
Abstract
Objectives
To summarize the experience and midterm outcomes of physician-modified endovascular grafts for zone 2 thoracic endovascular aortic repair.
Methods
A retrospective analysis was conducted of 51 consecutive patients (mean age 57.6 ± 12.5 years, 39 males) treated with thoracic endovascular aortic repair using physician-modified endovascular grafts for reconstructing the left subclavian artery from November 2015 to December 2019. The primary endpoints during follow-up were the overall mortality, aorta-related mortality, and major complications. The secondary endpoints were reintervention and the patency of the target branches, the demographics and technical details were also described and analyzed.
Results
Sixty-three thoracic stent-grafts were deployed in 51 patients and emergency surgery was performed in 10 patients (19.6%). Technical success was 94.1% (48/51). The incidence of perioperative complications was 15.7%, and the 30-day mortality was 0%. At a mean follow-up of 42.0 ± 14.4 months (range, 14–63 months), all the left subclavian arteries remained patent. All-cause mortality was 3.9% (2/51) and not aorta-related deaths. Estimated survival at one and three years was 98.0 ± 1.9% and 96.0 ± 2.8%, respectively.
Conclusions
The physician-modified endovascular grafts is feasible and effective to preserve left subclavian artery in thoracic endovascular aortic repair for aortic arch pathologies with unhealthy proximal landing zone.
Keywords
Introduction
Thoracic endovascular aortic repair (TEVAR) for aortic pathology has become more popular in recent years. Because of its minimal invasiveness, fewer complications, and shorter hospital stays than open surgery, both physicians and patients are more likely to choose TEVAR.1,2 To avoid coverage of any supra-arch artery, conventional TEVAR is limited to zone 3 pathologies far from the origin of the left subclavian artery (LSA; usually ≥15 mm is required). However, real world experience has demonstrated that 26% to 40% of TEVAR procedures require coverage of the LSA to acquire adequate healthy proximal landing zone. 3 The necessity to revascularize LSA remains controversial, but the dominant view seems to be that prophylactic LSA revascularization prior to intentional coverage, unless in an emergency or abnormal anatomy,4,5 as the European Society for Vascular Surgery and the Society for Vascular Surgery suggested.2,6 Several alternative strategies are available to revascularize the LSA while extending the proximal landing zone, such as hybrid operation, the chimney technique, fenestration, and branched stent-grafts. A reasonable amount of data show that physician-modified endovascular grafts (PMEG) can exclude complex aortic aneurysms while providing acceptable mortality and complication rate, even in emergency. 7 However, long-term results remain unknown. This study aims to review and share our experience and midterm outcomes of using the single-fenestrated PMEGs during TEVAR to preserve the LSA for zone 2 of aortic arch pathologies.
Materials and methods
Study design
A retrospective study was conducted of 51 consecutive patients (mean age 57.6 ± 12.5 years, range 18–83 years; 39 males) with various aortic arch pathologies who underwent TEVAR with the PMEGs to revascularize the LSA from November 2015 to December 2019. All patients underwent computed tomography angiography (CTA) to confirm the diagnosis. Indications for PMEGs implantation included the lesions (the penetrating aortic ulcer, the primary intimal tear of the aortic dissection or the neck of the thoracic aortic aneurysm) was located in the lesser aortic arch curvature, and the distance to the origin of LSA was <15 mm that require a seal in zone 2. Emergency surgery was performed for patients with persistent pain, refractory hypertension, or malperfusion syndrome (renal ischemia, bowel ischemia, acute limb ischemia), and so forth. Otherwise, elective surgery was performed as soon as adequate preoperative preparation had been completed.
The protocol and informed consent for this study were approved by the institutional ethics board of our hospital. All patients provided written informed consent for performing the operation and collecting the clinical data.
Sizing and device preparation
By means of a 3D vascular imaging workstation (3mensio Vascular, Pie Medical Imaging, Bilthoven, The Netherlands), center lumen line reconstruction of CTA was the important first step. The aortic diameter and lengths of the landing zones, the position of the lesions, and the optimal position of C-arm projection at tangential view of the aortic arch all required detailed measurements and assessments. Then procedure planning and device sizing were performed.
