
Abstract
Objective
Practice patterns and durability of parallel stent graft techniques in complex endovascular aneurysm repair (EVAR) remain poorly defined. We aimed to quantify and compare the impact of renal chimney intra-aortic stent length (IASL) on geometric deformations of renal arteries in complex EVAR.
Methods
Thirty-eight nonconsecutive patients underwent EVAR utilizing parallel stent graft techniques (chimney EVAR [chEVAR], n = 28; chimney endovascular aneurysm sealing [chEVAS], n = 10) between 2010 and 2016. A total of 59 renal chimney stent grafts were used. Geometric quantification was derived from three-dimensional model-based centerline extraction. Renal chimney intra-aortic stent length (IASL) was defined as the length of chimney stent that extended from the proximal edge of the chimney stent to the ostium of the corresponding renal artery.
Results
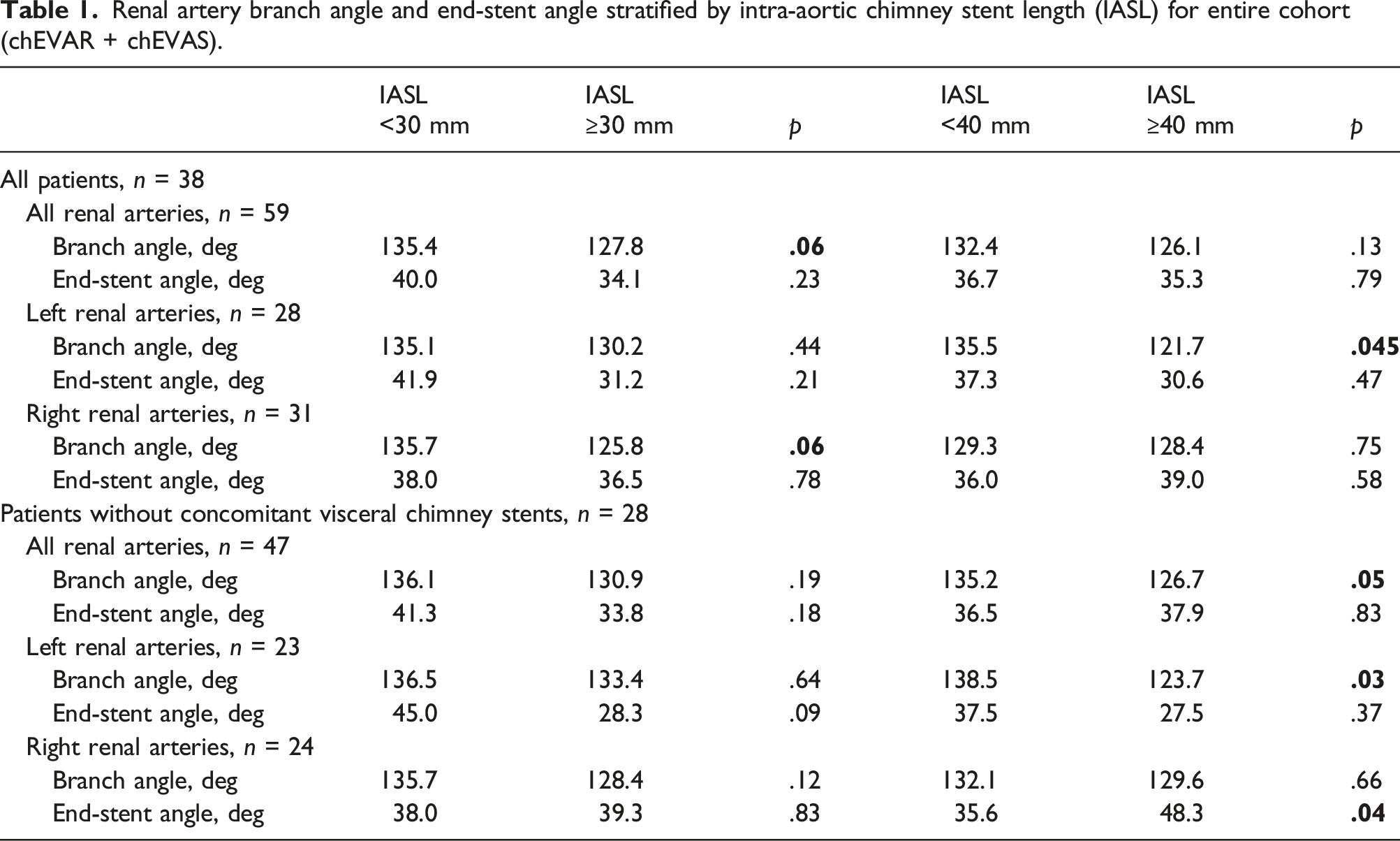
Mean IASL for both left and right renal arteries in the cohort was 35.7 mm. Renal arteries containing chimney IASL <30 mm trended toward a greater branch angle (135.4 vs. 127.8°, p = .06). Left renal arteries showed significantly greater branch angle among those with IASL <40 mm (135.5 vs. 121.7°, p = .045). Mean IASL for renal arteries in chEVAR was significantly longer compared to chEVAS (39.2 vs. 26.3 mm, p = .003). No difference was noted in overall branch angle or end-stent angle based on procedure type. ChEVAR with IASL <30 mm had significantly greater end-stent angle (48.2 vs. 33.5°, p = .03). In contrast, chEVAS patients showed no difference in end-stent angle based on IASL thresholds, but did have significantly greater branch angle among those with IASL <30 mm when grouped by both all renal arteries (133.5 vs. 113.5°, p = .004) and right renal arteries (134.3 vs. 111.6°, p = .02).
Conclusions
Renal chimney stents with longer IASL appear to exhibit less renal artery deformation, suggesting a more gradual and perpendicular transition of the chimney stent across the renal ostium.
Introduction
While endovascular aneurysm repair (EVAR) is widely recognized as the gold standard treatment modality of abdominal aortic aneurysm disease, nearly 30% of these patients are not anatomically suitable for conventional EVAR due to hostile features of the proximal aneurysm neck. 1 Fenestrated and branched stent graft technology serves as the basis for more complex EVAR among patients with juxtarenal, pararenal, and thoracoabdominal aortic pathology. However, there are limitations to these more sophisticated forms of complex EVAR, including inability to use these devices in non-elective settings as a result of manufacturing delays, renovisceral anatomy that falls outside acceptable engineering constraints, and iliofemoral tortuosity or occlusive disease.
