
Abstract
Background/Objective
To evaluate the safety and utility of a new in Europe intravascular ultrasound (IVUS) catheter in a case of peripheral arterial disease caused by in-stent restenosis of the superficial femoral artery.
Method
Pre-therapeutic computed tomographic angiography identified severe stent restenosis related to device underexpansion, which was caused by an underlying eccentric severely calcified stenosis leading to suboptimal device deployment. The OptiCross 18 (30 MHz Peripheral Imaging Catheter, Boston Scientific, USA) is a short rail imaging catheter. It consists of two main assemblies: The imaging core is composed of a hi-torque, flexible, rotating drive cable with a radial looking 30 MHz ultrasonic transducer at the distal tip. An electro-mechanical connector interface at the proximal end of the catheter makes the connection to the Motordrive Unit (MDU5 PLUSTM) Instrument. The MDU5 PLUS-catheter interface consists of an integrated mechanical drive socket and electrical connection.
Results
The use of the IVUS-guided imaging revealed in-stent restenosis, fracture, and protrusion of the calcified plaque in the stent and confirmed the preoperative computed tomography angiography which showed stent compression. Use of intravascular litotripsy catheter (intravascular lithotripsy Shockwave Medical, Santa Clara, California) and drug coated balloon led to improvement in stent expansion, having minimal patent diameter of 5.77 mm. The patient’s subsequent clinical course was uneventful, and clinically had palpable pulses in the foot and ankle-brachial index of 1.
Conclusions
Whether acoustic pulse application might affect device structure in the long term remains to be determined, use of the novel IVUS system demonstrated excellent visibility of the etiology of the in-stent restenosis improving the perioperative diagnostic modalities of suboptimal endovascular outcome.
Calcification remains the Achilles heel of the endovascular treatment of peripheral arterial disease.1,2 The heterogenous plaque morphology can not only influence the patency of the treated segments but can also provoke severe stenosis of deployed nitinol stents with protrusion in the lumen of the stent and also stent fractures.3,4
A 74-year-old man with history of peripheral artery disease (PAD) and stent implantation in the superficial femoral artery 14 months previously was referred to our center for recurrent claudication.