Thoracic endografts were fully deployed without releasing tip-capture mechanism on a sterile table. According to the previous measurement results, the fenestration had to be marked in its appropriate position on the endografts and damaging of the endografts struts had to be avoided as much as possible. We usually make the fenestration by a thermal cautery instrument (OASIS Medical, Glendora, CA, USA), and try to make it as round as possible and not have struts crossing (Figure 1(a)). The fenestrations were sized 2 mm smaller than the diameter of the LSA bridging stents (usually 8–10 mm). The edge of the fenestration will be reinforced using a radiopaque nitinol snare (Amplatz Goose Neck, ev3, Plymouth, MN, USA) and fixed on the fabric with a continuous running suture of CV-5 (Gore, Flagstaff, AZ, USA) (Figure 1(b)), which can be used as a positioning marker and reduce the risk of joint tear and leakage. A 0.014 inch nitinol guidewire (ASAHI, Nagoya, Aichi, Japan) (Figure 1(c)) was passed into the sheath through the needle hole, which was made on the introducer sheath distal to the section bearing the endograft, to travel through the endograft and transverse the fenestration. Finally, compress the fenestration into a straight line parallel to the long axis of the endografts and keep it on the outermost side, then reload the PMEGs into the delivery system by using the umbilical tape section by section tightening stent-graft carefully (Figure 1(d)).

Device modification (this figure shows the Relay thoracic stent graft). (a) Cauterizing fabric to create a proper fenestration of the LSA; (b) reinforcing the edge of the fenestration by suturing the radiopaque loop of a snare (the red arrow); (c) the finished PMEGs: (1) Tapered tip, (2) Pre-load auxiliary guidewire, (3) Fenestration, (4) Fenestration marker (the loop of a snare). (d) The endograft was reconstrained with 1–0 nylon sutures and reloaded into the conveying sheath.
Several thoracic endografts and bridging stents were selected for use. The thoracic endografts included Relay (Terumo Aortic/Bolton Medical, Sunrise, FL, USA); Valiant (Medtronic Vascular, Santa Rosa, CA, USA); Zenith TX2 (Cook Medical, Bloomington, IN, USA); and Ankura II (Lifetech Scientific Corporation, Shenzhen, China). The PMEGs oversize was <10% for acute aortic dissection and between 10% and 15% for other aortic arch pathologies. 8 The bridging stents included covered stents [Fluency (BD/Bard Peripheral Vascular, Tempe, AZ, USA) or Viabahn (Gore Medical, Flagstaff, AZ, USA)] and bare stents [S.M.A.R.T. (Cordis Corporation, a Cardinal Health company, Santa Clara, CA, USA), Zilver (Cook Medical), or Protege GPS (EV3, Plymouth, MN, USA)].
Technique
All patients underwent heparinization (100 U/kg) after general anesthesia. The left brachial artery (LBA) and one side of common femoral artery (CFA) were punctured or surgically exposed (if the CFA is severely distorted or calcified). A total aortography was performed to evaluate the location of the lesion and the left vertebral artery, and the measurements were re-examined (Figure 2(a)). A Lunderquist guidewire (Cook Medical, Bloomington, IN, USA) was advanced into the ascending aorta from the CFA access through a pigtail catheter. Meanwhile, a Supracore guidewire (Abbott Vascular, Santa Clara, CA, USA) was introduced from the LBA through the true lumen of the aorta into the CFA, and was exteriorized through the 18 Fr sheath of CFA access (Figure 2(b)). Then, a 4 Fr 120 cm length multifunction catheter was inserted along the Supracore guidewire to establish the path from the LBA to the CFA access. The PMEGs was inserted along the Lunderquist guidewire into the descending aorta. At the same time, the pre-loaded guidewire was introduced along with the PMEGs and exteriorized from the LBA access through the 4 Fr multifunction catheter. Rotation of the delivery system could adjust the PMEGs and keep the two guidewires from winding. To reduce the difficulty and risk of operating within the aortic arch, all rotation and adjustment were performed within the descending aorta. Rotation of the PMEGs made the compressed circular mark from an ellipse to a line toward the outer curve of the aorta at the optimal angle of C-arm projection, then the PMEGs was advanced into the aortic arch and the fenestration mark was aligned with the LSA. The PMEGs was partially released to expose the fenestration, and the 4 Fr multifunction catheter and a 6 Fr long sheath were placed along the pre-loaded guidewire through the retrograde LBA and the fenestration of the LSA into the PMEGs lumen, then the PMEGs was fully deployed. The bridging stents was deployed along the Supracore guidewire that replaced the pre-loaded guidewire, and the proximal usually enters into the PMEGs lumen for about 1 cm. The distal should not exceed the origin of the left vertebral artery.