Parallel stent graft techniques utilizing one or more chimney stents placed antegrade into the renal and/or visceral arteries in combination with either a conventional EVAR device (chimney EVAR [chEVAR]) or endovascular aneurysm sealing system (chEVAS) both serve as alternative forms of complex EVAR with fewer relative limitations. Despite well-established technical success and early outcomes,2–6 longer-term durability of parallel stent graft techniques—particularly as it relates to device–tissue interactions—remains poorly defined. Previous work has explored this topic as it relates to cardiac pulsatility-, respiratory-, and EVAR-induced deformations of the renal arteries associated with complex EVAR.7–12
While fenestrated EVAR serves as the only currently available FDA-approved endovascular treatment option for complex AAAs, the utilization and clinical practice of complex EVAR with parallel stent graft techniques lack similar standardization. The length of chimney stent grafts in these other complex EVAR configurations, for instance, remains one of the most variable aspects of the procedure. As such, the present study expands on our previous work by characterizing the impact of renal chimney intra-aortic stent length (IASL) on geometric deformations of the renal arteries and associated renal chimney stents in complex EVAR.
Materials and Methods
Study cohort
The present study features a non-randomized subset of our overall series of complex EVAR patients who were prospectively recruited between March 2010 and December 2016. Written informed consent was signed by all patients under a complex EVAR protocol approved by our local Institutional Review Board. Notably, all patients were deemed not candidates for open surgical repair based on poor physiologic fitness and were also unsuitable for conventional EVAR due to one or more hostile infrarenal neck anatomic variables. Planning and execution of final endovascular strategy utilizing chimney techniques with or without concomitant fenestrated technology was based on anatomic considerations, acuity of presentation, as well as endograft availability. Patients with aortic anatomy necessitating complex EVAR with planned stenting of at least one renal artery and with adequate serial contrast-enhanced postoperative CTA imaging were included for analysis.
ChEVAR procedures utilized commercially available bifurcated aortoiliac stent grafts in combination with one or more parallel chimney stents. Renal arteries were stented using either balloon-expandable (iCAST, Atrium Maquet Getinge Group, Hudson, NH, USA) or self-expanding (Viabahn, W.L. Gore, Flagstaff, AZ, USA) covered stents. Balloon-expandable bare metal stents (Omnilink Elite, Abbott Vascular, Santa Clara, CA, USA) were routinely used to augment the radial force of Viabahn stents in the area of overlap between the main body endograft and the parallel graft. Secondary bare metal stents in chEVAR cases did not extend any distance into the target renal arteries. In contrast, chEVAS procedures utilized both the Nellix EndoVascular Aneurysm Sealing system (Endologix, Irvine, CA, USA) and one or more balloon-expandable renal artery chimney stents (iCAST; Atrium Maquet Getinge Group). No accessory maneuvers or devices (e.g., reinforcing or transition bare stents) were used in chEVAS procedures. Patients with a history of connective tissue disorder, lack of contrast-enhanced cross-sectional imaging, or those undergoing either periscope (parallel stent-graft configuration oriented in an inferior to superior direction) or sandwich techniques were excluded.
Geometric quantification
