
Abstract
Background
Mural thrombus in abdominal aortic aneurysm (AAA) has been associated with increased rates of aneurysm growth as well as adverse cardiovascular events. The extent of mural thrombus in thoracoabdominal aortic aneurysms has recently been linked to 1-year mortality following endovascular repair and has been hypothesized as a marker for reduced cardiac reserve. This study investigates whether the extent of mural thrombus in infra-renal AAA is associated with 5-year mortality following elective repair.
Methods
Retrospective review of all patients undergoing elective infra-renal AAA repair at a single academic medical center between 2007 and 2016 was performed. The following variables at the time of surgery were investigated for association with 5-year mortality: age, sex, ethnicity, insurance status and co-morbidities, repair type, renal insufficiency, end-stage renal disease on dialysis, history of smoking, coronary artery disease, congestive heart failure, diabetes mellitus, hypertension, stroke, chronic obstructive pulmonary disease, body mass index category, AAA diameter, and ratio of aortic thrombus to total aneurysm diameter.
Results
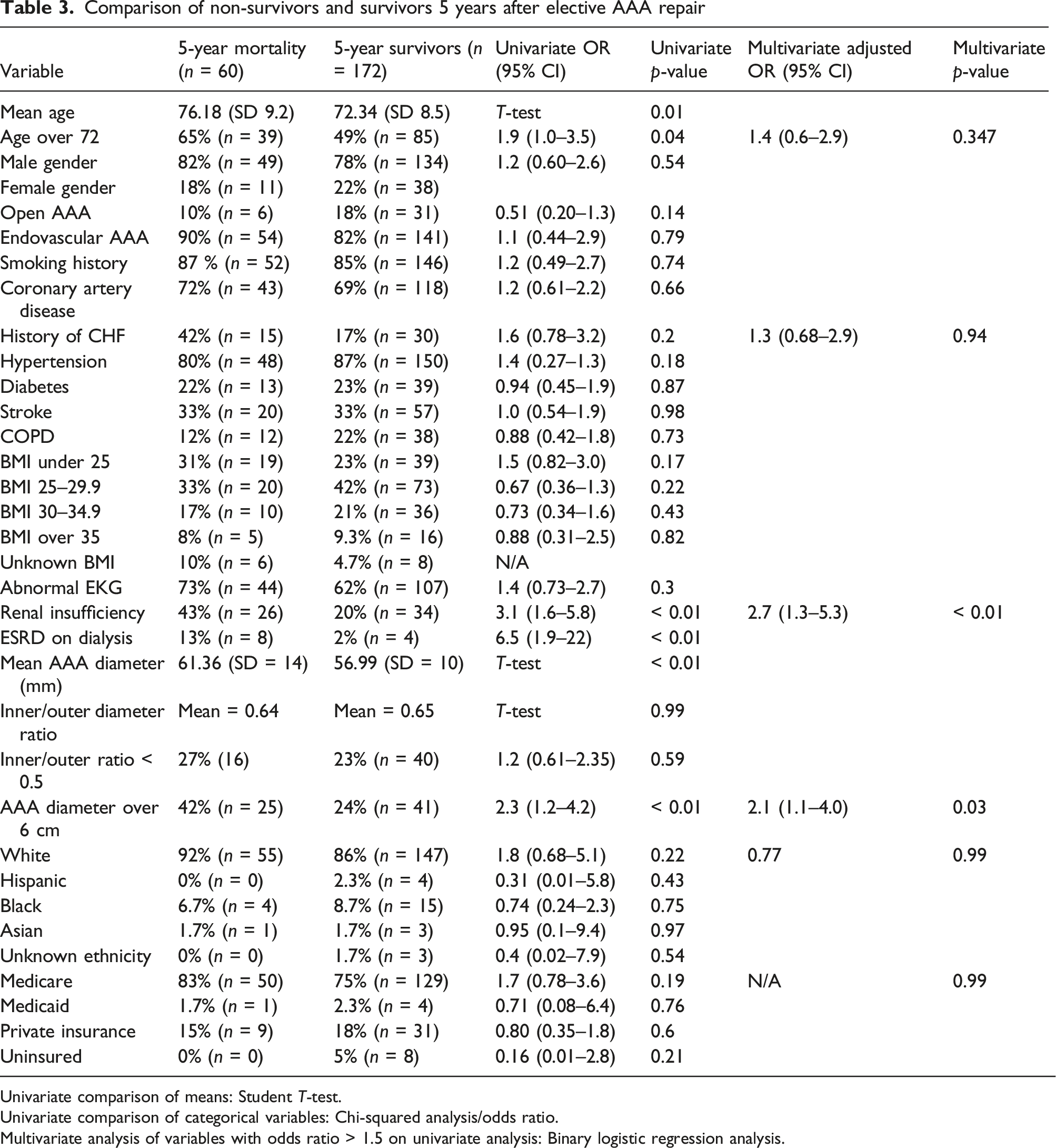
Amongst 427 patients undergoing infra-renal AAA repair during the study period, 232 met extensive inclusion criteria. Univariate analysis found mean age (76 vs 72, p < 0.01), age cohort over 72 years (OR = 1.9, p = 0.04), renal insufficiency (OR = 3.1, p < 0.01), ESRD (OR = 6.5, p < 0.01), AAA diameter 6 cm or greater (OR = 2.3, p < 0.01), and mean AAA diameter (61.36 vs 56.99 mm, p < 0.01) all predictive of 5-year mortality. Multivariate analysis revealed renal insufficiency (p < 0.01) and AAA diameter 6 cm or greater (p = 0.03) to be significantly associated with 5-year mortality. The extent of mural thrombus was identical between 5-year survivors and non-survivors. The mean inner to outer AAA diameter was 0.65 in the survivor cohort and 0.64 in the mortality cohort. Inner to outer ratio of < 0.5 was identified in 23% of 5-year survivors and 27% of the mortality group.