Procedure of fenestrated TEVAR using the PMSGs. (a) Diagnostic angiogram confirmed the type B aortic dissection without adequate landing zone for TEVAR. (b) The Supracore guidewire (black arrow) was introduced from the LBA and exteriorized through the 18 Fr sheath of CFA access. The multifunction catheter (white arrow) was inserted along the Supracore guidewire to establish the path from the LBA to the CFA access. (c) Successful catheterization of the LSA through the fenestration from the retrograde access, and replace the pre-load auxiliary guidewire as the Supracore guidewire wire. (d) Ensuring that the fenestration was oriented toward the LSA by hand injection of iodinated contrast through the 6 Fr sheath placed at the ostium of the LSA. (e) A bridging stent was implanted through LSA fenestration. (f) Final angiogram showing complete exclusion of false lumen.
Follow-up, endpoints, and statistics
All patients had been scheduled evaluation including regular outpatient review and CTA or follow-up at one, three, and six months, and annually thereafter. The primary endpoints during follow-up were overall mortality, aorta-related mortality, and major complications (stroke, paraplegia, or endoleaks). The secondary endpoints were reintervention and the patency of the target branches. Technical success is defined as complete exclusion of the aortic pathology and LSA reconstruction. Categorical data are reported as count (percentage); continuous data are reported as the mean ± standard deviation and/or range. Kaplan–Meier analysis was used to generate estimates for survival.
Results
Patients’ characteristics and demographics
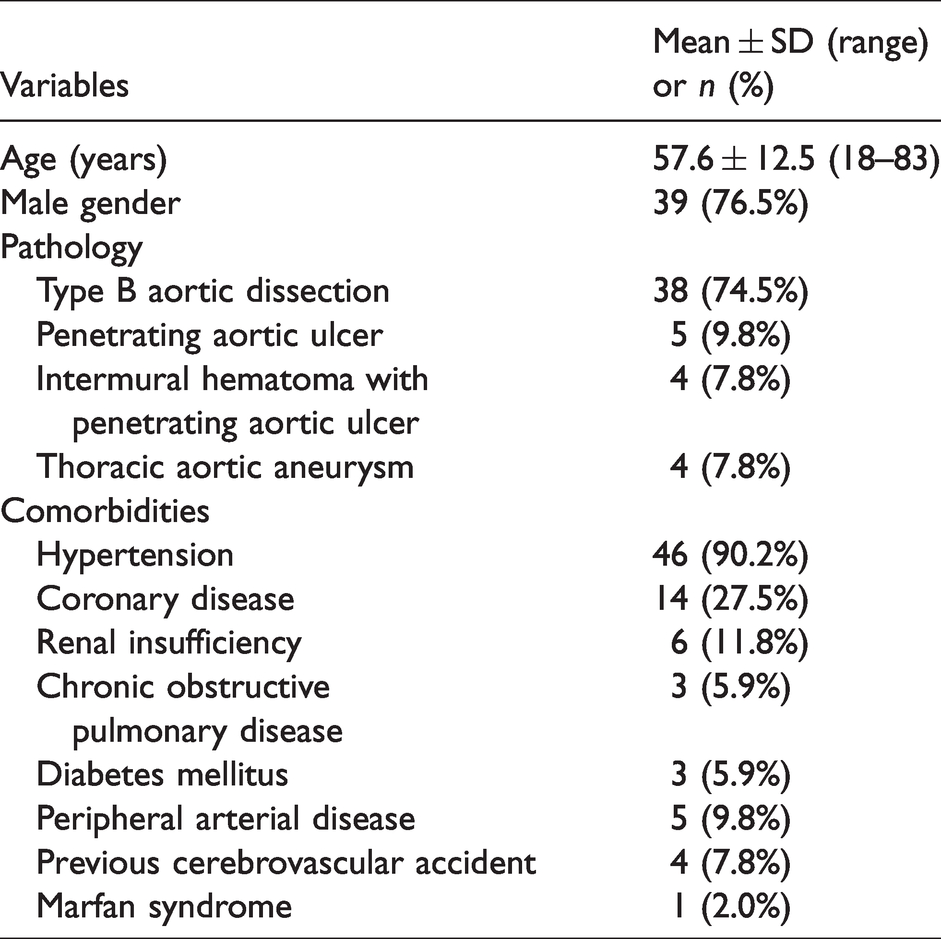
A total of 51 patients were included in the retrospective study. Of these, 38 were type B aortic dissection, 5 were penetrating aortic ulcer, 4 were intermural hematoma with penetrating aortic ulcer, and 4 were thoracic aortic aneurysm. The characteristics of the patients are listed in Table 1.
Patient demographics.
Perioperative outcomes
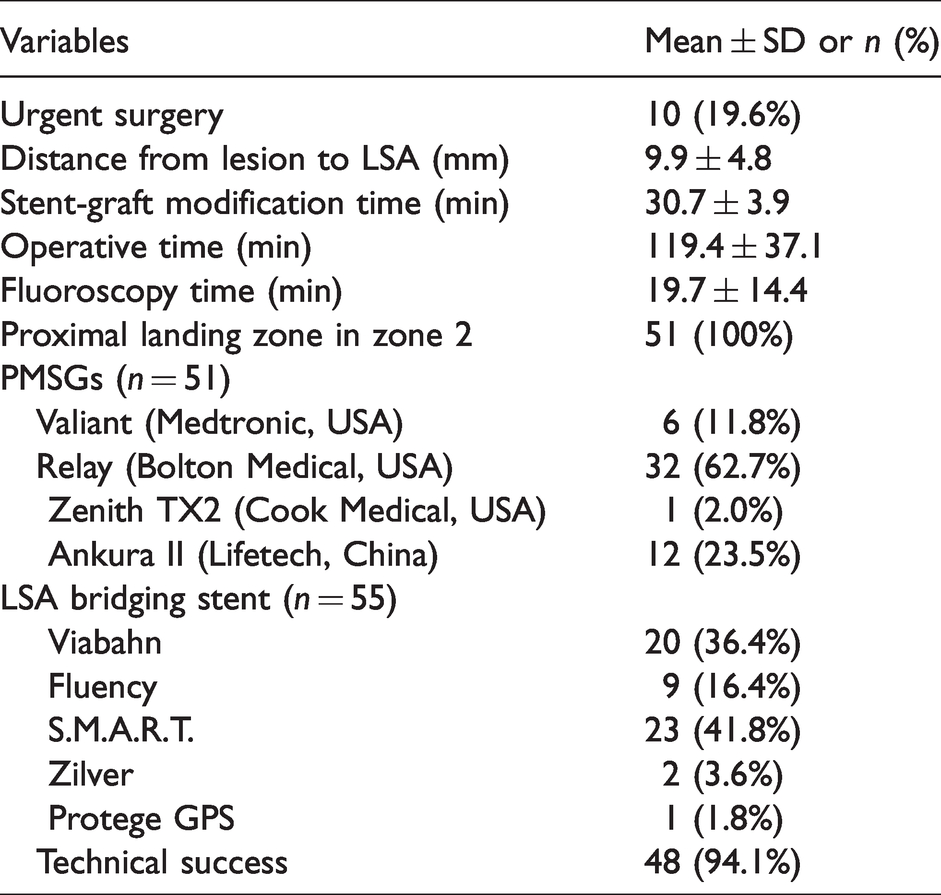
All patients completed surgery and LSA reconstruction was achieved, and 10 (19.6%) of them underwent emergency surgery. The technical success rate was 94.1% (48/51). Two patients were conversion to chimney technique during operation, both due to inaccuracy in early localization, one with unfortunate coverage of LSA and the other with partial coverage of the left common carotid artery (LCCA). An immediate slight proximal type I endoleak was identified but not treated intraoperatively. Mean time of operative and fluoroscopy were 119.4 ± 37.1 min and 19.7 ± 14.4 min, respectively.