Details regarding CTA image acquisition and processing methods have been described in the previous studies.7,9,12 Using dedicated modeling software (SimVascular; Open Source Medical Software Corporation, San Diego, CA, USA), initial postoperative CTA images were utilized to generate three-dimensional geometric models of the abdominal aorta with branch vessels, branch vessel stents, and aortic endografts (Figure 1). Imaging was acquired at inspiratory breath-hold. Mathematical centerlines of the abdominal aorta, renal arteries, and renal stents were extracted in order to facilitate the following renal artery (chimney) geometric calculations (Figure 2): CT-based computational modeling steps to extract geometry of the abdominal aorta, vessels, stents, and endograft from chimney EVAR (top row) and chimney EVAS (bottom row) patients. Quantification of intra-aortic stent length (IASL), renal branch angle, and end-stent angle, based on geometry of the abdominal aorta with renal arteries (gray) and chimney stents (red).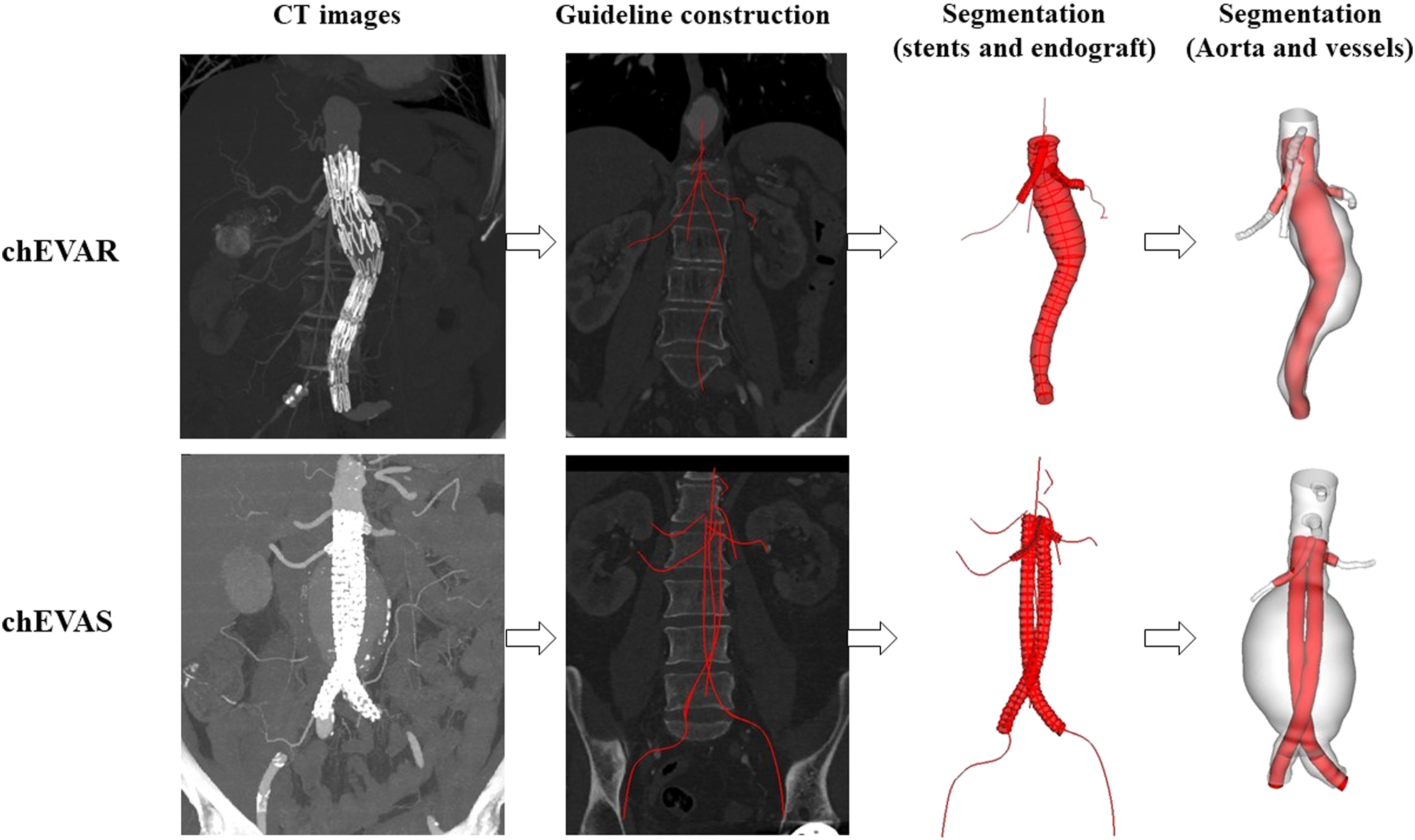
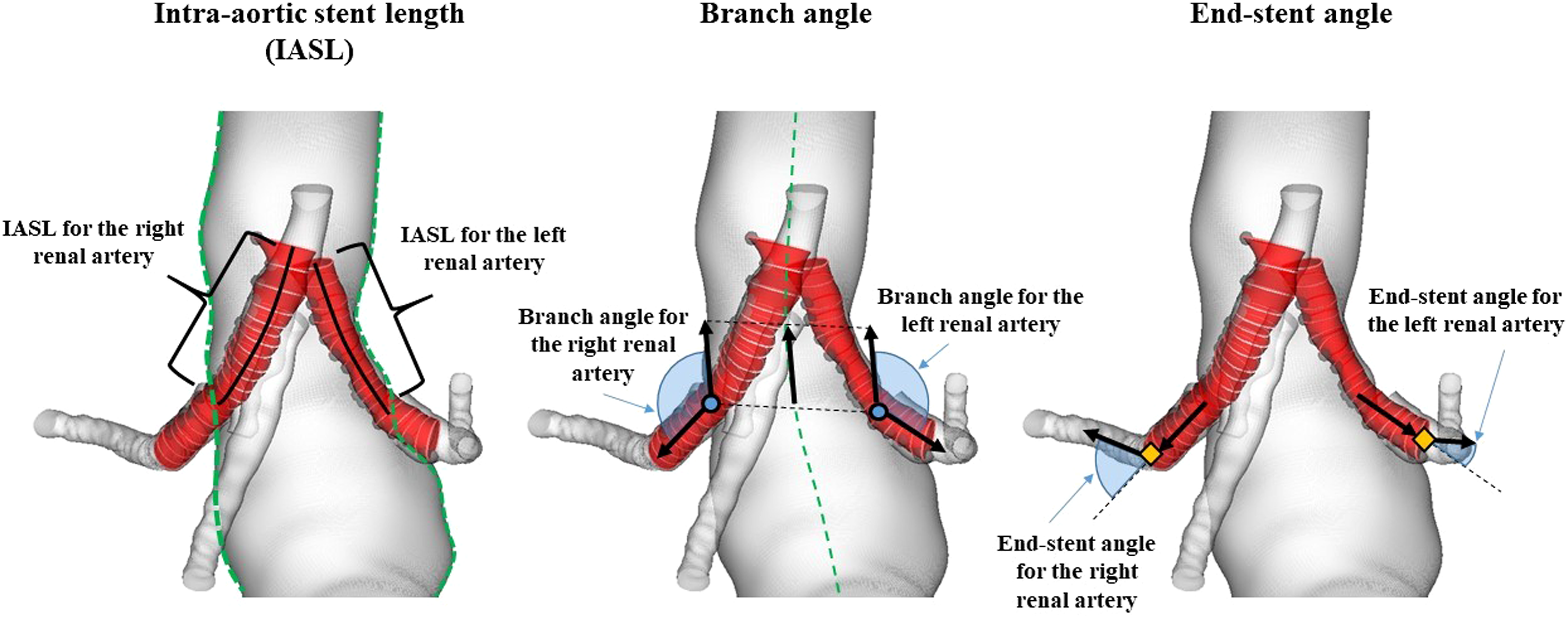
Intra-aortic stent length (IASL)
Defined as the length of renal artery chimney stent that extends from the proximal edge of the chimney stent to the ostium of the corresponding renal artery. Clinically relevant IASL thresholds of 30 mm and 40 mm were selected to perform subgroup analysis, and seek for statistical correlation to branch angle and end-stent angle.
Branch angle
Defined as the angle of renal artery centerline with respect to the centerline of the aorta at the renal ostia. A 90° branch angle indicates perpendicular branching. Obtuse branch angle indicates downward-directed branching, whereas acute branch angle indicates upward-directed branching.
End-stent angle
Defined as the angle between the vectors of the distal end of the renal stent and the native renal artery distal to the stent end, each defined by a 10 mm arclength along the renal centerline. Zero-degree end-stent angle indicates straight configuration from the distal stent to the native artery.
Clinical outcomes
Perioperative outcomes and both clinical and radiologic follow-up data were prospectively recorded for enrolled patients. Early mortality included deaths occurring during the index hospitalization or within 30 days of procedure. Renal artery patency was defined as absence of branch vessel stenosis (peak systolic velocity ratio >2.0) or occlusion requiring reintervention during the follow-up period. Reintervention was defined as a repeat procedure for complications that were aneurysm- or endograft-related or a result of the initial procedure. Target (chimney) vessel events included renal artery stenosis or occlusion, need for any branch vessel–related reintervention, or aneurysm sac growth resulting from branch-related type III endoleak.
Statistical analysis
Data were reported as mean ± standard deviation. Two-tailed paired t-tests were employed for comparisons between different time points, whereas two-tailed unpaired t-tests were used for comparisons between left and right renal arteries. The significance threshold was set at p < .05.
Results
A total of 38 patients met inclusion criteria and were analyzed, including 28 undergoing chEVAR (21 using conventional aortoiliac stent grafts and seven in combination with a customized fenestrated bifurcated aortoiliac stent graft [ZFEN, Cook Medical, Bloomington, IN, USA]) and 10 patients undergoing chEVAS. Among those patients undergoing repair using combined fenestrated and parallel stent graft technology, only the renal chimney stent(s) were examined in this study (renal arteries targeted with fenestration were not included for analysis). Device manufacturers utilized in the patients undergoing chEVAR with commercially available stent grafts included 15 Zenith or Renu (Cook Medical), three Endurant (Medtronic Inc, Minneapolis, MN, USA), one Anuerx (Medtronic Inc), one Ovation (Endologix, Irvine, CA, USA), and one Excluder (Gore Medical, Flagstaff, AZ, USA). Chimney stents included 31 right renal arteries and 28 left renal arteries. Twelve patients required concomitant visceral artery chimney stents (SMA chimney, n = 10; SMA + celiac chimney, n = 2). In total, chimney configurations were single in 12 patients, double in 22 patients, triple in 3 patients, and quadruple in 1 patient.