Conclusions
In our experience, the extent of mural thrombus in AAA does not influence long-term survival after elective repair. AAA repair may provide protection against circulating components of mural thrombus which have the potential to promote atherosclerotic-related adverse events. Patients with renal insufficiency and larger AAA have increased risk of mortality 5 years after elective repair.
Introduction
The extent of mural thrombus in abdominal aortic aneurysm has been associated with increased rates of aneurysm growth as well as adverse cardiovascular events.1–3 Further, larger AAA diameter at the time of elective repair is linked to increased risk of long-term mortality.4–6
The extent of mural thrombus in thoracoabdominal aortic aneurysms (TAAA) has recently been linked to 1-year mortality following endovascular repair. Patrick et al. 7 presented the concept that patients with marginal cardiac reserve compensate by developing aneurysm mural thrombus. Patients with lower ratios of inner to outer aortic diameter (more mural thrombus) were shown to have significantly reduced 1-year survival following endovascular repair of TAAA. Aneurysms, particularly TAAA which have a large aneurysm volume, create a need for increased cardiac output. The authors suggest that the formation of mural thrombus is a physiologic response to preserve a patient’s ejection fraction. The subsequent TAAA repair has the potential to increase afterload which makes patients with reduced cardiac reserve more vulnerable to experience mortality.
While these findings were significant for thoracoabdominal aortic aneurysms, similar investigation has not yet been done within the realm of infra-renal abdominal aortic aneurysms (AAA). Infra-renal aortic aneurysms encompass a significantly reduced total aneurysm volume relative to TAAA, and thus, the above concept thus has questionable applicability to AAA. This study investigates whether the extent of mural thrombus in infra-renal AAA is associated with 5-year mortality following elective repair.
