatient clinic, considering a prevalence of 40% (without praying category) to 80% (with praying category), based on local experience in rheumatoid arthritis patients. We obtained 209 − 292 patients with 95% confidence level and 5% precision. Moreover, to detect an effective size of 17% as an absolute difference in the percentage of patients with the highest PDRQ score between patients with and without CAM use, we estimated a sample size of 223 patients and added 15% for possible missing data, providing a sample size of 256 patients.
Enrollment of patients was halted on March 17 because of the COVID-19 pandemic. The VS outpatient clinic was temporarily suspended, and 223 patients were recruited. The number of patients included in the study allowed us to have a precision of 4.79 (for CAM use including praying category) and 5.87 (for CAM use excluding praying category). Finally, the distribution of the best PDRQ-9 score between CAM users and non-users obtained allowed us to have a power of 0.3 in a one-tailed test.
Statistical analysis
Descriptive statistics was used with frequencies and percentages for dichotomous variables and mean ± standard deviation or median (Q25–Q75) for the continuous variables, with normal or abnormal distribution, respectively.
CAM users were defined as patients who gave a positive answer to at least one of the four sections of ICAM-Q for the past three months. The number of CAM users was also defined by excluding the prayer category, and analyses were repeated. The results were similar. At the “Results” section, CAM use excluding the prayer category will be presented (unless otherwise indicated).
The characteristics of patients with and without CAM use were contrasted with the χ 2 test for the categorical variables, Student t-test for the continuous variables with a normal distribution, and the Mann–Whitney U test for the continuous variables with an abnormal distribution.
Multiple logistic regression analysis (stepwise) was used to identify factors associated with CAM use. The variables included were: females, age, years of formal education, socioeconomic status, religious beliefs, years of follow-up at the outpatient clinic, multi-comorbidity, previous hospitalizations, previous VS indication/intervention, pain-VAS, and HAQ scores. Previously, correlations between the variables were analyzed, and when appropriate (Pearson correlation ≥ 0.80), one of them was selected according to its clinical relevance.
All the statistical tests were two-sided, and a value of p ≤ 0.05 was considered significant. The statistical analyses were performed using the SPSS/PC program (v. 17.0; Chicago, IL, USA).
Results
Population characteristics
During the study period, 228 patients were invited to participate and 223 agreed. Patients were primarily females (135 [60.5]), had medium-low socioeconomic status (186 [86.1%], six missing data), and self-referred being Catholics (193 [86.9%], one missing datum). Meanwhile, few of them were household workers, which was defined as performing unpaid work in or for a household (92 [41.4%], one missing datum), and had access to Federal health care system, which was defined as having 100% gratuity in hospitalizations/consultations, laboratories, and medical interventions (50 [22.4%]). Moreover, median age was 65 years (54–75), and the number of years of formal education was 12 (6–17). The VS diagnosis is depicted in Supplementary Table 1 (see additional file 1), and the most frequent diseases were chronic venous insufficiency in 81 patients (36.2%), and peripheral artery disease in 58 patients (26%). The median of the follow-up at the VS outpatient clinic was 2.8 (1.8–4.8) years. Majority of the patients received at least one pharmacologic intervention (127 [57%]), and to a lesser degree, at least one non-pharmacologic intervention (95 [42.6%]). These are summarized in Supplementary Tables 2 and 3 (see additional file 1), respectively. Patients were non-adherent to both interventions (non-adherence was defined as adherence-VAS < 80 mm), and the medians for their adherence-VAS were 95 mm (67–100) and 70 mm (36–97), respectively. Majority of the patients had at least one comorbid condition that was defined as a specific additional diagnosis documented after chart review, irrespective of a treatment indication (193 [86.5%]). These are summarized in Supplementary Table 4 (see additional file 1), and number of comorbidities/patient (median) was three [2–3]. Considering the severity of the disease, a minority of the patients (39 [17.5%]) had been previously hospitalized; nevertheless, 23 (10.4%) patients had VS indication/intervention during the previous year. Patients referred to have pain under control that was defined as pain-VAS ≤ 15 mm (median of pain-VAS was four [0–43]), 22 adequate physical function that was defined as HAQ score ≤ 0.5 (HAQ: 0.5 [0.1–1.25]), 22 and a good PDR (PDQR-9 score: 5 [4–5]). One hundred and twenty-one patients (54.5%) scored the highest value in the PDRQ-9.
