
Abstract
Objectives
To report the midterm outcomes of treating prosthetic peripheral and aortic graft infections using a biosynthetic collagen prosthesis in a tertiary vascular center.
Methods
A retrospective analysis of all patients with prosthetic peripheral and aortic graft infections who underwent in situ reconstruction using a biosynthetic collagen prosthesis between March 2015 and November 2020 was conducted. Perioperative and midterm outcomes were analyzed.
Results
A biosynthetic collagen prosthesis was used in 19 patients (14 males, median age 66 years) to reconstruct the femoral artery (n = 6), iliac artery (n = 1), and infrarenal aorta (n = 12). All patients were treated for a prosthetic vascular graft infection. The median follow-up period was 26.6 months (range 1–66 months). The 30-day graft failure rate was 15.7% (n = 3), leading to a major amputation in one patient (5.3%). All grafts were occluded aortofemoral reconstructions in patients with occluded superficial femoral artery and were treated by immediate thrombectomy. The 30-day mortality rate was 5.3% (n = 1), and survival after 3 years was 63.2%. The reinfection rate was 5.3% (n = 1). At 13.6 months, the occlusion of a femoral graft was detected in 5.3% (n = 1) and was treated with a new interposition graft. We observed no graft rupture or degeneration during follow-up.
Conclusions
Although results of in situ repair with autologous vein seem to be superior with little or none reinfection and low number of occlusions, biosynthetic collagen prostheses show acceptable midterm outcomes in terms of graft occlusion and mortality after prosthetic peripheral and aortic graft infections. Similar to other xenogenous materials, the reinfection rate is low with this prosthesis. With regard to immediate availability and easy handling, the use of a biosynthetic collagen prosthesis might be favorable compared to other replacement materials while treating prosthetic graft infections.
Introduction
Despite improvements in surgical techniques and perioperative management, vascular graft infection (VGI) is still relevant in arterial reconstructive surgery. Depending on the anatomic localization of the vascular graft—either extracavitary or intracavitary—VGI frequency varies from 1% to 5% with an infection rate as high as 6% for vascular grafts in the groin. 1 The clinical picture of VGI is diverse, but complications, such as sepsis, septic embolization, and anastomotic rupture with acute bleeding, result in high morbidity and mortality rates.2,3 Besides removing the infected graft and in situ reconstruction of the affected vessel, surgical treatment nowadays consists of the radical debridement of surrounding tissue, the coverage of the reconstruction with biological material (e.g., greater omentum and muscle flaps), and an appropriate antibiotic therapy. 4 Currently, different graft materials are used to replace infected grafts: autologous veins, silver-coated or rifampicin-soaked Dacron grafts, arterial allografts, and xenografts, and each of these materials has their advantages and disadvantages. 5 Furthermore, several authors reported encouraging results using biosynthetic collagen prosthesis for treating VGI in various arterial positions.6–10 This group has previously published a case series in which a biosynthetic collagen prosthesis was used to treat aortic prosthetic graft infection; this case series focused on the feasibility and technical aspects of handling and applying the prosthesis. 11 The aim of this study was to report the midterm results of a biosynthetic collagen prosthesis as a treatment option for VGI and add corresponding follow-up data.
Methods
All patients with prosthetic graft infections undergoing total graft excision and replacement with biosynthetic collagen prosthetic grafts (Omniflow II, LeMaitre, Sulzbach, Germany) between March 2015 and November 2020 were analyzed. Data were generated from a prospectively compiled database. The data collected included clinical symptoms at presentation, comorbidities, procedural details, postoperative complications, and follow-up information. Written informed consent was not obtained because only unidentified data were used. This study was conducted in accordance with the Declaration of Helsinki and was approved by the local ethics committee (approval number 17-858-104).
Diagnosis of VGI
Vascular graft infection diagnoses were made with respect to clinical, laboratory (elevated white blood cell count and increased inflammatory markers [C-reactive protein (CRP) level]), and radiologic means (computed tomography angiography [CT-A]) in combination with intraoperative findings and microbiological culture results. 12 If necessary, an additional 18-F-fluorodeoxyglucose positron emission computed tomography (PET-CT) was performed to confirm diagnosis. Patients with suspected aortoenteric fistulas received endoscopy.
