
Abstract
Objectives
We represent two cases of late proximal type I endoleak following EVAR with aneurysm expansion that were treated with a custom-made graft with inner branches.
Methods
Two patients of 87 and 82 years old were operated by EVAR 6 and 8 years ago for abdominal aortic aneurysm. Both had proximal type I endoleak with aneurysm sac expansion. Open surgery had a high risk, and a proximal aortic extension with a simple aortic cuff was not possible neither because previous EVAR grafts were already at the level of the renal arteries. A custom-made endograft with inner branches was planned as a fenestrated graft was not technically possible.
Results
We successfully treated both patients using a custom-made graft with four inner branches from Jotec (Cryolife, Kennesaw, GA). Three months’ follow-up CT scan did not show any endoleaks. All target vessels were patent with good conformability of the bridging stents.
Conclusion
The treatment of proximal type I endoleak using inner branches’ endografts is feasible. This novel technology might broaden the indications for complex aortic repair in a group of patients where fenestrated endografts are not possible.
Introduction
Type Ia endoleaks following endovascular aortic repair (EVAR) can be seen years after the initial procedure and need to be addressed promptly as they put the patient at risk of aneurysm rupture. It is estimated to occur in about 9% of cases, 1 and with the extensive use of EVAR, failed grafts with type I endoleak are expected to increase in the future. These endoleaks are often challenging to treat and need complex open surgical and endovascular skills like fenestrated (FEVAR) or branched (BEVAR) repairs. 2 There are no clear guidelines on how to manage type Ia endoleaks. Many factors are considered when choosing a treatment strategy: anatomic features for endovascular repair and physiologic characteristics for open surgery.
Recently, endovascular repair of complex aortic pathologies using inner branch devices (iBEVAR) have gained popularity due to some advantages over FEVAR and BEVAR; mainly, for the forgiving nature of branches over fenestrations in device orientation and position and the smaller working aortic diameter of inner over outer branches.
We describe two cases of late proximal type I endoleak with sac enlargement that were treated with this technology.
Case report
Case 1
An 87-year-old male was treated for a 55-mm abdominal aortic aneurysm (AAA) 6 years ago using a polymer ring endograft. Five years following the index procedure, an aortic neck dilation of 8 mm (20 mm–28 mm) with a type Ia endoleak and aneurysm sac progression of 20 mm was noted on a follow-up CT scan. Initially, a Palmaz stent of 18 mm was placed at the level of the polymer rings (the measured diameter of the circulating lumen at this level was 16 mm), and after a short-lived success, the endoleak recurred a year later with continuous expansion of the aneurysm (Figure 1(a)). (A) Pre-op CT scan of patient 1 with coronal images showing aortic neck dilation and proximal type I endoleak. (B) Graft plan for patient 1 with four downward inner branches. (C) Successful catheterization and stenting of all inner branches. The right renal stent is extended proximally inside the gate.
We planned a custom-made endograft with four inner branches (Jotec, Cryolife, Kennesaw, GA) which we intended to place in the supra-coeliac healthy aorta. The graft has a 30-mm proximal diameter that tapers down to 20 mm with a length of 135 mm. Since the previous EVAR main body had a 23-mm diameter, a 28-mm extension tube of 45 mm length was planned to be placed distally to ensure adequate seal. All branches have a caudal direction (Figure 1(b)).
20-, 7-, and 12-french (fr) sheaths were introduced, respectively, through a left femoral, right femoral, and right axillary artery cutdown. The initial attempt to bring up the endograft over a stiff wire was not successful due to a very diseased external iliac artery. After multiple balloon angioplasties and with the use of a through-and-through wire, we were able to advance the graft to a position where the inner branches’ orifices lie 1–2 cm above the intended target vessels.
Upon retrieval of the graft introducer, we encountered a complete avulsion of the left external iliac artery, beginning at its origin till the left common femoral artery (iliac on a stick). For this reason, a covered stent was not attempted; instead, an occlusive balloon was rapidly placed in the left iliac limb to achieve hemostasis, and a temporary shunt was connected from the right introducer through its side port to a 9-fr introducer that was placed in the left superficial femoral artery. From the contralateral femoral artery, the 28 mm x 45 mm extension tube was placed distally with 30 mm overlap with the branched endograft.