CAM prevalence, modalities, perceived benefits, and safety
CAM prevalence
There were 104 patients (46.6%) who confirmed the use of CAM in the past three months. When the prayer category was considered, 198 patients (88.8%) confirmed the recent use of CAM.
CAM modalities and perceived benefits
Figure 1 summarizes the distribution of the CAM modalities. Among the 198 patients with recent CAM use (including praying), self-helped practices were reported by 190 (96%) patients, use of herbal, vitamins, or homeopathic medicines were reported by 47 (23.7%) patients; meanwhile, 38 (20%) and 34 (17.2%) patients were receiving complementary therapies from physicians and visiting healthcare providers, respectively. Figure 2 describes the patients’ distribution among the categories within each section of the ICAM-Q.
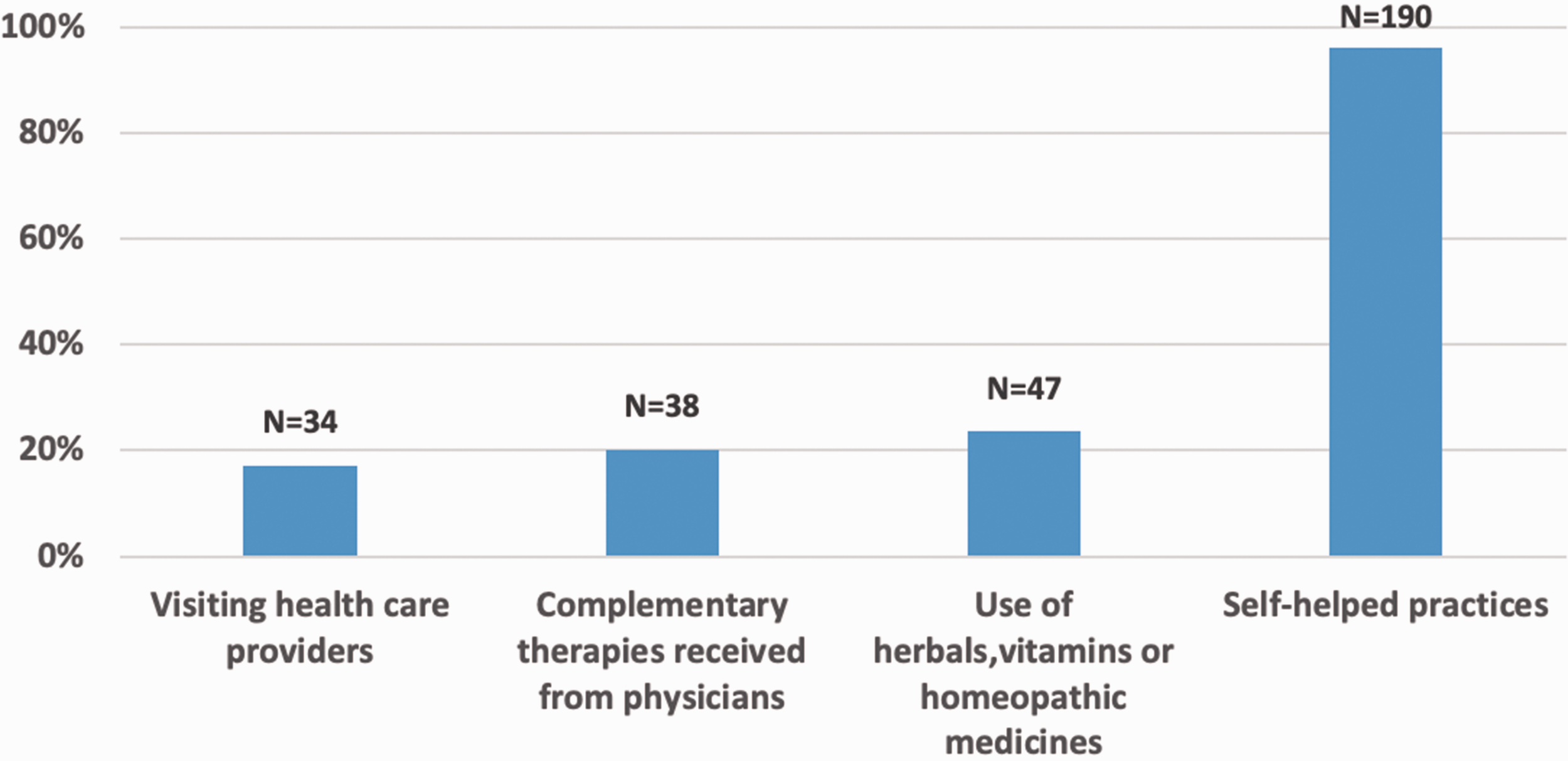
Distribution of patients among the four sections of the ICAM-Q.