Surgical treatment
Surgical treatment consisted of the complete removal of the infected graft and the radical debridement of surrounding tissue. After the extensive irrigation of the operative field with a hypochlorous acid solution (Granudacyn, Sastomed), an in situ reconstruction with a biosynthetic collagen prosthesis was performed. In all cases, Omniflow II grafts (diameter 8 mm and length 20–40 cm) were used either as a tube graft or as a bifurcated graft as described previously. 11 Patients with infected femoral reconstructions were treated by interposition grafting. 13 Whenever possible, reconstructions were covered by biological material (pedicle omental flap and sartorius muscle flap). In patients with a groin infection, negative wound pressure therapy was applied for 4–10 days; femoral wounds were closed secondarily or were covered by a split skin graft. In the case of an aortoenteric fistula, a bowel reconstruction with a tubular defect resection and side-to-side enteroanastomoses was performed. Patients with prostheto-ureteral fistulas had their ureter resected using an end-to-end anastomosis over an ureteral splint.
Antimicrobial therapy
With suspected diagnoses, serial blood culture samples were taken at admission. Calculated intravenous antibiotic treatment was started intraoperatively after the collection of the specimens of the infected graft and surrounding tissue. The antibiotic therapy was modified according to microbiologic findings, resistance screening, and the consultation of a microbiologic specialist. Generally, the duration of antibiotic therapy was limited to a maximum of 6 weeks following a recent review by Antonello et al., who recommends a duration of antibiotic therapy for 4–6 weeks for methicillin-sensitive Staphylococcus aureus (MSSA) or methicillin-resistant Staphylococcus aureus (MRSA) and 2 weeks for other species, for all graft materials (autologous vein, silver-coated grafts, rifampicin-soaked Dacron grafts, and xenogenous materials). 5
Follow-up
Before discharge, a clinical assessment and laboratory tests for white blood cell count and CRP levels were performed. All patients received antiplatelet therapy with acetylsalicylic acid (100 mg/day). They were seen in an outpatient clinic every 3–6 months with clinical, laboratory, and duplex ultrasound evaluations and were assessed for signs of reinfection and graft patency.
Statistical analysis