Comparative geometric data
Renal artery chimney stents, stratified by IASL
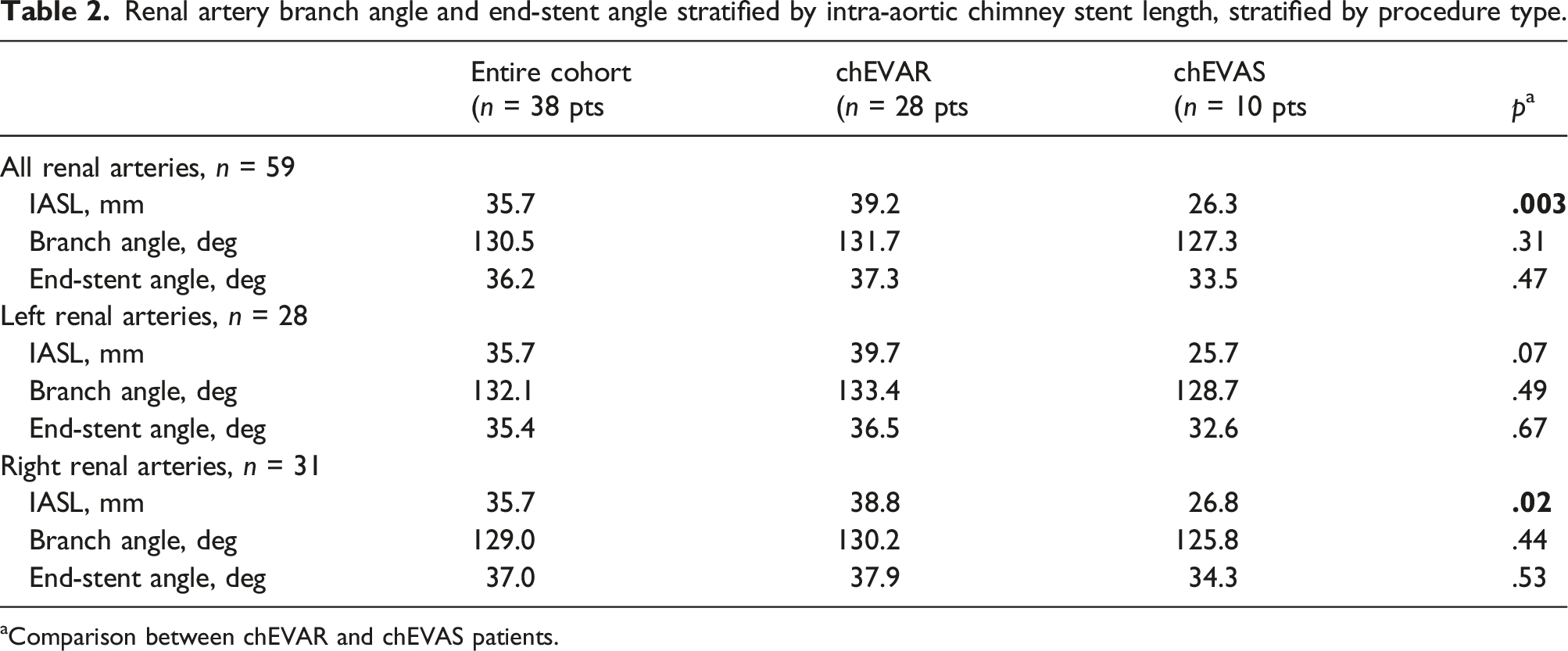
Renal artery branch angle and end-stent angle stratified by intra-aortic chimney stent length (IASL) for entire cohort (chEVAR + chEVAS).
ChEVAS versus ChEVAR
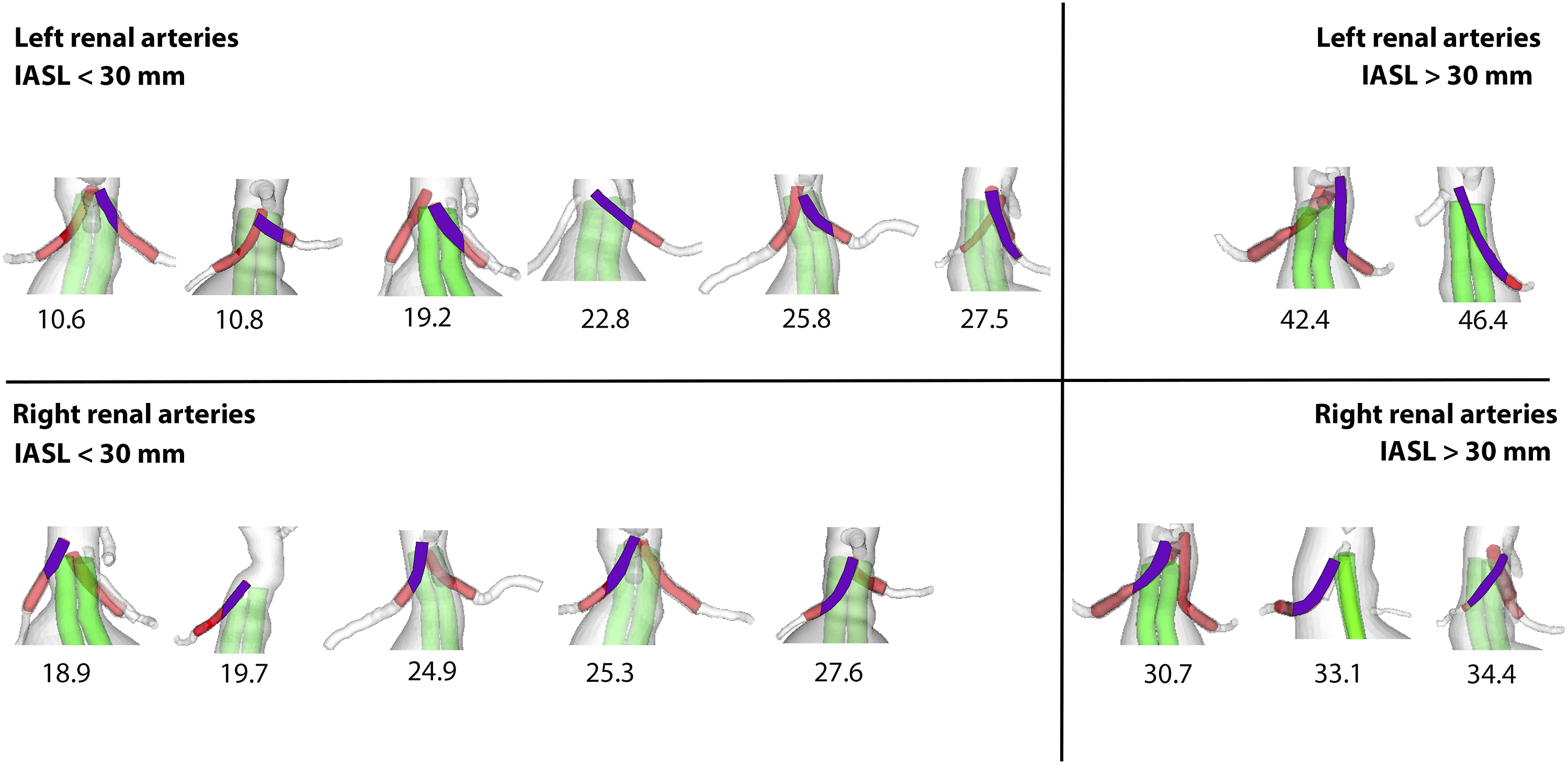
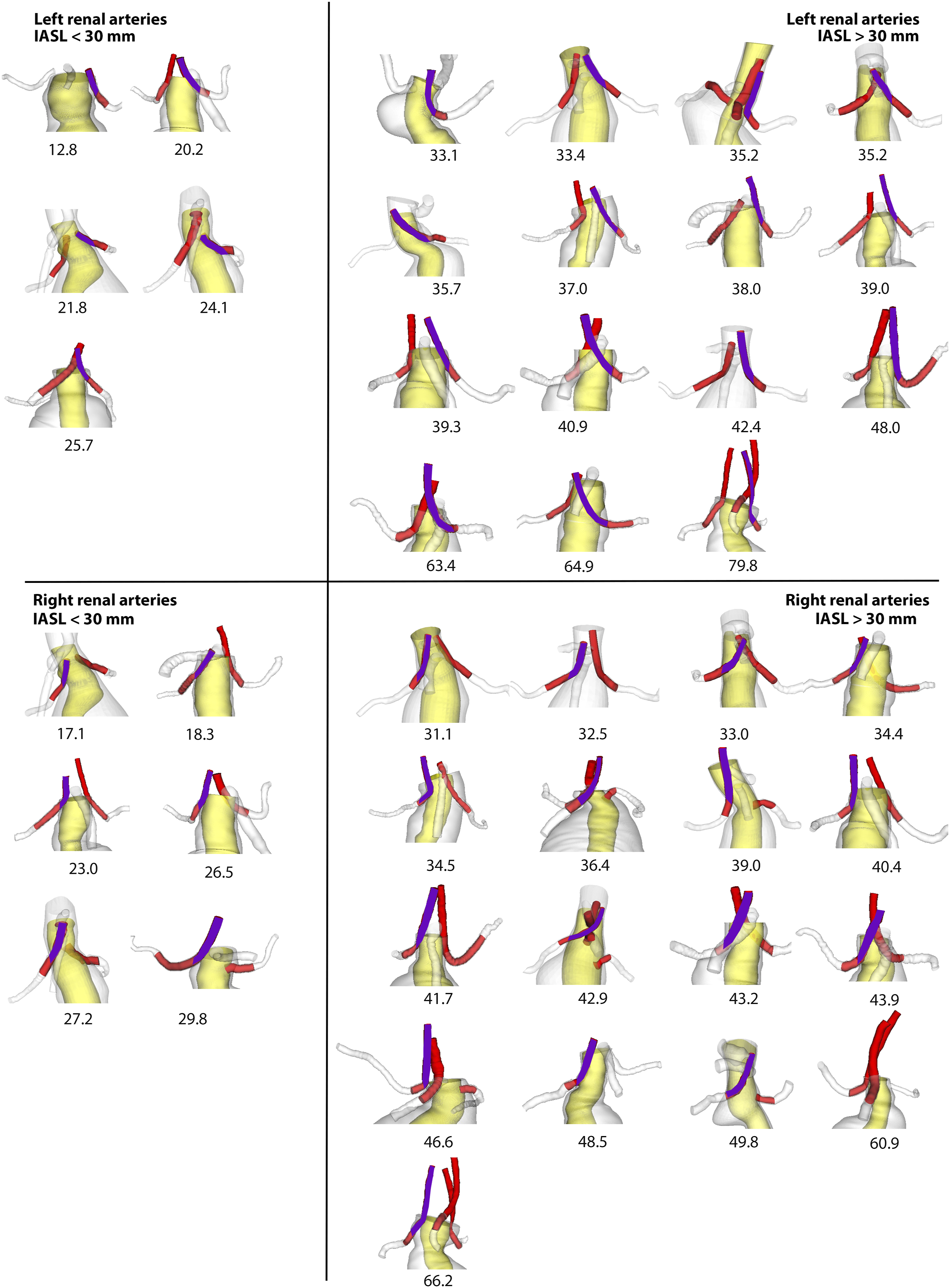
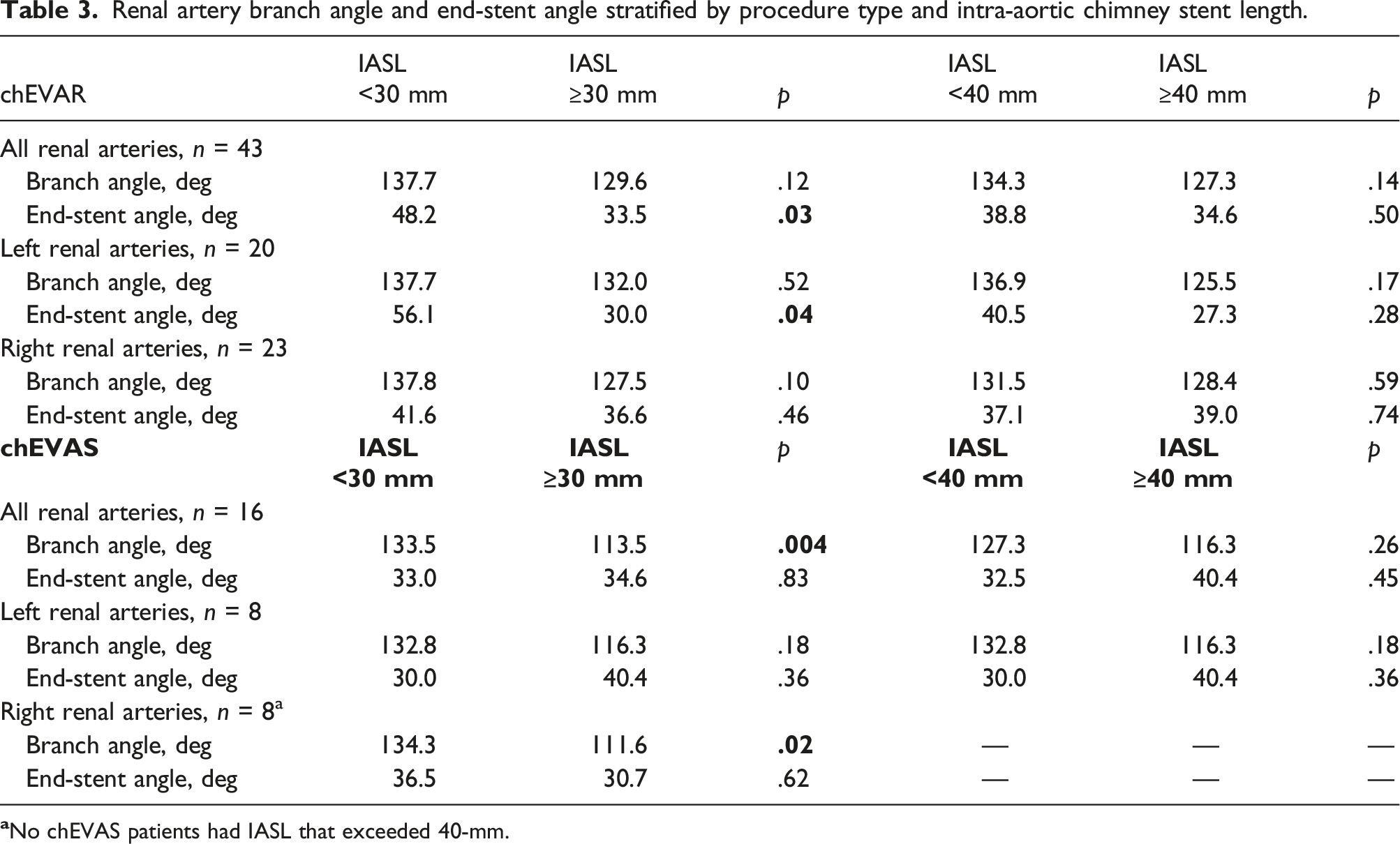
Quantification of renal chimney IASL for chEVAS and chEVAR is depicted in Figures 3 and 4, respectively. Mean IASL for renal arteries in chEVAR was significantly longer compared to chEVAS (39.2 vs. 26.3 mm, p = .003), a difference that was apparent in both right (38.8 vs. 26.8-mm, p = .02) and left (39.7 vs. 25.7 mm, p = .07) renal arteries (Table 2). No difference was noted in overall branch angle or end-stent angle based on procedure