Methods
Retrospective review of all patients undergoing elective repair of infra-renal abdominal aortic aneurysm at Loyola University Medical Center between 2007 and 2016 was performed. Both open and endovascular repair were included in the analysis. Case identification by query of CPT codes 35081, 35102, and 34800, 34805 was conducted by bio-informatics. CPT codes for open repair of ruptured aneurysms (35082 and 35103) were not included. Electronic medical records (EMR) review was then performed for all cases. In terms of our routine practice, we follow Society of Vascular Surgery recommended indications for AAA repair at a diameter of 5.5 cm in men and 5 cm in women. 8 Consideration of repair at smaller diameters is made for symptomatic aneurysms, saccular morphology, and rapid aneurysm growth.
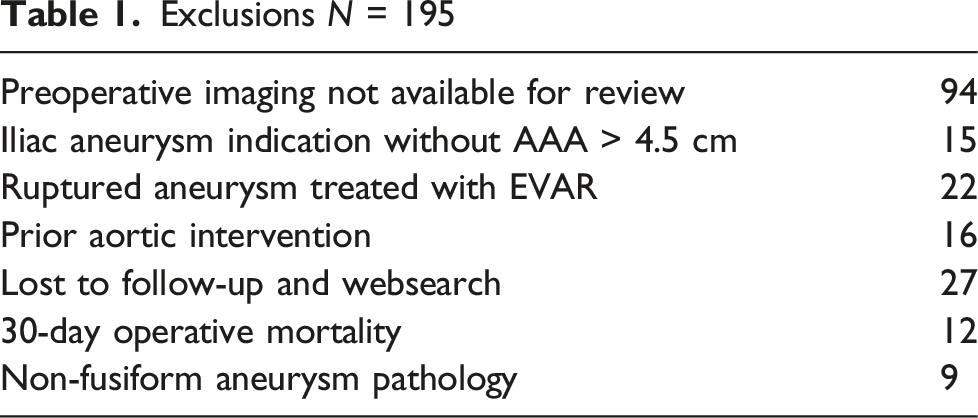
The primary outcome investigated was mortality 5 years after index operation. Inclusion in the study mandated either 5 years of documented follow-up or confirmation of mortality between 30 days and 5 years. Only elective repair of fusiform, infra-renal aorto-iliac aneurysm morphology was included. Patients were excluded for any of the following scenarios: preoperative imaging not available (or inadequate) for review of the extent of mural thrombus, iliac aneurysm indication with abdominal aortic component less than 4.5 cm maximal transverse diameter, ruptured aneurysm, prior aortic intervention, lost to follow-up before 5 years with no confirmation of mortality as source, 30-day operative mortality, and non-fusiform aneurysm pathology (saccular aneurysm, dissection, penetrating ulcer, trauma, concomitant supra-renal aortic intervention). Before 2017, endovascular repair (EVAR) for ruptured aneurysm did not routinely have distinct CPT code placement, and thus, these ruptured cases were excluded after EMR review. Mortality status at each 1-year interval was recorded to allow for survival curve creation. This was done as a point-to-point annual analysis and included all patients in the study.
The following variables at the time of surgery were investigated as potential predictors of mortality within 5 years: age, gender, ethnicity, insurance status, open repair, endovascular repair, renal insufficiency, end-stage renal disease on dialysis, history of smoking, history coronary artery disease (CAD), history of congestive heart failure (CHF), diabetes mellitus (DM), hypertension (HTN), history of stroke, chronic obstructive pulmonary disease (COPD), abnormal electrocardiogram (EKG), body mass index category (BMI) in kg/m2, AAA diameter, and ratio of aortic thrombus to total aneurysm diameter.
Insurance status was categorized as Medicare, Medicaid, private insurance, and uninsured. Renal insufficiency was defined as glomerular filtration rate of < 60 mL/min at the time of surgery. Any history of CHF, stroke, HTN, DM, and CAD was included as a positive finding regardless of the current manifestations or lack thereof associated with medical management of these co-morbidities.