The primary endpoint of the study was freedom of reinfection. Thirty-day mortality and morbidity, graft occlusion rate, major amputation rate, and survival were secondary endpoints. Thirty-day mortality was defined as death ≤30 days postoperatively, and 30-day morbidity included postoperative complications within 30 days after surgery. Postoperative complications included surgical, medical, graft-related, and gastrointestinal complications. Late mortality was defined as death ≥30 days postoperatively. All categorical variables are presented as absolute and relative frequencies, while age is shown as mean (standard deviation (SD)). Freedom from reinfection, graft occlusion rate, major amputation rate, and survival were calculated by the Kaplan–Meier method. Statistical analysis was performed using SPSS version 26.0 (IBM, Armonk, NY, USA).
Results
Patient characteristics
Between 2015 and 2020, a total of 19 patients (14 males, median age 66.6 years) with VGI were treated with a biosynthetic collagen prosthesis. Some data from eight of these patients were published before. 11 Follow-up data for all surviving patients were available until November 2020. No patients were lost to follow-up. The median follow-up period was 26.6 months (range 1–66 months).
Patient characteristics and presentations.
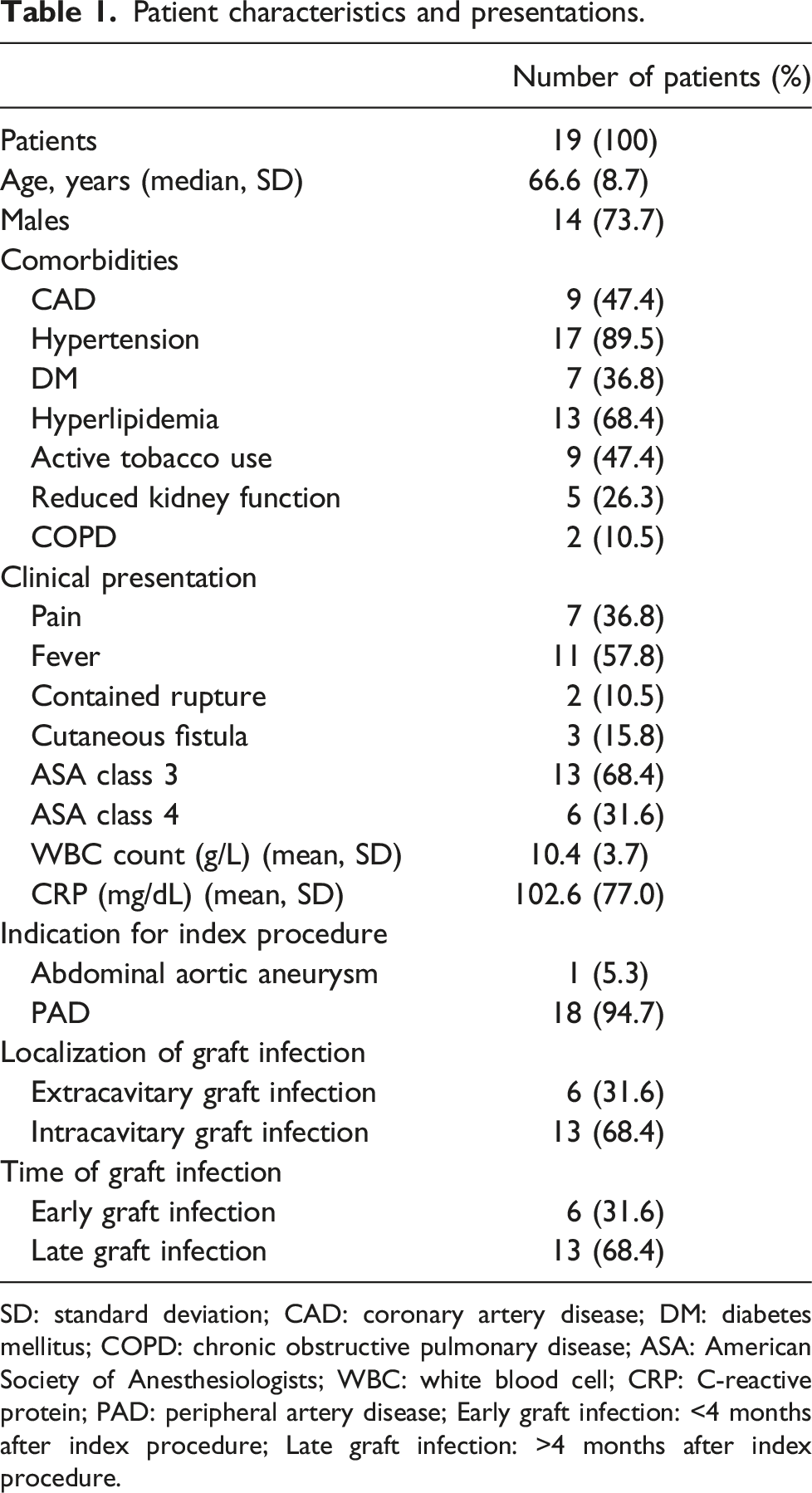
SD: standard deviation; CAD: coronary artery disease; DM: diabetes mellitus; COPD: chronic obstructive pulmonary disease; ASA: American Society of Anesthesiologists; WBC: white blood cell; CRP: C-reactive protein; PAD: peripheral artery disease; Early graft infection: <4 months after index procedure; Late graft infection: >4 months after index procedure.
Management
Clinical and diagnostic findings.
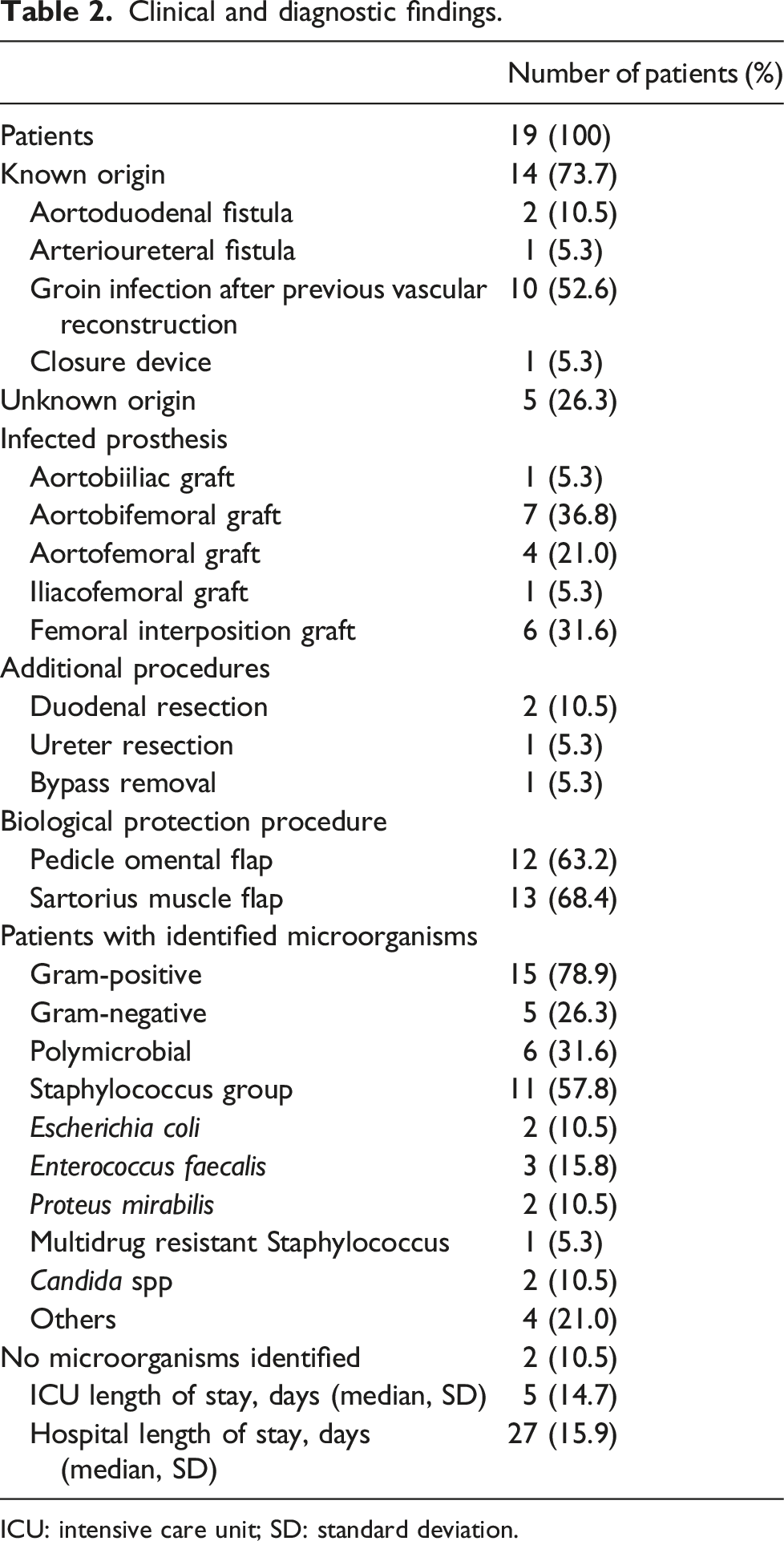
ICU: intensive care unit; SD: standard deviation.
Culture samples of intraoperative specimens were positive in 17 patients (89.5%). Among these, 11 specimens were monomicrobial (64.7%), and six specimens were polymicrobial (35.3%). Gram-positive microorganisms were most commonly isolated, followed by Gram-negative microorganisms and Candida subspecies. There were two patients (10.5%) where no causative microorganisms were detected.
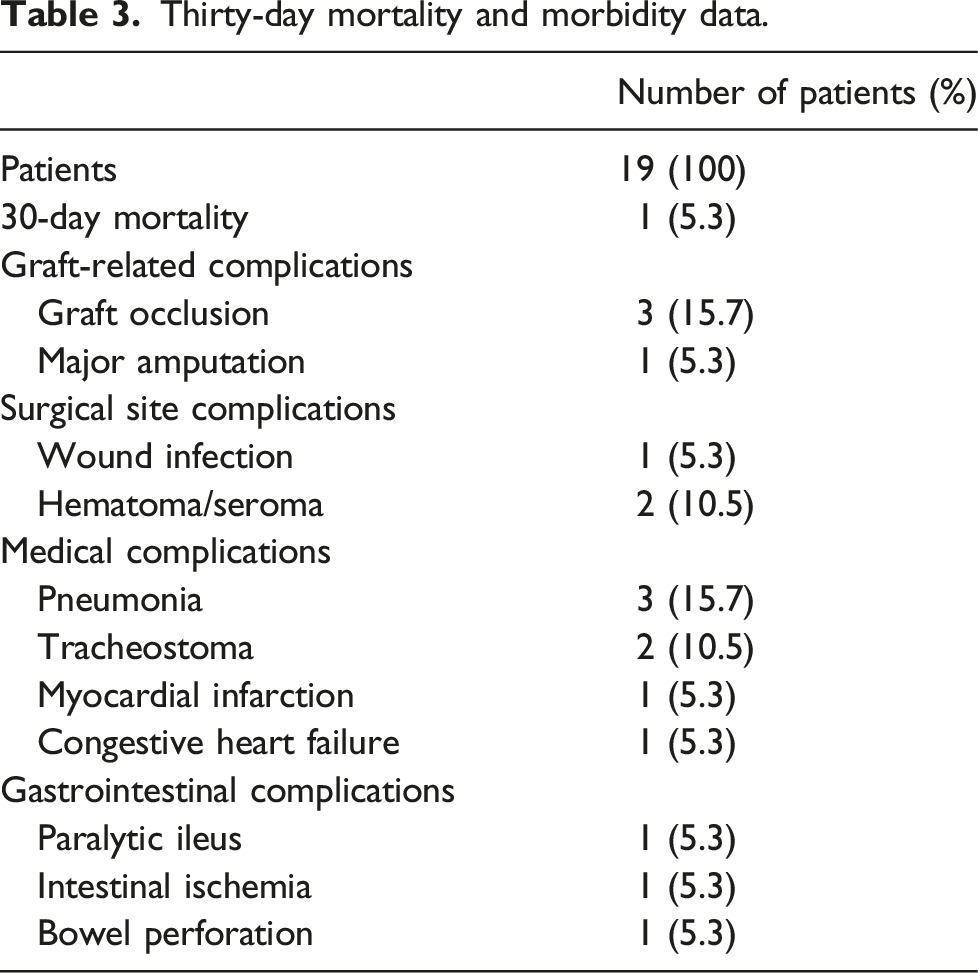
Thirty-day results
Thirty-day mortality and morbidity data.
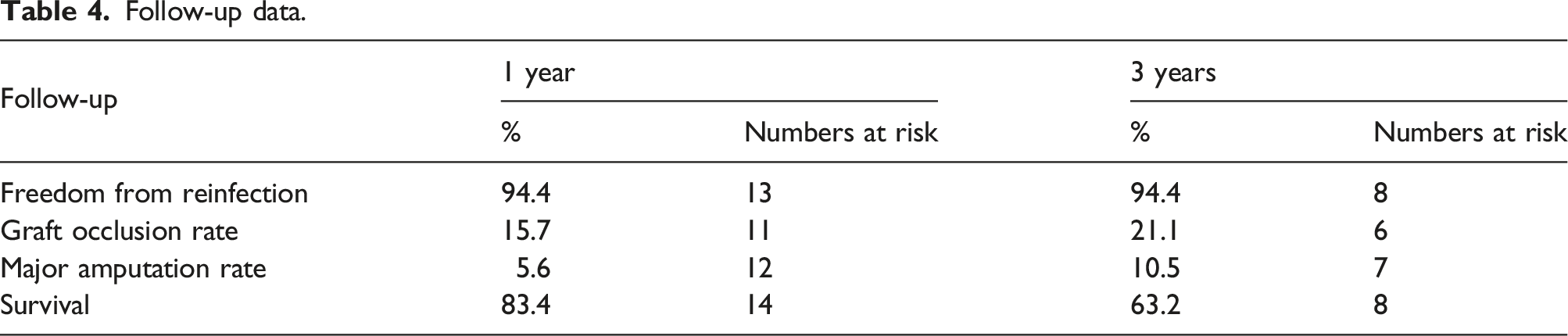
Midterm results
Follow-up data.