The mean distance between the lesion and LSA was 9.9 ± 4.8 mm. All landing zones were in zone 2, and the mean aortic diameter of proximal landing zone was 31.5 ± 2.4 mm. Mean time of stent grafts modifications was 30.8 ± 3.8 min. There was no significant difference in the time of modification and reloading between the four devices. A total of 63 thoracic stent-grafts including 51 PMEGs were deployed in 51 patients, and 12 (23.5%) patients required a second distal aortic stent-graft (included eight covered aortic stent-graft and four bare aortic stent-graft). Twenty-nine (52.7%) covered stents and 26 (47.3%) bare stents were deployed as bridging stents in the LSA, two stents were deployed in 4 (7.8%) patients. All the operative details are shown in Table 2.
Operative details.
Mean length of hospital stay was 14.9 ± 5.0 days (range, 5–28 days). The incidence of perioperative complications was 15.7% (8/51). One (2.0%) type IIIc endoleak at the junction between the bridging stent and PMEGs was sealed by an Amplatzer occluder and several spring coils at postoperative seven days. One (2.0%) patient had a stroke without permanent sequelae after careful treatment. Postoperative elevation of serum creatinine levels was observed in 5 (9.8%) patients (three of them had previous renal insufficiency). One left brachial pseudoaneurysm required surgical repair. During postoperative 30 days, no paraplegia, new endoleaks, retrograde dissection, death or other major complications were observed, the intraoperative proximal type I endoleak disappeared. All bridging stents remained patent.
Midterm outcomes
The mean follow-up was 36.2 ± 13.9 months. Follow-up was available in 6 at ≤ 2 years, 9 at ≤ 3 years, 15 at ≤ 4 years, and 21 at > 4 years. All-cause mortality was 3.9% (2/51), and no aorta-related mortality and no reinterventions. One patient died of an acute episode of COPD at three months and one patient died of renal failure at 17 months after surgery. Estimated survival at one and three years was 98.0 ± 1.9% and 96.0 ± 2.8%, respectively. The patient with a LSA chimney stent developed a type Ia endoleak at the second postoperative year. Three (5.9%) distal stent-graft-induced new entry tears (dSINE) were identified (Figure 3(c)). One patient suffered cerebral ischemia at 12 months and was resolved by carotid artery stent placement, but this was identified as a result of simple progression of carotid atherosclerosis. During follow-up, there has been no ruptures, spinal cord ischemia, new endoleak, stent fracture or migrations, retrograde dissection, or other aortic complications, and all the LSAs remained clinically and radiologically patent (Figure 3(a) and (b)).

Outcomes of CTA follow-up. (a) A type B dissection: the CTA of preoperative and three-year follow-up; (b) a multiple penetrating ulcers (the red arrows shows ulcers): the CTA of preoperative and two-year follow-up; (c) the dSINE was identified after fTEVAR (the yellow arrow shows the tear).