type. However, the two procedure groups did demonstrate differing geometric changes when stratified by pre-determined IASL thresholds (Table 3). Patients undergoing chEVAR with IASL <30-mm had significantly greater end-stent angle when evaluating all renal arteries (48.2 vs. 33.5°, p = .03) and left renal arteries individually (56.1 vs. 30.0°, p = .04). No difference in branch angle was noted from those undergoing chEVAR. In contrast, those undergoing chEVAS showed no difference in end-stent angle based on IASL thresholds, but did have significantly greater branch angle among those with IASL less than 30-mm when grouped by both all renal arteries (133.5 vs. 113.5°, p = .004) and right renal arteries (134.3 vs. 111.6°, p = .02). The longer IASL threshold of 40 mm failed to demonstrate any significant differences between procedure groups relative to branch angle or end-stent angle. Quantification of renal chimney intra-aortic stent length (IASL) in chEVAS configurations. Numbers represent renal chimney IASL in millimeters. Quantification of renal chimney intra-aortic stent length (IASL) in chEVAR configurations. Numbers represent renal chimney IASL in millimeters. Renal artery branch angle and end-stent angle stratified by intra-aortic chimney stent length, stratified by procedure type. aComparison between chEVAR and chEVAS patients. Renal artery branch angle and end-stent angle stratified by procedure type and intra-aortic chimney stent length.
Renal chimney stent type
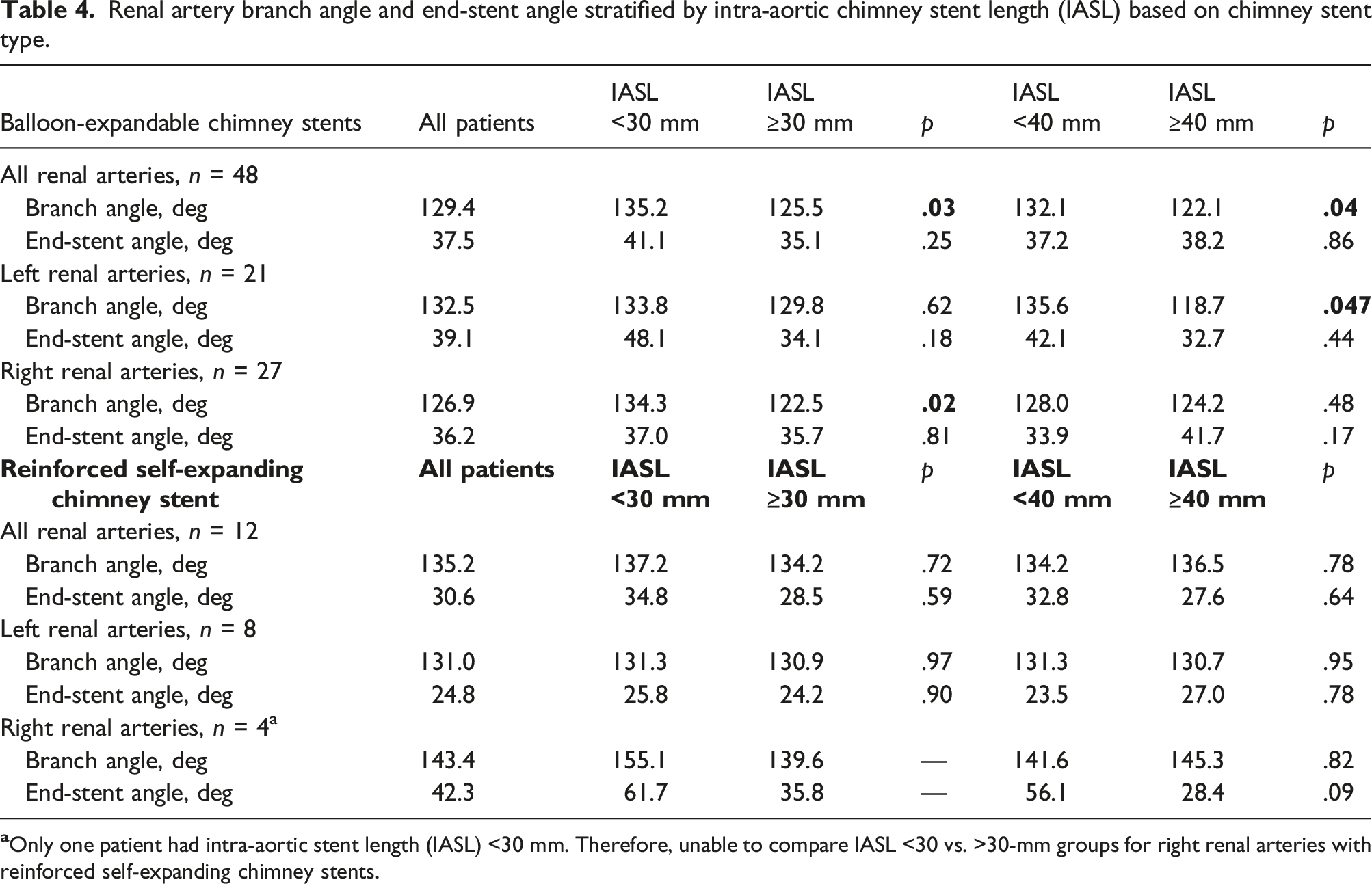
Renal artery branch angle and end-stent angle stratified by intra-aortic chimney stent length (IASL) based on chimney stent type.