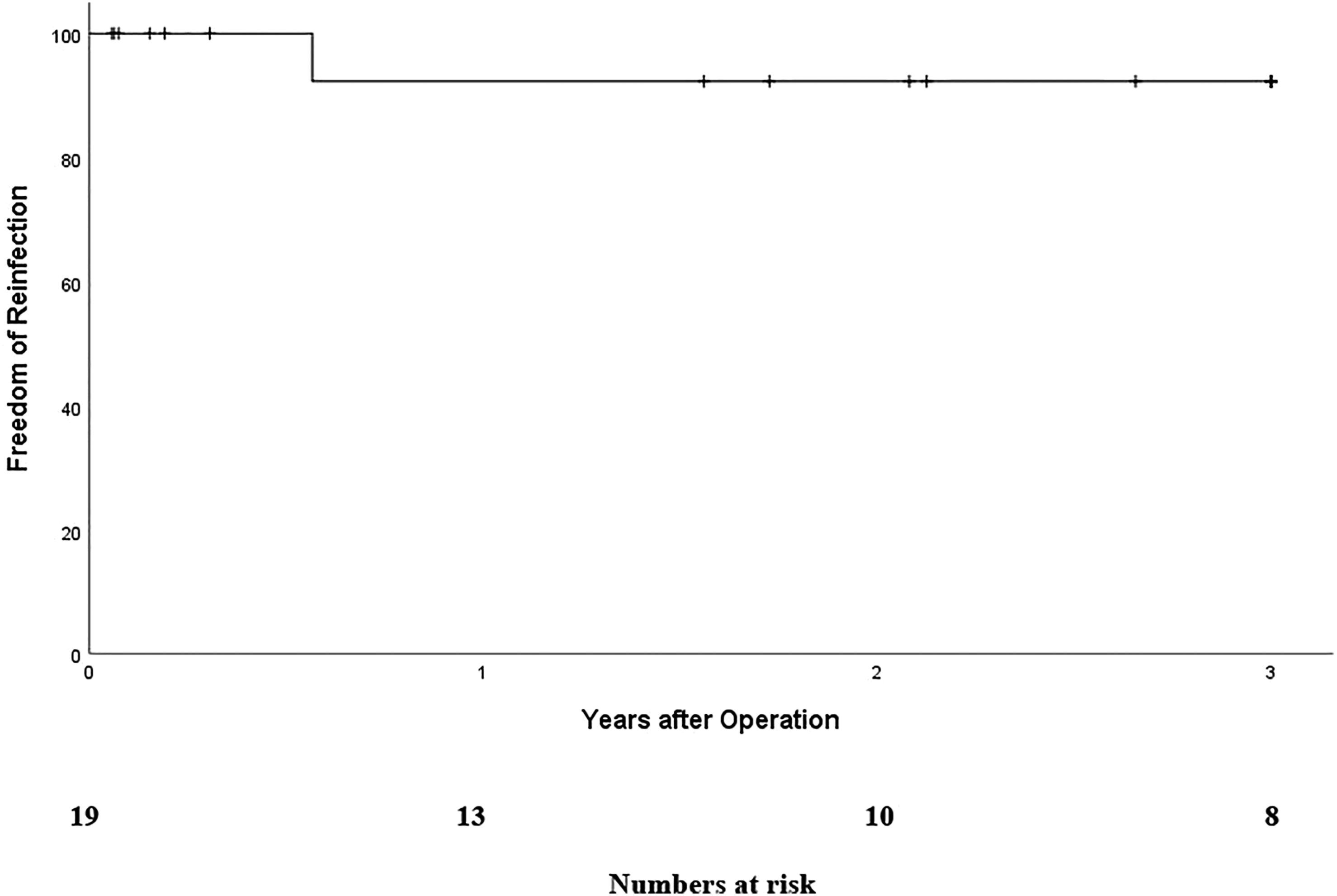
Freedom from reinfection.
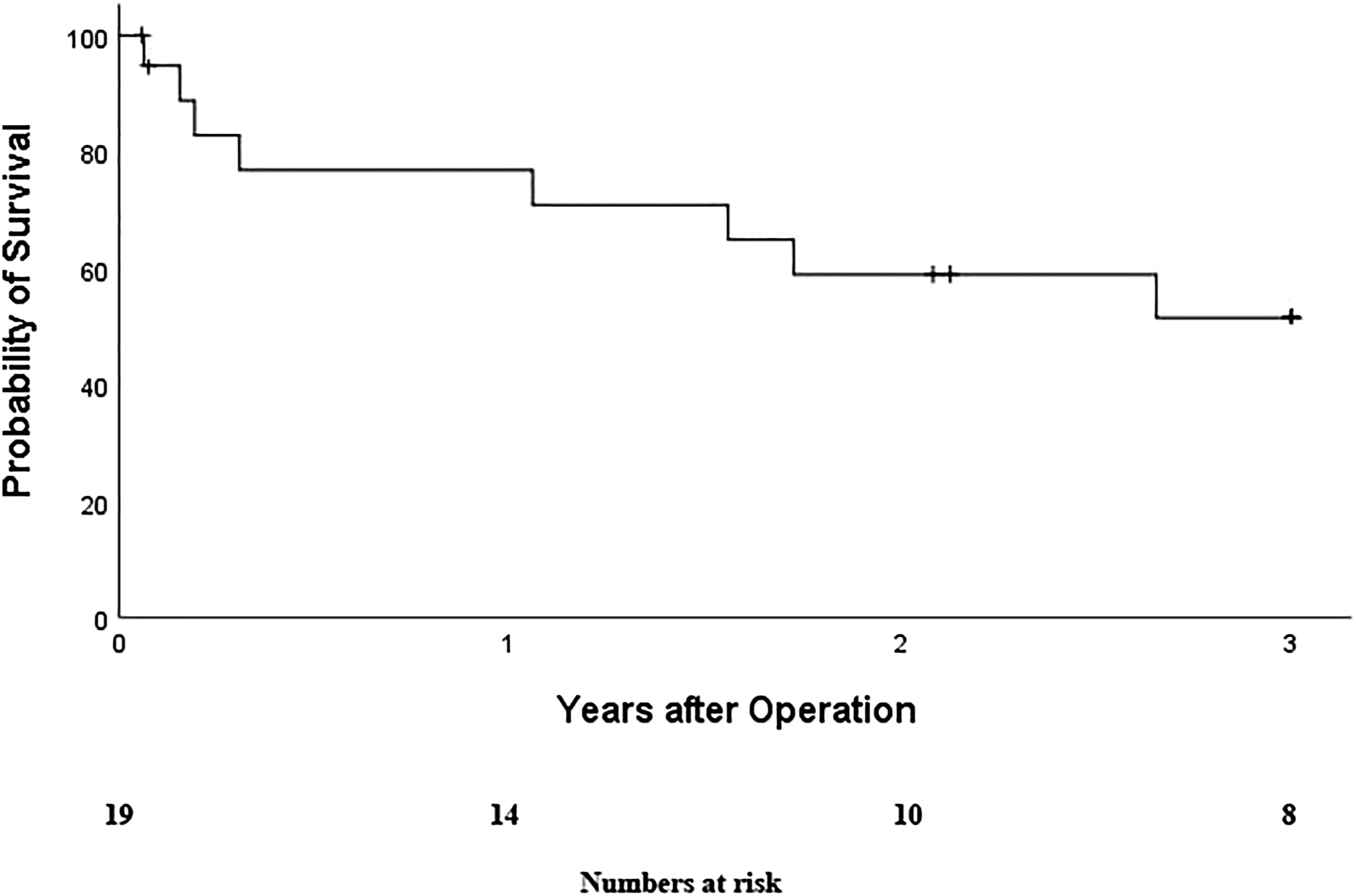
Probability of survival.
Discussion
The aim of this study was to evaluate the midterm results of biosynthetic collagen prostheses used for arterial reconstruction in patients with a prosthetic graft infection. Our reinfection rate was considerably low. We observed no graft rupture or graft degeneration during follow-up. Follow-up imaging showed no signs of restenosis. Nonetheless, results related to the graft occlusion rate were not as favorable as expected.
Today, several graft materials are used for VGI management, and each of these materials has variable outcomes, advantages, and disadvantages. Compared to synthetic-coated grafts with reinfection rates of up to 18%, biological conduits, autologous veins, and cryopreserved allografts achieve much lower reinfection rates. 4 However, the autologous vein is not always suitable as graft material, and vein harvesting might be also associated with deeper surgical trauma and lengthier operative times. 5 Furthermore, cryopreserved allografts are not available in emergency settings and allograft-related reintervention rates were found up to 55% during long-term follow-ups, including reinterventions due to allograft degradation leading to aneurysms, dilatations, and graft ruptures. 4
Besides that, different groups report encouraging results using xenogenous grafts for VGI treatment. 4 A recent review by Hostaldrich et al. analyzed four studies with 71 patients treated with aortic grafts and native aortic infections with xenopericardial grafts. Authors reported a reinfection rate of 6% during a mean follow-up of 28 months. The early reintervention rate was 1.4%, and the late reintervention rate was 7.5%. Due to false aneurysms or xenograft ruptures, two patients had to be treated by open repair and three by thoracic endovascular aortic repair. 14 Another study by Kreibich et al. observed no reinfections during a mean follow-up of 18 months in a series of 20 patients. Three patients required aortic intervention for false aneurysms, graft occlusion, and the development of a neoaortointestinal fistulation. 15 Low reinfection rates were also reported in a case series by Krazsnai et al. 8 and De Siqueira et al. 9 who used a biosynthetic collagen prosthesis to treat VGI in aortoiliac and femoral positions. In our cohort, the reinfection rate was 5.6% at a mean follow-up time of 26.6 months. We observed no graft ruptures or false aneurysms during follow-up. One patient developed a fistulation between the right ureter and the Omniflow tube graft and had to be treated by open repair.