Discussion
Undeniably, conventional surgical repair remains the gold standard for the treatment of aortic arch pathologies. However, with the development of endovascular devices and techniques, more and more physicians try to use endovascular repair to solve complex aortic arch pathologies involving the supra-aortic branches, although all current technologies have their shortcomings. Hybrid surgical debranching procedure is less invasive, and could be the best option in some special situations (such as complex anatomy or variation of the aortic arch), but may still have surgery-related complications.9,10 Chimney technology is a simple, convenient, maneuverable alternative for preservation of supra-aortic branch. But it seems not be the best choice because of concerns about type Ia gutter endoleak. 11 It was usually prepared as a remedy for the failure of fenestrated TEVAR in this study. Custom-made stent-grafts is anticipated, but still limited by long waits, high costs, anatomy, and technical factors. In situ fenestration is relatively simple and has a high technical success rate, 12 but it will temporarily block the branch and may damage the endograft scaffold. The branched endografts are still being investigated and also has high expectations. It is more in line with the anatomical structure of the original artery, and the more sealed and integrated junction between the main body and the branch stent greatly eliminates the risk of the type III endoleak. But several fixed sizes make it unsuitable for complex and variable anatomical lesions.
PMEGs can be carried out rapidly at any time according to the patients’ anatomic pathology and disease status. We have been able to control the time of stent grafts modifications within 20 min through a lot of experience accumulation and process optimization. Especially when it is done in conjunction with anesthesia and tracheal intubation at the same time, there is not much waiting time. Therefore, PMEGs may be able to extend TEVAR indications to patients in emergency or not suitable for other conventional options.
The challenge of deploying PMEGs intraoperatively is to ensure accurate alignment of the fenestration with the LSA ostium, 13 and how to effectively solve the vexing entanglement between pre-loaded guidewire and Lunderquist guidewire. Some useful and import methods and tips for solving these problems have been described in detail in the earlier publication,14,15 and their high technical success rate and favorable safety outcomes are consistent with our experience. The two patients were conversion to a chimney TEVAR during our early experience, with a mismatch in position or misalignment due to failure to use preset guide wire and multiple angles to determine positioning as the main causes.
Four brands of available thoracic stent grafts were selected for fenestration from our experience. Some differences were found during the procedures of graft modification and deployment. The fabric of the Relay thoracic endograft is more suitable for fenestration due to its thickness and tear resistance. 16 And it has a strut on the longitudinal axis to provide more support and positioning on the outer curve of the endograft, but need to be avoided during fenestration. The thin and soft delivery sheath makes the Relay thoracic endograft easier to resheath and clearer to develop under DSA after outside the outer sheath. But owing to the poor support of its soft delivery sheath, the Relay thoracic endograft is considered unsuitable for severe tortuosity of the aortic arch. Therefore, three other thoracic endografts with stiffer delivery sheath that provide more support are used in severe tortuosity of the aortic arch. The Zenith TX2 thoracic endograft has no bare proximal scaffold, so it needs a longer length of zone 2 (the distance between LCCA and LSA) to avoid loose sealing and occlusion LCCA. Sometimes in order to reduce the financial burden of some patients, the Ankura thoracic endograft was chosen, which also has a strut on the longitudinal axis like the Relay thoracic endograft.
It is important for the bridging stent to extend sufficiently into the LSA and the PMEGs to avoid type III endoleak and migration of the PMEGs. The diameter of the LSA bridging stent is normally 2 mm bigger than the fenestration, which is helpful to limit potential kinks or loosening of the bridging stent. Both covered and uncovered stents can be used as the LSA bridging stent in our study. Covered stents would be more suitable to the proximal entry tear adjacent to the origin of the LSA or the PMEGs that are not able to fit tightly to the aortic wall at the level of the LSA, especially aneurysmal dilatation of the aortic arch. Whereas uncovered stents were usually used in patients whose proximal PMEGs has formed a good seal and the risk of leakage is likely to be low, such as aneurysm or tear are located on the side of the minor curvature of the aortic arch or on the opposite side of the fenestration. At this point, the main role of uncovered stent aims to maintain the alignment rather than to ensure PMEG sealing and keep the LSA unobstructed when the fenestration is slightly malpositioned. We believe that the uncovered bridging stent has less impact on the hemodynamics of the aortic arch than the covered bridging stent. In addition, the balloon-expandable stent is a better choice due to its strong support and better alignment with the fenestration through balloon expansion. But unfortunately, we do not have any balloon-expandable covered stents currently available. Therefore, in some patients, we used an uncovered stent inside the covered stent to obtain more support similar to a balloon-expandable covered stent. In the near future, we may have the opportunity to use the balloon-expandable covered stent and evaluate its effect.