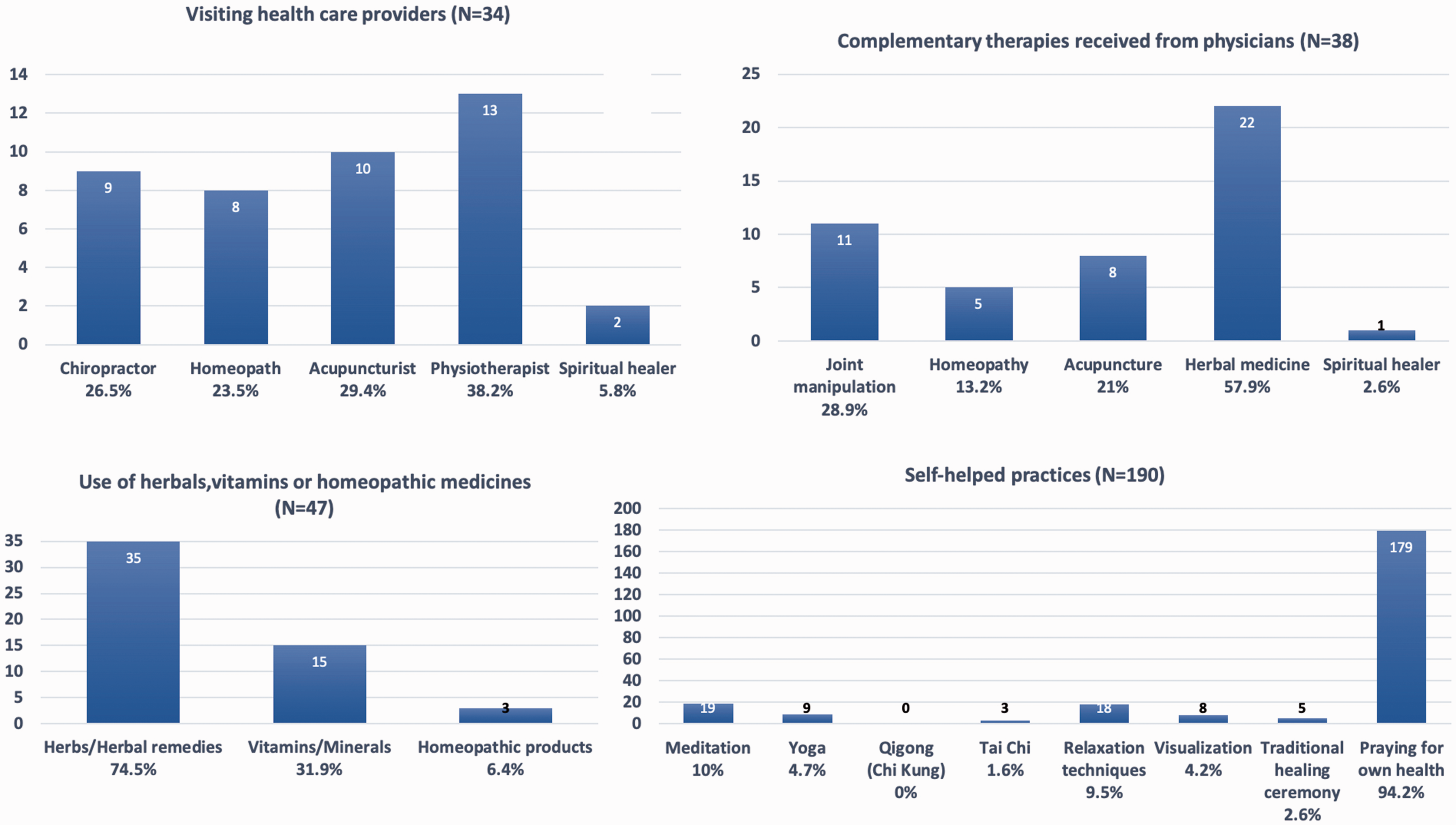
Distribution of patients among the categories within each section of the ICAM-Q.