Regression analysis
Figure 5 summarizes findings from regression analysis by plotting branch angles with respect to IASL stratified by both procedure type and renal artery laterality. A consistent negative correlation was discovered between IASL and branch angle for all renal arteries (R 2 = 0.05) and left renal arteries (R 2 = 0.13). Regression analysis continued to show an overall negative correlation between IASL and branch angle across both procedure types, particularly among chEVAS patients (R 2 = 0.37). The strongest negative correlation between IASL and branch angle was noted in right renal arteries in the chEVAS cohort (R 2 = 0.77). Renal artery branch angle versus intra-aortic stent length for all patients (ChEVAR + ChEVAS) and stratified by procedure type. A trend line with the corresponding coefficient of determination (R2) and significance value (p) is depicted.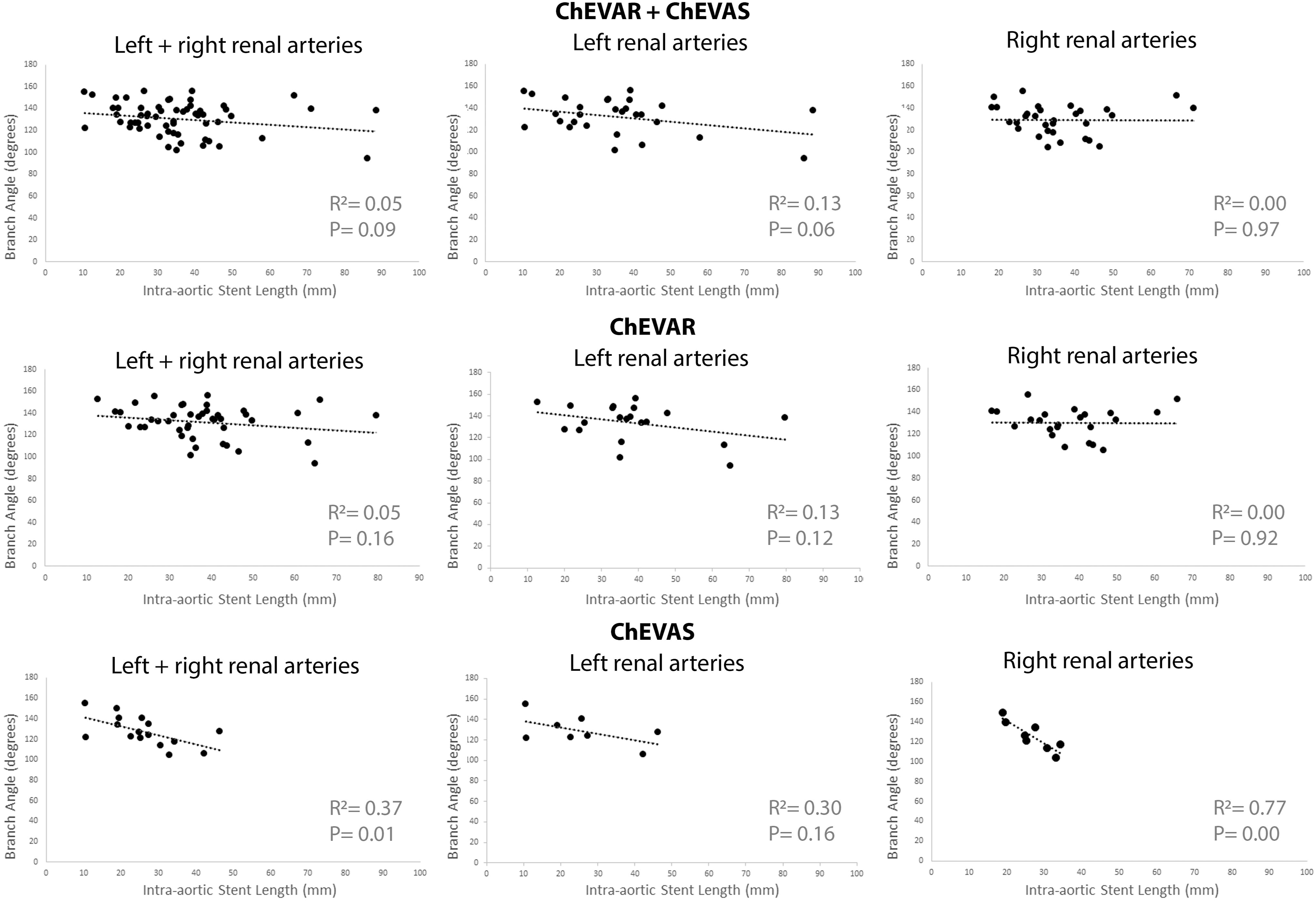
Clinical data
At a mean clinical follow-up period of 2.7 years, renal chimney stent patency was 96.6%. Two target vessel events occurred at a mean of 1.1 years following the index procedure. Both renal chimney events occurred in the chEVAR group and featured incidental chimney stent occlusion on routine postoperative surveillance imaging. Of note, both events involved left renal arteries with IASL >40 mm. No reintervention were performed in either case due to asymptomatic status and stable renal function. Neither patient exhibited any long-term renal function decline.