The AAA diameter was measured at the location of maximal transverse diameter perpendicular to the centerline of aortic flow between the renal arteries and iliac bifurcation. Aortic mural thrombus burden was also determined at the level of the largest AAA diameter. The inner flow channel on arterial phase contrast at this level was measured and divided by the total aortic diameter to determine the inner-outer ratio. Aneurysms with larger thrombus burden relative to maximal aortic diameter thus have inner-outer ratios closer to zero, and aneurysms with trace mural thrombus have ratios closer to 1. Figure 1 provides examples of aneurysm measurements. The analysis of CT scans was performed by individuals who at that time were blinded as to mortality status. With respect to determining a threshold of mural thrombus to create a categorical variable, a cutoff level of 0.5 for inner to outer diameter was utilized because it correlates with the median amount of thrombus amongst our patients and based on the analogous analysis performed by Patrick et al.
7
AUC analysis revealed there was no level of inner-to-outer aortic diameter ratio that corresponded to a meaningful sensitivity or specificity with respect to association with 5-year mortality. The area under the curve was 0.509 Examples of measurement of inner and outer AAA diameters. Blue lines represent inner diameter and yellow lines outer diameter. Inner-to-outer ratio is calculated by dividing the inner diameter in millimeters by the outer diameter in millimeters. Thus, ratios closer to 1 represent minimal mural thrombus, and ratios closer to 0 represent more extensive mural thrombus.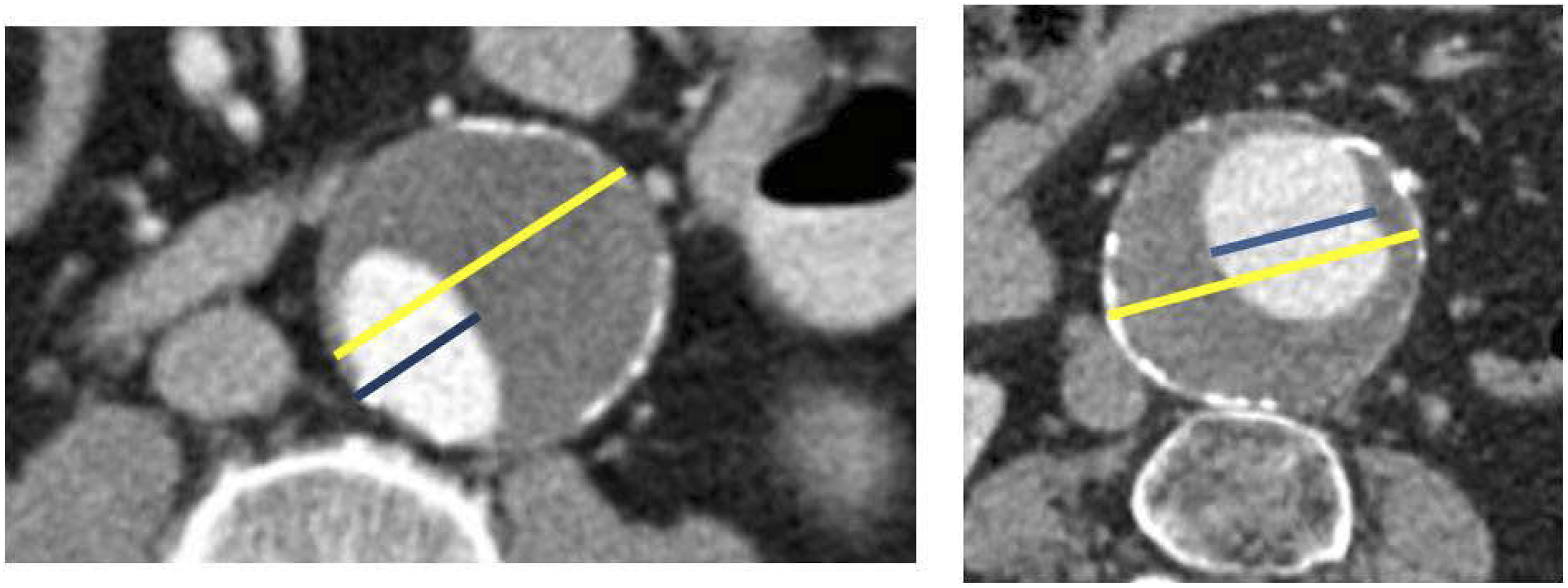
Statistical analysis was performed with IBM SPSS version 28 software. Univariate analysis of association with 5-year mortality was first conducted using chi-squared statistic and odds ratio calculation for categorical variables and student t-test for comparison of means for ordinal variables. Binary logistic regression was then performed for the outcome of 5-year mortality using the variables which had an odds ratio > 1.5. Given direct correspondence with renal insufficiency, ESRD was not included in regression analysis to prevent redundancy as those patients were included in the renal insufficiency cohort as well.