Figure 3 shows patients experiences on CAM use and patients’ perceived benefit. The most frequent experiences include visiting a physiotherapist at the “visiting health care providers” section; herbal medicine at the “complementary therapies received from physicians” section; herbs/herbal remedies at the “use of herbal medicine, vitamins/minerals or homeopathic medicines” section; praying for own health at the “self-helped practices” section. Majority of the patients perceived the modalities as being “very or somewhat helpful”, and some differences were seen among modalities.
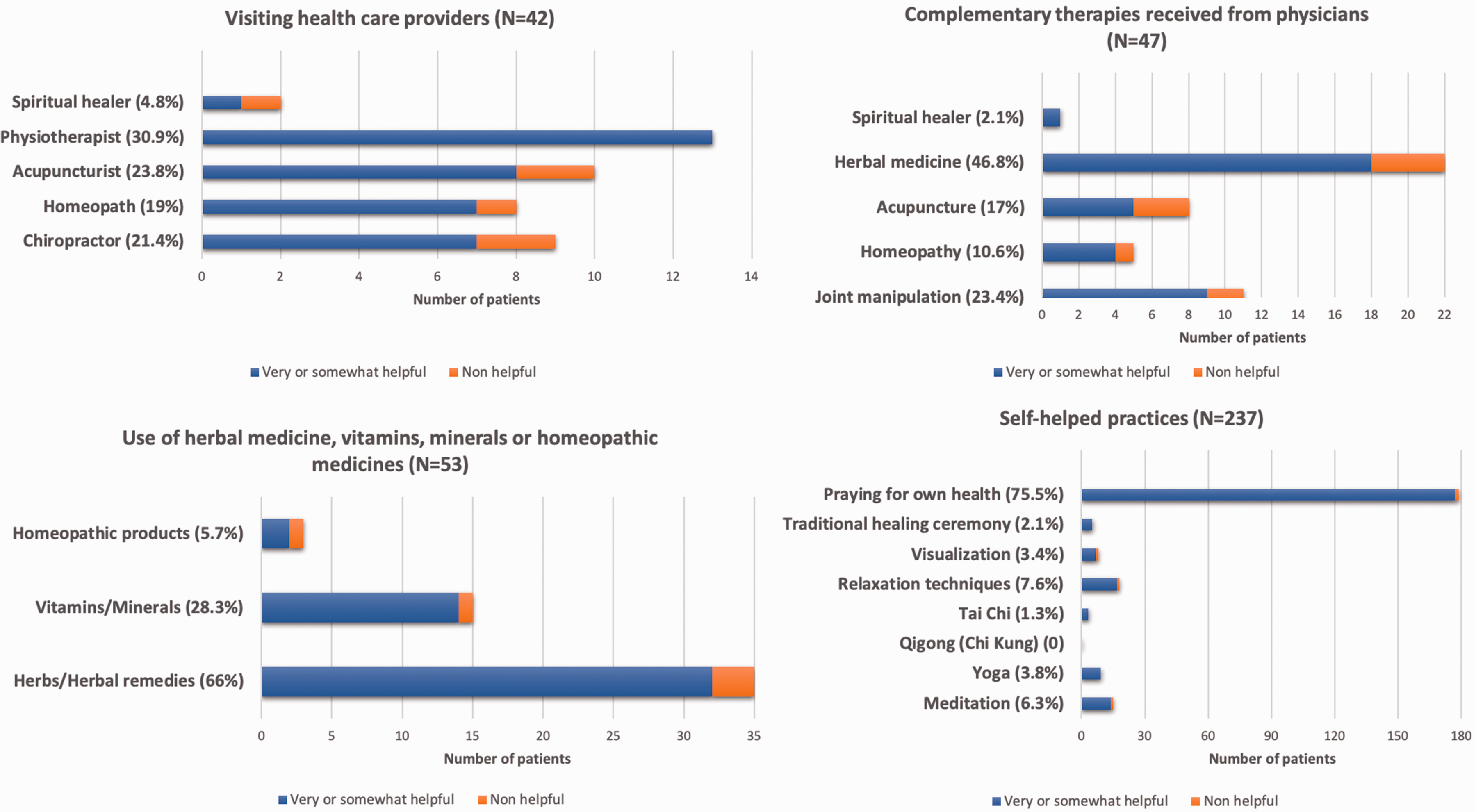
Patients experiences about CAM perceived benefit.