Discussion
The present study is the first to specifically examine the impact of IASL on branch vessel geometry following complex EVAR involving one or more renal artery chimney stents. Across our entire cohort, longer renal chimney IASL was associated with more perpendicular renal artery branch angles. This relationship between IASL and branch angle would suggest that longer renal chimney stents enable a more gradual and perpendicular transition across the renal ostia into the native renal arteries. Moreover, such longer chimney stent configurations would encourage less renal artery deformation and associated adverse clinical outcomes. Indeed, we did note that IASL beyond 30 mm was associated with significantly less end-stent angle in chEVAR (all renal arteries and left renal artery subgroups) and chEVAS (right renal artery only).
Previous analyses of cardiac pulsatility and respiratory-induced deformations of the renal arteries after complex EVAR showed bending stiffness of chimney stents dampened renal branch angulation, whereas it intensified bending of the renal arteries distal to the chimney stent.8,12 Indeed, one previous biomechanical analysis observed both chEVAR and chEVAS patients experienced approximately 10 times as much maximum bending of the renal arteries compared to a similar cohort with untreated AAAs. 12 While these findings were again noted in the present analysis, we also noted distinct differences between chEVAR and chEVAS procedures. Renal chimney stents were notably longer in the chEVAR group compared to the chEVAS group. This finding may be a reflection of physician preference owing to the perceived benefits of the polymer in chEVAS occupying the gutters between the parallel stent grafts and, as a result, a reduced need for additional proximal extension of the chimney stents. The significant increase in end-stent angle among those in the chEVAR group with IASL less than 30 mm further supports that having reduced IASL may force excessive downward pressure on the branch vessels, resulting in further exacerbation of angulation in the native renal artery distal to the chimney stent. This novel finding is the first to suggest a threshold IASL to elicit these extremes of angulation in more distal native renal artery. In addition, the non-significant trend toward decreased branch angle and end-stent angle among chEVAS patients compared to chEVAR patients supports previous findings that peak curvature and maximum curvature change locations were more proximal in chEVAS patients, an observation that suggests bending concentrated nearer to the renal ostium is related to the less-complaint nature of the sac-filling polymer. 12
Similar prior reports have consistently demonstrated geometric differences in the renal arteries based on laterality, including in cohorts featuring normal subjects, untreated AAAs, as well as those treated with both chEVAS and chEVAR.7,10–13 During the cardiopulmonary cycle, for instance, the left renal artery has been noted to yield an increase in mean curvature, whereas the right renal artery tends to straighten. 8 A recent analysis with chEVAS patients revealed left renal arteries experienced nearly three times the respiratory-induced end-stent angle change compared to right renal arteries. 12 We have long opined that this differential behavior may be driven by variance in geometric or mechanical constraints, such as the amelioration of dynamic motion of the right renal artery owing to the stability of the right renal artery provided by the inferior vena cava. Due to the lack of corollary mechanical support on the left side, the left renal artery is relatively free to move with visceral organ translation during the cardiopulmonary cycle. Our only two renal chimney events in this cohort involved left renal arteries with IASL >40 mm, although there was no evidence of any obvious kinking or stent compression on radiologic follow-up in either patient.
The influence of IASL on branch vessel geometry may be particularly important relative to the junctional segment of the chimney stent. This portion of the chimney stent that lies adjacent to the main body aortic endograft has been previously shown to be consistently narrower by an average of 15% compared to the proximal or distal chimney segments, and also experiences a greater degree of negative deformation compared to the distal segment. Based on a previous report, 14 we believe that this junctional segment has the highest distribution of kinking forces across the chimney stent and a corresponding relative lack of stabilizing radial forces, which are otherwise provided to the remaining portion of the chimney stent by the support offered by the aortic wall, main body device, and renal arterial wall in adjacent segments. As such, this junctional segment would be expected to be most susceptible to kinking, compression, or collapse.
Additionally, the suggestion that longer chimney stent configurations encourage less branch vessel deformation would support the design and early clinical success noted with branched thoracoabdominal aortic endografts, which feature longer target vessel constructs compared to conventional fenestrated correlative devices (e.g., reduced stent kinking, risk of “pull out”). Indeed, modest length redundancy has similarly been shown to confer improved biomechanical properties in prosthetic bypass grafts. 15 While target vessel events are rare, it does support the need for close radiographic surveillance and potential value of more aggressive intraoperative interrogation in select cases (e.g., intravascular ultrasound, reinforcement stent placement).
Limitations
Our analysis is limited by several important variables, including a relatively modest sample size. To enhance overall sample size, patients with concomitant chimney stents were included in this analysis under the assumption that the presence of a visceral stent(s) did not introduce geometric change at the level of the renal branch angle or end-stent angle. Also, the impact of physician preferences (e.g., chosen aortic bifurcated device or chimney stent graft type), local institutional practices, and device availability (e.g., chEVAS is not currently commercially available in the United States) on clinical and geometric outcomes in our cohort is unclear. Assessment of the mechanical properties (e.g., flexibility) of chimney stents, particuarly those with self-expanding stents internally reinforced with balloon-expandable stents, is also inherently limited. Moreover, our geometric analysis does not account for additional variables which may affect the mechanical properties of target vessels following complex EVAR, including renal flow resistance, intraparenchymal disease, size and type of renal chimney stent, tortuosity of the paravisceral aorta, presence of aortoiliac or renal ostial occlusive disease, and concomitant cardiovascular comorbidities. In addition, the postoperative imaging was performed at a single time point and, therefore, does not fully capture the potential for additional target vessel (renal chimney) events resulting from changes in stent-graft position or native vessel remodeling over time. The paucity of target vessel events (e.g., chimney stent occlusion) in our series also limits the ability to provide direct clinical correlation to our geometric observations.
Conclusion
In patients undergoing both chEVAR and chEVAS, renal chimney stents with longer IASL appear to exhibit less renal artery deformation, particularly as it relates to encouraging a more gradual and perpendicular transition of chimney stent across the renal ostium. This finding has important implications in terms of device design, case planning, and conduct of complex EVAR. Further elucidation of in vivo interactions of both aortic and renovisceral stent grafts with native vasculature is warranted to better understand the impact of such biomechanical changes on device durability and the potential for adverse clinical outcomes.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Brant W. Ullery is a consultant to Medtronic and Cook Medical, Inc. Christopher P. Cheng and Ga-Young Suh are consultants for Medtronic, W.L. Gore & Associates, Bard, Endologix, Cardinal Health, and Terumo. Andrew Holden is a medical advisory board member for Medtronic and W. L. Gore & Associates, as well as a clinical investigator for Endologix. The remaining authors have no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.