An 8-fr 90-cm sheath was then placed inside the 12-fr axillary sheath parallel to the through-and-through wire. The 12-fr sheath with the through-and-through wire provided a stable platform with minimal manipulation across the arch to avoid stroke.
The inner branches were consecutively cannulated using a vertebral catheter and a hydrophilic guidewire. Once we made sure we were inside the target vessel, a balloon expandable covered stent was deployed 2 cm inside each artery (Begraft plus, Bentley Innomed, Hechingen, Germany) (Figure 1(c)) over a Rosen wire (Cook Medical, Bloomington, Ind). A selective angiographic run was performed in each stent to rule out type Ic and III endoleaks.
Completion angiography confirmed the patency of all target vessels and the absence of endoleaks. A total fluoroscopic time (FT) of 124 min with a dose area product (DAP) of 1482 Gycm2 was noted.
Finally, a left ilio-femoral bypass was performed using a retroperitoneal approach.
The patient follow-up course was smooth. He was discharged home 10 days after the procedure. On a 3-month CT scan follow-up, all branches were patent and no endoleak was noted (Figure 2). Three months’ follow-up CT scan of patient 1. (A) Axial images showing a good accommodation of all inner branches. (B) MIP reconstruction showing an absence of endoleaks and a good conformability of all stents.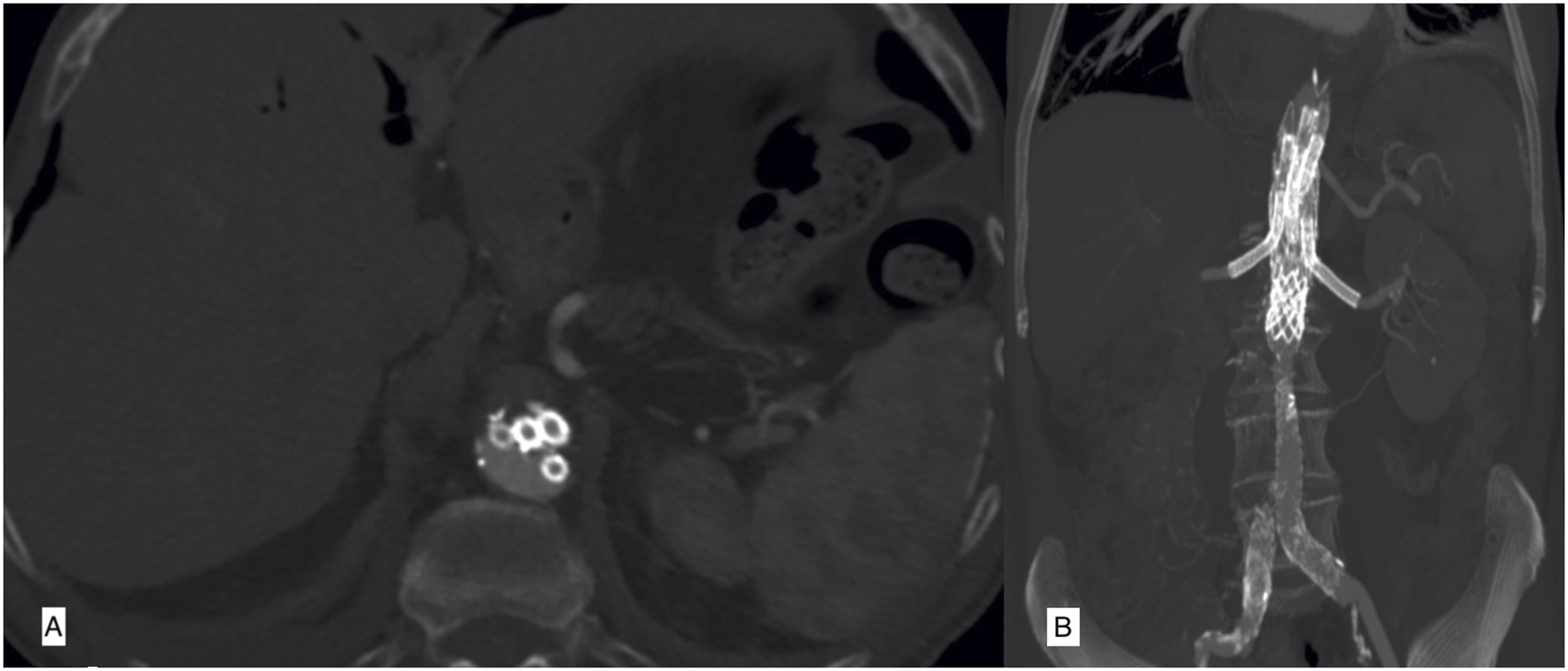
Case 2
An 82-year-old male patient was treated 8 years ago for an AAA of 7 cm using a polymer ring endograft. He was lost to follow-up and came back with a massive progression of this sac diameter to 10 cm. The proximal neck was completely effaced, and the polymer rings were inside the aneurysm (Figure 3(a)), but no migration of the graft had occurred. Due to his multiple co-morbidities, we opted for a total endovascular approach. Because of the upward direction of the right renal artery, an off-the-shelf BEVAR (where the graft has caudally directed outer branches) was not technically possible without