Nonetheless, autologous vein reconstructions for abdominal aortic VGIs are the most effective means of avoiding reinfection.2,4 A recent study by Ali et al. analyzed the outcome of 165 patients with aortic graft infection treated by in situ reconstruction with the femoral vein. The reinfection rate reported after 32 months of follow-up was 5%. 16 In another study by Dorweiler et al., 17 no reinfections were reported after 60 months of follow-up. In that study, 67 patients with infection of the aortoiliac axis received vascular reconstruction using the femoral vein. 17
Our findings concerning graft occlusion, major amputation, and 30-day mortality differed from these studies. We observed a high rate of aortic graft occlusions with the first 30 postoperative days. However, most of our patients received index procedures for the treatment of peripheral artery disease (PAD) and not for aneurysmatic disease, which is necessary to distinguish. All patients with occluded aortic grafts had a PAD and an impaired outflow with an occluded superficial femoral artery. All these patients had severe sepsis due to aortic graft infection, which causes intravascular activation of coagulation. 18 This in combination with an impaired outflow could explain the high early occlusion rate of the Omniflow II grafts. After revision surgery, we performed an additional anticoagulation with PTT-controlled heparinization along with antiplatelet therapy, so no further occlusions were observed in these groups of patients within the first 30 perioperative days.
In our experience, it is sometimes possible to explant the infected prosthetic graft with no further vascular reconstruction. In this series, we removed an occluded infected lower extremity graft and performed a femoro-profundal interposition graft without bypass replacement in a patient with claudication.
Our graft occlusion rate after 3 years was 21.1%. In the studies by Ali et al. 16 and Dorweiler et al., 17 reconstructions with the femoral vein performed better with occlusion rates of 0% and 3%, respectively. Similar results in terms of occlusion rates (0–8%) were reported from other authors using silver-coated grafts. 4 However, reinfection rates with silver-coated grafts are up to 16%. 4 Our midterm occlusion rates are comparable to rifampicin-bonded grafts and to cryopreserved allografts. Hayes et al. and Young et al. reported occlusion rates of 18.2% and 14% after 12 and 36 months of follow-up using rifampicin-bonded grafts, respectively.19,20 Kieffer et al. analyzed the outcome of 68 patients with aortic graft infection and cryopreserved allografts. After 34 months of follow-up, 29.7% of reconstructions were occluded. 21 Another study by Nevelsteen et al. reported an occlusion rate of 23% in 30 patients with cryopreserved allografts and intra- and extracavitary graft infections after 25 months of follow-up. 22
In our study, VGI also occurred in different arterial positions; extra and intracavitary graft infections were included. All intracavitary VGIs were limited to the abdominal aorta or iliac vessels compared to other series, where all aortic segments, including the aortic arch and the thoracoabdominal aorta were treated. 14 This limitation with localization of VGIs on infrarenal aortic segments and the groin could explain our low 30-day mortality of 5.3%. A recent study by Almasi-Sperling et al. analyzed the outcome of 19 consecutive patients with VGI in different arterial positions and in situ repair with bovine pericardium. In 47% of patients, VGI was localized in the femoral artery. During short-term follow-ups of 6 months, the graft occlusion rate reported was 11% and the major amputation rate was 5.3%. 23 In our study, the 1-year graft occlusion rate was 15.7%, and the major amputation rate was 5.6%. Survival at 3 years was 61.2%, which is comparable to that reported in other series. 14 Nonetheless, experience with the use of biosynthetic collagen prosthesis to treat prosthetic aortic graft infection is still limited, and only case series with small numbers of patients have been reported until now.8,9,24 However, the reinfection rates with this prosthesis in these studies are low. The study with the greatest number of patients was published in 2021 by El Beyrouti et al., who reported the outcome of 16 patients with aortic graft infection treated with biosynthetic grafts. After a mean follow- up of 28.6 months, the reinfection rate was 6.3%. 24
This study has several limitations. The main limitation is the small number of patients and the retrospective design. The study population was heterogeneous since patients with extracavitary and intracavitary VGIs were included. We did not include patients with VGI who received other graft materials. Follow-up was performed with clinical examinations, laboratory values, and duplex ultrasound. Hence, no additional imaging studies, such as PET-CT, were performed.
This is the largest case series reporting the treatment of VGI using Omniflow II grafts. The use of a biosynthetic collagen prosthesis for treating VGI was feasible and associated with low reinfection rates. Graft occlusion and major amputation rates were acceptable compared to other graft materials. Although results of in situ repair with autologous vein seem to be superior with few or no reinfection and low number of occlusions, biosynthetic grafts may be a valuable alternative to traditional graft materials due to the low reinfection rate, their ease of handling, and their immediate availability.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.