Results
Exclusions N = 195
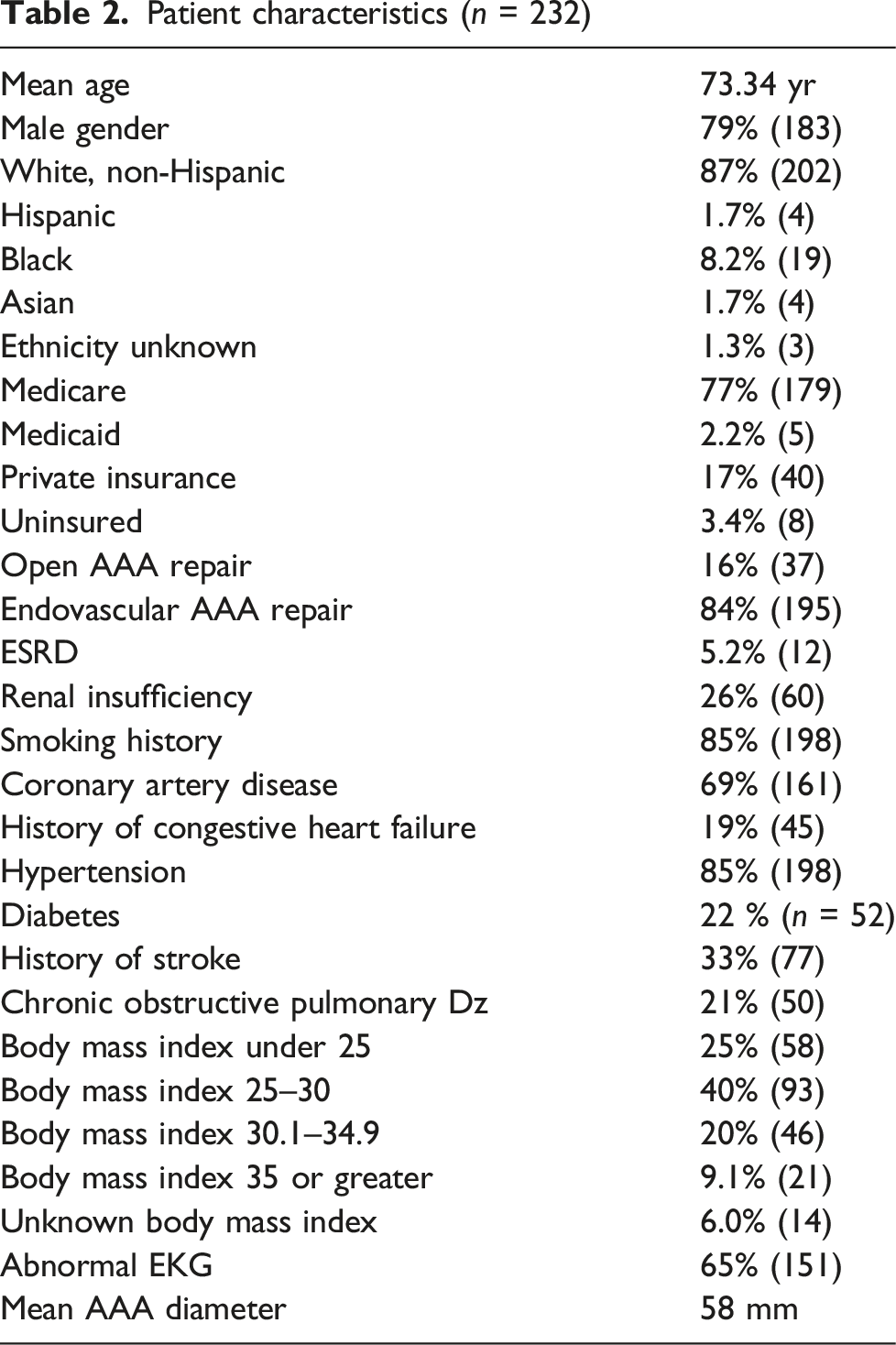
Patient characteristics (n = 232)
Comparison of non-survivors and survivors 5 years after elective AAA repair
Univariate comparison of means: Student T-test.