The fragility and fabric durability of PMEGs is a crucial concern. Modifications may alter the overall stability of the endograft. 17 Metal fatigue and material deterioration are possible complications of the PMEGs, and the continuing interaction between the fenestration and the LSA bridging stent should be closely observed. No stent fractures or fabric tear has been identified by routine CTA follow-up in our series. Avoiding the damage of the scaffold of the PMEGs and reinforcing the edge of the fenestration play an important role in maintaining the overall stability of the PMEGs. Compared with the in situ laser fenestration, the fenestrations may be more stable over time since they are reinforced. In order to avoid the type I and type III endoleak, the length of the proximal landing zone must be sufficient (≥15 mm), and at least 3 mm of the fabric should be retained from the fenestration to the proximal edge of the PMEGs.
Compared to the high incidence of dSINE reported in other literature,18–20 the 5.9% incidence seems acceptable in our study. Complete avoidance of dSINE is probably impossible because the distal landing zone usually is unhealthy aorta, 21 and the stent-graft size selected based on the proximal landing zone may be relatively too large for the distal landing zone in most patients, especially in aortic dissection with compressed distal true lumen and more fragile intimal membrane. With the remodeling of the aorta (false lumen reduction and true lumen expansion), the mismatch between the distal of the stent-grafts and the distal landing zone will become more obvious and fatal, and the interaction between the two during arterial pulsation may damage the aortic intima. Our lower incidence may have been due to the selection of appropriate oversize and the deployment of additional stent-grafts in high-risk patients to protect or extend the distal landing zone. The additional restrictive bare stent could protect the intima at the distal of the stent graft from excessive radial force. 22 It is also helpful that appropriately extending the length of the covered stent graft to minimize the leverage effect of the lesser curvature on the stent graft, 23 but spinal ischemia or paraplegia will become a more intractable and notable problem. Using a tapered stent-graft may be beneficial for the prognosis of dissection. For those with large changes in the true lumen diameter of the distal and proximal landing zone, we usually selected the tapered stent-graft (taper was 4 or 6 mm). However, in the case of extremely narrow distal true lumen, the lack of a more tapered stent-graft makes its effect equally limited. It is also worth considering how to balance the mismatch of the distal of the stent-graft caused by the gradual expansion of the true lumen during the later aortic remodeling process.
The disadvantages of this technique are the necessity of extensive experience and a long learning curve. The use of PMEGs is still outside the device specification, and different operators may have different modification characteristics, resulting in a lack of industrial quality control for PMEGs and differential clinical outcomes. This type IIIc endoleak in our study was caused by the large fenestration hole, which lead to a large gap at the junction between the fenestration hole and the bridging stent. We sealed this large gap and eliminated endoleak by an unusual embolization approach of using the Amplatzer occluder and spring coils. Although the custom-made thoracic endografts are getting easier to obtain, at least two to three weeks waiting times and high prices are beyond the reach of most patients in China. PMEGs present a valuable compromise in this desperate situation.
There are several limitations in the current study. This study was retrospective in nature. The number of enrolled patients was small and from the same center. In addition, there was heterogeneity in aortic pathology and the brand of PMEGs. Larger samples, longer follow-up, and further subgroup analysis are necessary in the future.
Conclusions
The PMEGs enable extension of the proximal landing to zone 2 and revascularization of LSA during TEVAR. Short-term and mid-term outcomes based on this study seem to be acceptable. This technique is safe and effective for aortic arch pathologies with unhealthy proximal landing zone, and it may be a viable alternative for emergency patients and those who are unable to use custom-made fenestrated or branched device. Durability and stability of the PMEGs will need to be assessed in additional studies with larger sample series and long-term follow-up.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.