CAM perceived safety
Among the 104 patients who confirmed the use of recent CAM, 11 (10.6%) did not provide data about the perceived safety. Majority of the remaining patients (88 [94.6%]) denied any adverse event.
Factors associated with CAM use
The characteristics of the patients with CAM use (excluding praying) were compared to those without CAM use and are summarized in Table 1. Briefly, patients with CAM use had a more frequent previous hospitalization (25% vs. 10.9%, p = 0.008) and previous VS indication/intervention (15.5% vs. 5.9%, p = 0.026). Furthermore, there was a tendency of seeing a higher (median, IQR) number of comorbidities/patient among CAM users compared to patients without CAM use: 3 (2–3) vs. 2 (1–3), p = 0.082.
Female sex (OR: 1.768, 95% CI: 0.997–3.135, p = 0.051) and hospitalization during the previous year (OR: 3.173 95% CI: 1.492–6.748, p = 0.003) were identified as the factors associated with CAM use.
Patients’ attitudes about CAM disclosure with their primary vascular surgeon
There were 218 patients with data on patients’ disclosure about CAM with their primary vascular surgeon. Majority of them (168 [77%]) agreed on the disclosure. Among those who disagreed, the primary reasons were fear of being nagged (44%) and fear of having their institutional health care being suspended (18%) as shown in Figure 4. Nonetheless, majority of CAM users (N = 104) did not disclose it with their primary vascular surgeon (54.9%), and their main reasons were “Doctor did not ask” (32%) and “I consider it unnecessary” (16%).
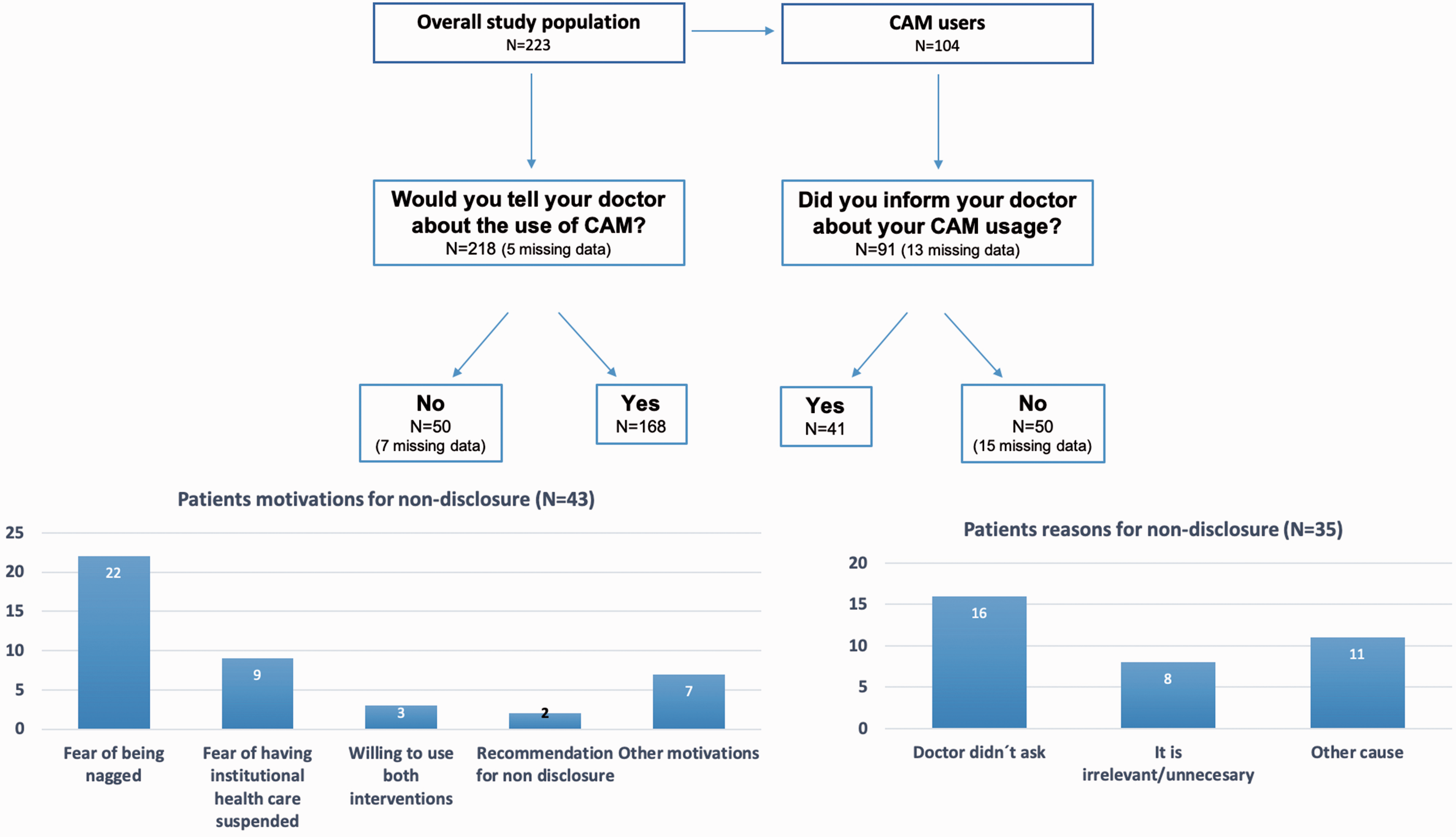
Patient’s attitudes about CAM disclosure with their primary vascular surgeon.