Univariate comparison of categorical variables: Chi-squared analysis/odds ratio.
Multivariate analysis of variables with odds ratio > 1.5 on univariate analysis: Binary logistic regression analysis.
Binary regression analysis of the categorical variables with odds ratios > 1.5 (other than ESRD) revealed renal insufficiency (p < 0.01) and AAA diameter 6 cm or greater (p = 0.03) to be significantly associated with 5-year mortality.
The extent of mural thrombus was identical between 5-year survivors and non-survivors. The mean inner to outer AAA diameter was 0.65 in the survivor cohort and 0.64 in the mortality cohort. Inner-to-outer ratio of < 0.5 was identified in 23% of 5-year survivors and 27% of the mortality group.
Survival curves comparing percent survival in AAA diameter, renal insufficiency, age, and aortic thrombus ratio cohorts are presented in Figure 2. Survival curves for 5-year survival comparing (A) AAA under 6 cm to AAA 6 cm and above, (B) AAA repair in patients with and without baseline renal insufficiency, (C)AAA repair in patients with low and high AAA mural thrombus burden, and (D) patients above and below 72 years old.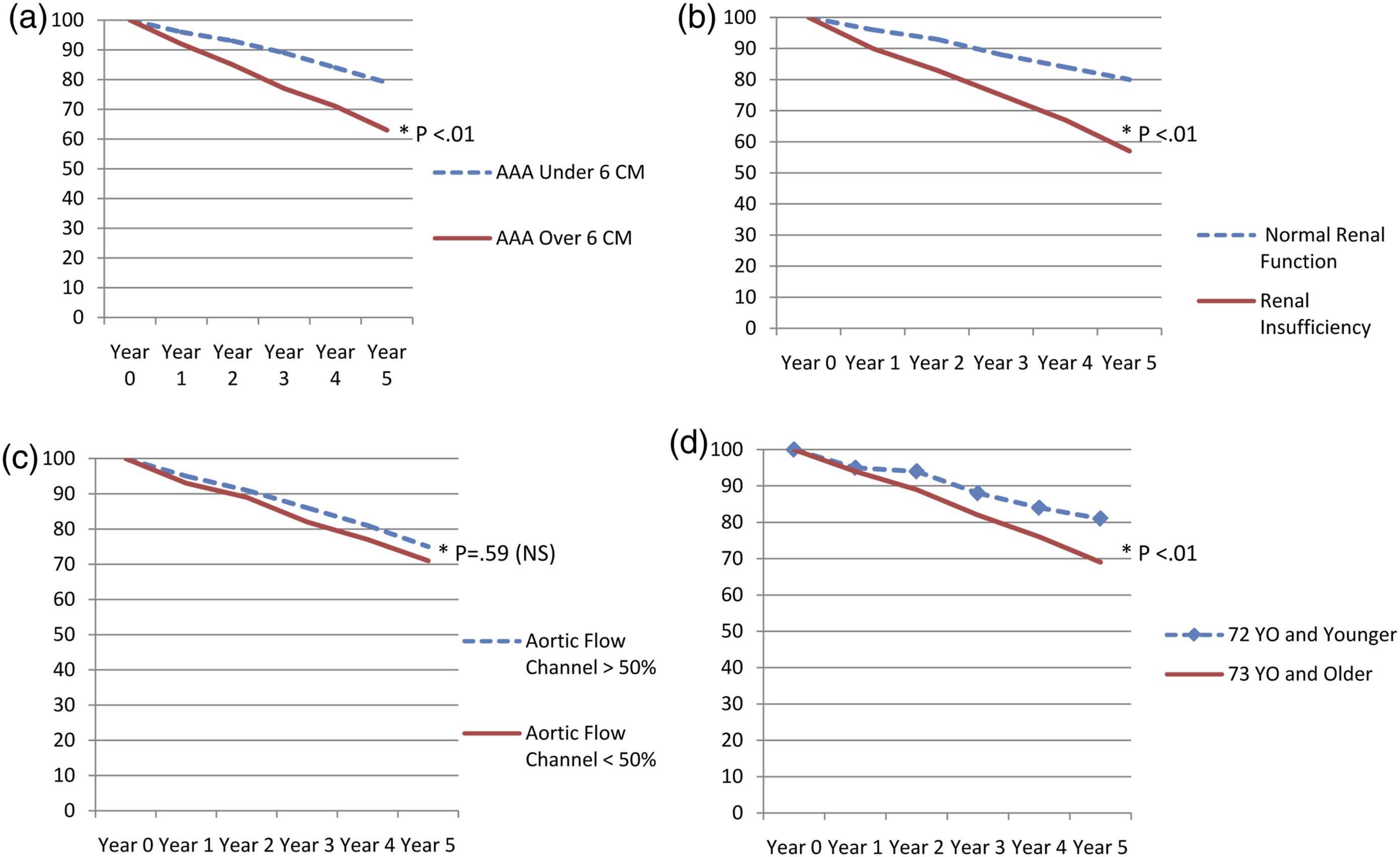
Discussion
Our study did not find an association between extent of mural thrombus and 5-year mortality after elective repair. The “who and why” of aortic aneurysm mural thrombus is poorly defined. It was thus with great interest that we read the analysis by Patrick et al. 7 regarding endovascular repair of TAAA. The concept that patients who have reduced cardiac reserve more readily form mural thrombus as a compensatory mechanism to reduce required stroke volume is quite intuitive. The subsequent decreased aortic compliance