sacrificing this vessel. We, therefore, designed a custom iBEVAR with four branches (Jotec, Cryolife, Kennesaw, GA) that was manufactured and delivered 30 days later. All inner branches were directed caudally except for the right renal (RR) branch which had a cranial direction. With a previous EVAR main body of 20 mm, a proximal graft of 33 mm tapering down to 24 mm was designed. (A) Pre-op CT scan of patient 2 with coronal views showing the proximal polymer ring inside the aneurysm (white arrow). (B) Successful catheterization of the right renal artery from the right femoral access. (C) Three months’ follow-up CT scan of patient 2 with MIP reconstruction in coronal view, showing a good conformability of renal stents.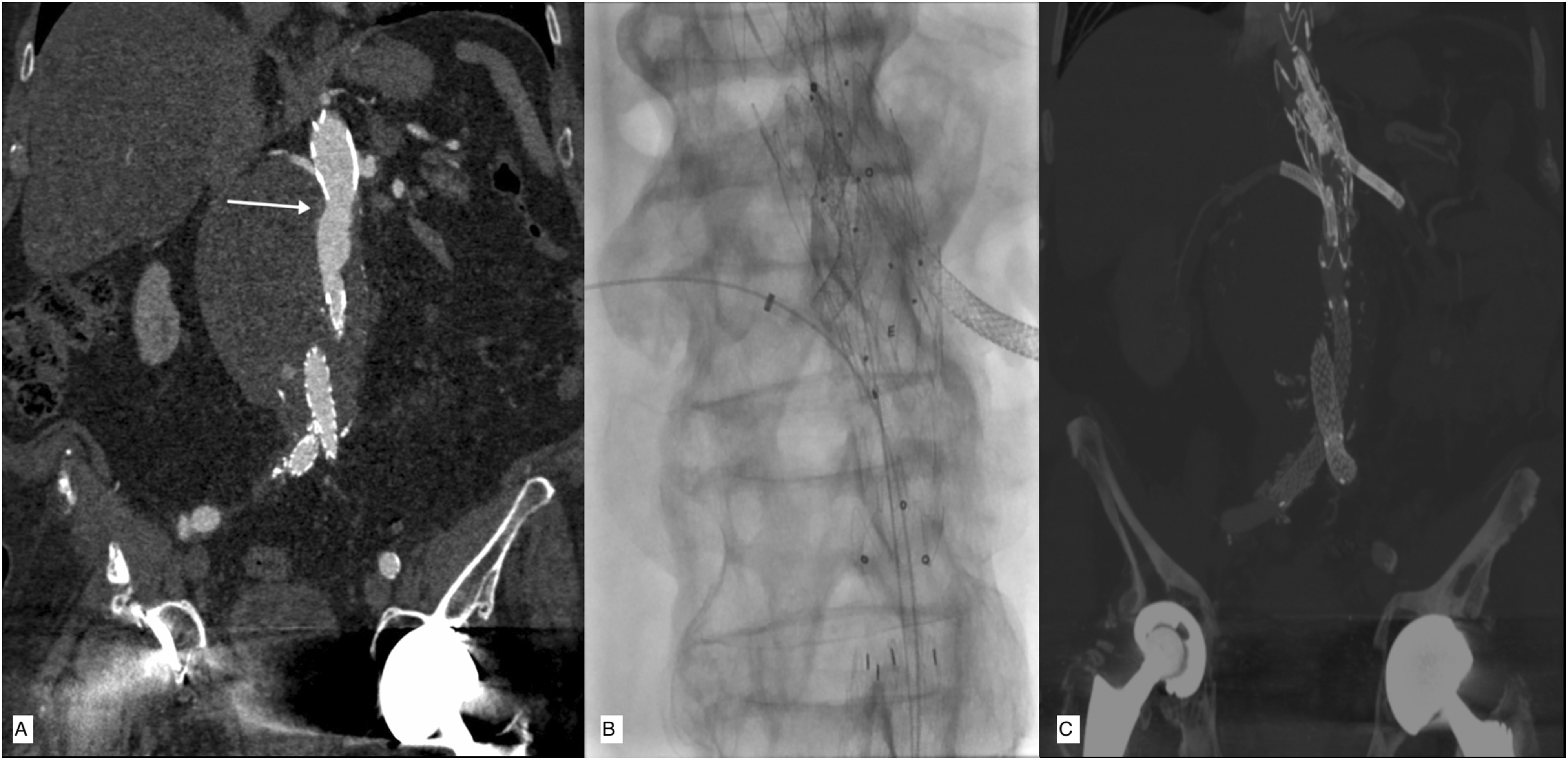
A left femoral and a right axillary artery cutdown were performed. The graft was introduced from the femoral approach and deployed, with the orifices of the downward branches 1–1.5 cm proximal to their respective targets and the RR branch orifice 1 cm distal to the respective artery. The graft introducer was removed and a 12-French 33-cm sheath was placed in the femoral artery. A 12-fr 45-cm sheath was placed in the right axillary artery to provide stability and limit manipulation in the aortic arch through which an 8-fr 90-cm sheath was telescoped. The three caudal branches were consecutively catheterized using a vertebral catheter and a hydrophilic guidewire, and then, balloon expandable covered stents (Begraft plus, Bentley Innomed, Hechingen, Germany) were deployed over a Rosen wire. The RR branch was catheterized from the femoral approach and subsequently stented with the same type of stents (Figure 3(b)). The final angiogram showed a successful repair without endoleaks. FT and DAP were 92 min and 1170 Gycm2, respectively.
The patient did well and was able to return home on day 5 and a 3 month CT scan showed the absence of endoleaks with patent branches and good stent conformability (Figure 3(c)).
Discussion