Association between CAM use and the PDRQ-9 score
There were neither differences in the median (Q25–Q75) of the PDRQ-9 global score (5 [4–5] vs. 4.9 [4.2–5]) nor in the individual item’s scores, particularly items three (patient’s perceived trust in the physician: 5 [4–5] vs. 5 [4–5]) and eight (patient’s satisfaction with treatment: 5 [4–5] vs. 5 [4–5]) among the patients who agreed on the disclosure of the use of CAM and their counterparts. Similarly, no differences were found in the PDQR-9 global score (5 [4–5] vs. 5 [4–5]), the scores of item three (5 [4–5] vs. 5 [4–5]) and item eight (5 [4.3–5] vs. 5 [4–5]) between the patients who use CAM and disclose it to their vascular surgeon, and those who did not disclose its use (p > 0.05 for any comparison).
Discussion
The present study revealed that a significant proportion of outpatients attending a VS clinic used different CAM modalities and remedies. Self-helped practices and the use of herbal, vitamins, or homeopathic medicines were the most frequently used ones. Patients perceived CAM modalities as helpful and safe although some differences were seen among the modalities. Female sex and hospitalization during the previous year were significantly associated with CAM use in our population. Patients agreed that CAM use should be disclosed to their vascular surgeons. Considering those who disagreed, the primary reasons were fear of being nagged and of having their institutional health care being suspended. However, a minority of the CAM users indeed disclosed their use to their primary vascular surgeons. Patients rated positively for PDR though no further conclusions on the impact of CAM use and the patient’s CAM disclosure could be obtained.
This is the first study that addresses CAM use in a VS outpatient clinic. The surgical discipline focuses on surgical and endovascular interventions; nevertheless, patients’ care extends beyond the surgical domain. Patients may benefit from integration in an outpatient clinic where a surgeon’s competencies include defining the optimum time of intervention, 1 immediate as well as long-term post-surgical patient assessments, and the judicious use of non-surgical interventions including the administration of drugs that have the potential to interact with some CAM modalities and impact the outcomes.10,23
In the last decades, the use of CAM has been increasingly recognized, particularly among patients suffering from chronic, and disabling conditions such as rheumatoid arthritis, cancer, diabetes mellitus, and cardiovascular disease.10,24 These entities are frequent sources of patients’ referral to a vascular surgeon’s assessment. Our study found that approximately half of the patients evaluated confirmed the recent use of CAM, and the percentage increased to 88.8% when the prayer category was included. This is in accordance with the results from previous studies10,11 and confirms higher levels when prayer is considered as a CAM modality. 25 Considering the CAM modalities, our patients confirmed the frequent use of self-helped practices as well as herbal, vitamins, and/or homeopathic medicines. Prayer is highly influenced by the local culture, and the use of herbal and homeopathic medicines was similar to those described in other regions. Spinks et al. 26 reported that 25% of Australian patients suffering from diabetes mellitus and cardiovascular diseases used nutritional supplements while 16% used vitamin, mineral, or herbal supplements. Likewise, Rhee et al. 27 reported herbal therapies as the most common type of CAM use in diabetic patients. In USA, patients with cardiovascular conditions frequently used herbal products, among those who confirmed the use of CAM. 28 Our patients perceived that the use of CAM was helpful and safe. CAM has been perceived as having few side effects. 17 In furtherance, CAM treatment can cause gastrointestinal side effects 29 in addition to their potential interaction with drugs (such as aspirin) that are frequently prescribed by vascular surgeons.10,30 Therefore, there have been cautions from regulatory agencies against their use. 31 Finally, we found that female sex and previous hospitalizations were associated with the use of CAM. Previous studies have shown that women fit the profile of users of CAM in the clinical context of rheumatic diseases. 32 Furthermore, previous hospitalization may be considered a surrogate of a more aggressive disease phenotype and poorer health status, and the latter is associated with CAM use in patients with chronic hepatitis C. 33