The preoperative computed tomographic angiography (CTA) identified severe in-stent restenosis related to device underexpansion, which was caused by an underlying eccentric severely calcified plaque leading to suboptimal stent expansion (Figure 1(a)). The use of intravascular ultrasound (IVUS)–guided imaging revealed in-stent restenosis (Figure 1(b)), stent fracture (Figures 1(c) and (d)), and protrusion of the calcified plaque in the stent (Figure 1(e)) confirming the preoperative CTA findings. OptiCross 18 IVUS catheter was employed (30 MHz Peripheral Imaging Catheter, Boston Scientific, USA) is a short rail imaging catheter. It consists of two main assemblies: The imaging core is composed of a hi-torque, flexible, rotating drive cable with a radial looking 30 MHz ultrasonic transducer at the distal tip. An electro-mechanical connector interface at the proximal end of the catheter makes the connection to the Motordrive Unit (MDU5 PLUSTM) Instrument. The MDU5 PLUS-catheter interface consists of an integrated mechanical drive socket and electrical connection. Intravascular ultrasound–guided imaging confirming computed tomography angiography with the stent-related complications (1a-e) and also the final result after treatment 1f.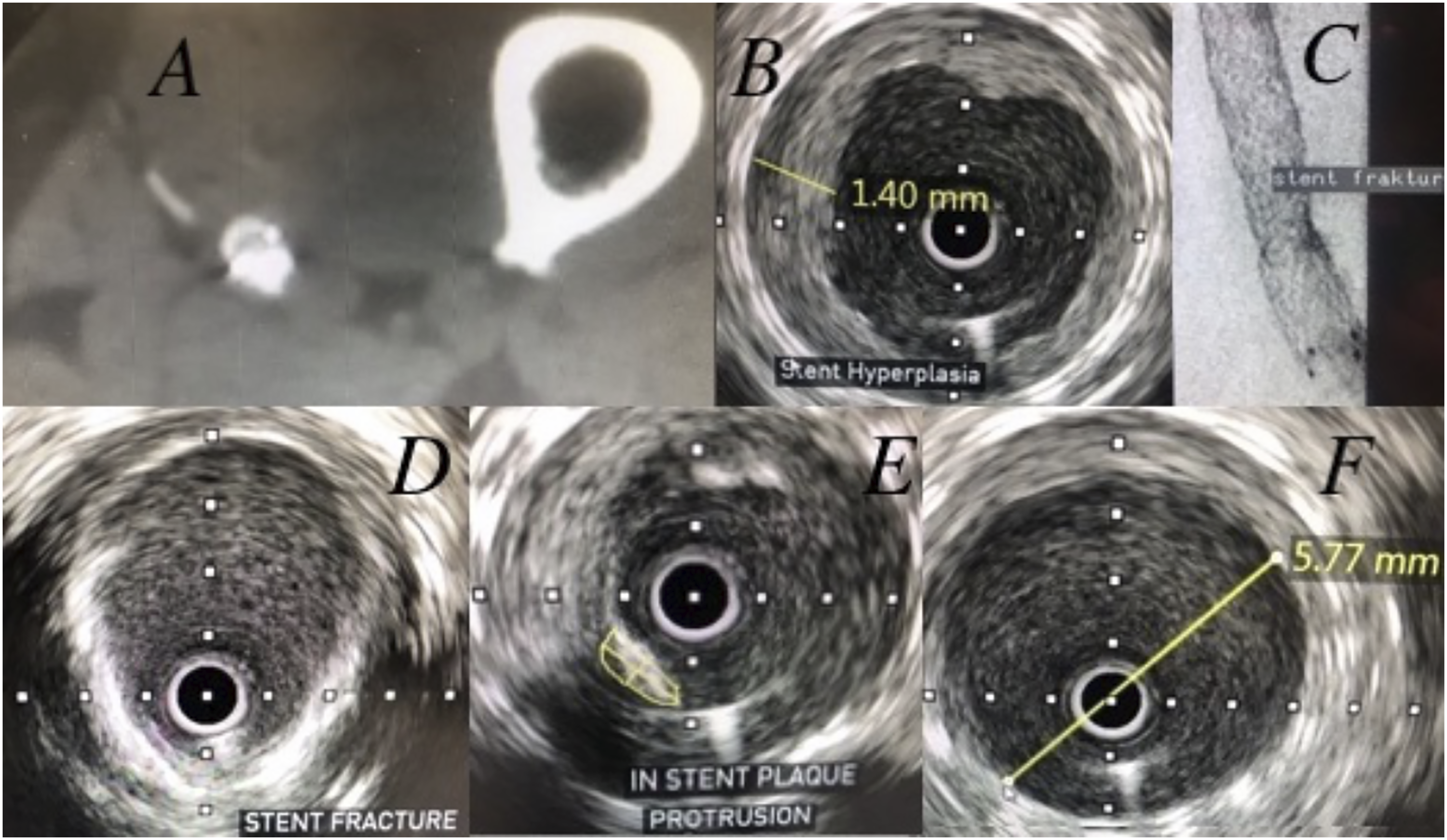
To disrupt the calcified lesion and ensure correct stent expansion, in-stent intravascular lithotripsy (IVL) was performed. The procedure was performed through transfemoral contralateral access and led to the delivery of 270 sonic pulses using a 6 × 60 mm IVL catheter (Shockwave Medical, Santa Clara, California). The procedure was finalized using 6 × 80 mm drug coated balloon (DCB) angioplasty. The use of IVL and drug coated balloon improved stent expansion enlarging the minimal patent diameter of 5.77 mm (previous 4.76, Figure 1(f)). The patient’s subsequent clinical course was uneventful, recovering ankle-brachial index of 1 (previous 0.68).
Vascular calcifications are associated with worse clinical prognosis in patients with PAD. 1 The here reported case is the first experience in Europe of the use of the OptiCross 18 IVUS-guided IVL therapy for successful treatment of underexpanded stent in the superficial femoral artery. It seems like the cited catheter for IVUS-guided imaging and later IVL and DCB therapies are safe and feasible diminishing the risk for peripheral embolization while avoiding the deploying of additional stents in the already stenosed device which may narrow further the patent lumen.5,6 Whether acoustic pulse application might affect device structure in the long term remains to be determined.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.