Late proximal type I endoleak following EVAR with subsequent loss of seal and aneurysm expansion can be due to multiple reasons, of which aortic neck dilation and disease progression are frequently found. Management of these endoleaks remains challenging whether by open or endovascular surgery.1,2,3
Open surgery with complete or partial graft extraction has been described but carries a high risk of mortality and morbidity in a group of patients that are already frail.3,4
Besides endostapling, endovascular repair is most often complex and requires advanced skills since proximal extension with a simple tube is rarely an option, and as most grafts from the index procedure are already positioned at the level of the renal arteries, any new repair should include the visceral aorta.
As for endostapling with the HeliFx system (Medtronic Vascular, Santa Rosa, CA), an 80.5% procedural success was shown is the ANCHOR registry. 5 . All neck diameters in this registry were inferior to 32 mm. In fact, good wall apposition is essential for the staples to enter the aortic wall. In the case of our patients, this technique was not adequate as there was no more wall apposition with the graft. Moreover, it was not possible neither, with the type of graft that had been implanted previously. Actually, besides the Gore Excluder (W. L. Gore & Associates, Flagstaff, Ariz), all expanded polytetrafluoroethylene grafts are outside the instruction for use of the endostaplers.
Parallel grafts have also been described with good mid-term results.6,7 Most of the patients were treated with one or two chimneys, and a significant percentage needed some type of reintervention for persistent endoleak (25–28%).6,7 In the series of Donas et al., the length of the new neck was 15 mm which raises some concerns about the durability of these repairs. 6 With more than two chimneys, the risk of gutter-induced endoleaks increases significantly. Nevertheless, since off-the-shelf devices are used, this technique is attractive in urgent cases.