The second important finding of our study was that majority of the patients agreed on CAM disclosure to their vascular surgeons. Among those who disagreed, the primary reasons were fear of retaliation from the physician. Moreover, a few of the CAM users disclosed it, and those who did not mentioned that their doctors did not ask and that it was irrelevant/unnecessary. The lack of disclosure of CAM use from patients has been described as almost universal 34 at rates similar to ours. 35 This was confirmed by Mexican patients with rheumatic diseases with universal health coverage. 36 All the reasons mentioned by our patients had already been described in a review of qualitative and quantitative studies by Robinson et al., 34 who grouped patient’s motivations into three areas: “negative response from the medical practitioner,” “patient’s perception that the medical practitioner did not need to know about CAM use,” and “the medical practitioner did not ask and appeared disinterested.” Although the review includes patients with a wide variety of medical conditions, our findings suggest that the results can be extended to patients with surgical conditions. Nonetheless, compared to our findings, patients’ concern about a negative response from the medical practitioner has been rarely mentioned in other studies.34,37 This may be related to a greater acceptance of alternative therapy in some European countries. 38
Finally, it should be noted that patients rated the PDRQ-9 with outstanding scores, even by those who feared to communicate CAM use or considered it as a personal decision and did not require their primary physician input. We used the PDRQ-9 questionnaire that had shown adequate psychometric properties to assess the construct in Spanish speaking patients although the instrument only considered the patient’s view. 15 This may explain the results. Additionally, patients that are referred to a vascular surgeon may have expectations that are different from those of patients referred to clinicians and may prioritize the outcomes related to the surgical procedure. In a study conducted on patients undergoing pulmonary resection for lung cancer, the duration (shorter) of hospital stay was associated with patient’s satisfaction with the provider of communication. 39 This may not be true for other surgery-related outcomes, such as postoperative complications, that were not associated with patients’ experience, in patients undergoing kidney transplant and lumbar spine surgery.40,41 This highlights the complexity of PDR construct in relation to surgical patients.
The study has limitations that need to be mentioned. First, we used a Spanish translated and an adapted version of the I-CAM-Q that lacks formal validation. The PDRQ-9 is limited to patients’ perspective of PDR. Second, the study has a cross-sectional design, and only associations can be inferred. Third, the study was conducted in a single academic center, where patients referred to the VS outpatient clinic might have particular characteristics; therefore, the results may not be generalized to other populations. Furthermore, Mexican patients with VS-related conditions may have some cultural proximity to specific CAM strategies and may not recognize them as CAM. Finally, the sample size of the study was limited to assessing the impact of CAM use in PDR.
Conclusions
The present study supports that almost half of the patients from a VS outpatient clinic use CAM remedies and strategies either as complements or alternatives of conventional medicine. Patients and their primary vascular surgeons do not enter into a dialog on the use of CAM therapies, and patients affirmed a wide range of reasons that prevent an open communication. It is becoming increasingly clear that patients may have legitimate needs and concerns that are not met by traditional medicine. Adhering to the ethical principle of respect for a patient’s autonomy, surgeons should initiate open discussions with their patients to enable them (the patients) make informed decisions and understand their patients views.
Supplemental Material
sj-pdf-1-vas-10.1177_17085381211006595 - Supplemental material for A comprehensive approach to complementary and alternative medicine usage among patients from a vascular department
Supplemental material, sj-pdf-1-vas-10.1177_17085381211006595 for A comprehensive approach to complementary and alternative medicine usage among patients from a vascular department by Cesar Cuen-Ojeda, Carlos A Hinojosa, Irazú Contreras-Yáñez, Erika Elenes-Sánchez, Casandra Rosas-Ríos, Miguel A Méndez-Sosa, Angel Ballinas-Sánchez and Virginia Pascual-Ramos in Vascular
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.