FEVAR after failed EVAR has been described with good success rate.2,3,8 However, the presence of a previous graft makes this technique much more challenging because of the difficulty of rotating the graft introducer inside the previous EVAR limb, as well as the need to catheterize the target vessels through the struts of the suprarenal bare stent. In the two largest series published by Katsargyris et al. and Martin et al., both groups described technical difficulties related to poor torquability of the fenestrated device which was responsible for rotational misalignment and loss of target vessels in some cases. Despite this issue, it was possible to achieve technical success rates of 85% and 92.3%.2,3,8,9
While BEVAR is less critical in terms of accuracy of deployment, the diameter of the suprarenal aorta could be a major limitation to this technique since at least 25 mm of working lumen is required for the branches to open freely. In addition, more aortic coverage is required, and thus, more spinal cord ischemia is to be expected. In urgent cases where a custom-made graft is not available, the off-the-shelf T-branch (Cook Medical, Bloomington, Ind) is very valuable. 10 Other investigational grafts like the Unitary Manifold (Sanford Health, Sioux Falls SDak) and the TAMBE (W. L. Gore & Associates, Flagstaff, Ariz) have been described with clinical success, but they remain investigational devices and are not commercialized yet.11,12
The concept of inner branches has evolved rapidly in recent years. Two grafts currently exist on the market. The first, from Cook, is only available as an investigational device and is limited to a few centers. Conversely, the Extra-design engineering endograft with inner branches (Jotec, Cryolife, Kennesaw, GA) has obtained the CE mark and is currently obtainable.
iBEVAR has many advantages over FEVAR and BEVAR. For instance, in comparison to FEVAR, downward-oriented target vessels are easier to cannulate. Severe neck angulation which is an important limitation for FEVAR is less crucial. Compared to BEVAR, iBEVAR necessitates a smaller working lumen. Moreover, less aortic coverage is needed which might lower the risk of spinal cord ischemia. Nevertheless, we still use measures to prevent this complication like keeping the mean arterial blood pressure above 75 mmHg and the hemoglobin levels above 10 g/dL. We only use spinal drainage if neurologic symptoms occur.
An off-the-shelf endograft with inner branches also exists on the market (E-nside, Jotec, Cryolife, Kennesaw, and GA), but this option was not possible in our second case because of the cranial direction of the right renal artery, and even though it was possible to use it in our first case, we thought that a custom-made device will limit aortic coverage and provide more ease with target vessels’ cannulation.
Abisi et al. published their experience with inner branches in over 18 patients, and 5 had type I endoleak after EVAR. Technical success with adequate seal was obtained in all patients at 12 months’ follow-up. Reintervention for primary assisted patency of renal stents was necessary in one patient. 13
In our two cases, a fenestrated graft, which is our preferred choice for failed EVAR, was not used. In the first case, a tapered graft from 30 to 20 mm to accommodate the previous Palmaz stent of 18 mm was not technically possible. In the second case, we were concerned by the long production time in a patient with a 10-cm AAA. Our preference to FEVAR is based on the better patency outcome of renal fenestrations in comparison to branches. 14
Target vessels’ cannulation in early BEVAR cases were performed from an axillary access, but recently, with the use of the steerable sheath, a femoral approach has become very popular, and some authors completely abandoned the former approach. 15 On one side, the femoral approach avoids maneuvers in the aortic arch, is more ergonomic for the operators, and requires less radiation, but on the other side, it incurs keeping a large occlusive sheath in the iliac vessels with subsequent lower limb ischemia with a potential increased risk of paraplegia. In our case, since it was our early experience with this device, we preferred to use an axillary approach to limit procedural time.
There is still no clear consensus on balloon vs self-expandable covered stents in branched technology. Our preference for the former type resides in the versatility of length, the possibility to adapt its diameter to the target vessel and the branch and its precise deployment.
One drawback of this inner branch device remains its large profile (24 fr) which contributed to an external iliac artery avulsion in our first case. Stacking four inner branches in proximity to each other in a restrained space is probably why the device is so bulky (Figure 4). This issue might be overcome by customizing the placement of branches on different levels but this implies using longer bridging stents and requiring more aortic coverage. On the other hand, constructing an iliac conduit increases the morbidity of the intervention since an invasive procedure is needed, which might limit the use of this device in some patients. Intraluminal view of an iBEVAR device with four branches in proximity.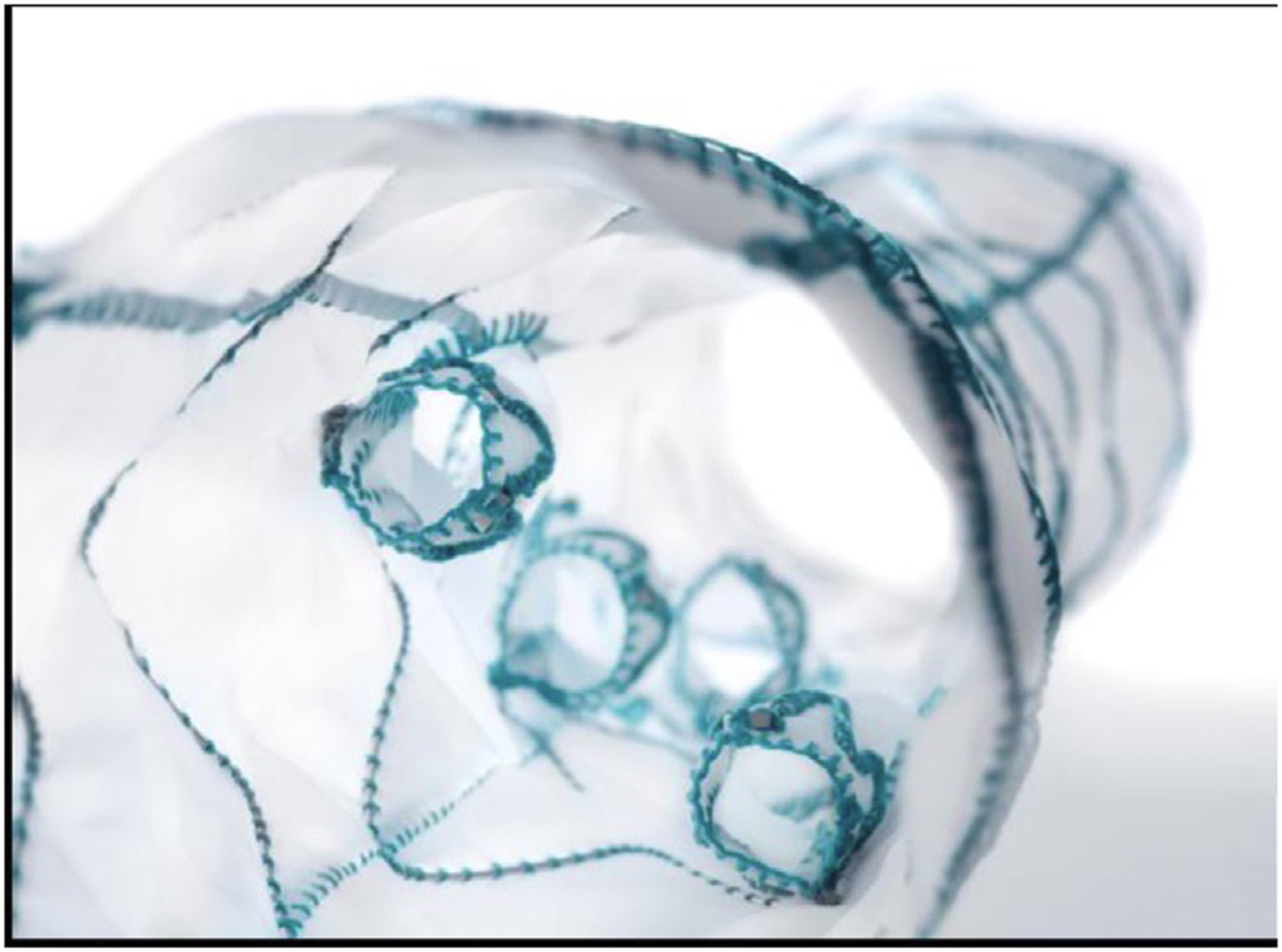
Finally, as this device is relatively new, longer follow-ups are needed to conform the durability of this repair.
Conclusion
Rescue of failed EVAR with proximal type I endoleak using inner branches is feasible and in some cases, can be the only possible endovascular solution. Longer follow-ups are needed to validate this relatively young technology.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.