associated with stent grafting extensive aortic length was then postulated to serve as a source of increase afterload and progression to heart failure. This final postulation does not apply as well to infra-renal AAA as far less aorta is replaced or stented. Nevertheless, the impetus toward thrombus formation due to reduced cardiac reserve would theoretically apply to infra-renal AAA and might have an associated reduced long-term survival association.
The other leading supposition regarding AAA mural thrombus formation is that it occurs in patients with a relative hypercoagulable state. Thrombus components have been postulated to circulate and promote atherosclerotic plaque activation and increase acute coronary and cerebrovascular events in patients who have not yet undergone AAA repair.
8
Additionally, the presence of AAA may be associated with relative hypercoagulability with associated potential for increased cardiovascular events.
9
Elevated fibrinogen and
Both of these mechanisms (reduced cardiac reserve and hypercoagulability) would thus create potential to increase long-term mortality in patients with higher burdens of aortic mural thrombus. In this light, we conducted this investigation. The rationale for investigating a potential association between the extent of mural thrombus and long-term survival was not to seek any adjustment in clinical management of AAA per se. Rather, identifying any such association would have potential biomedical implications. While the inquiry proved negative, it is novel and addresses an unanswered question. This is only study we are aware of that has evaluated the extent of mural thrombus and long-term survival after elective AAA repair.
Increased amount of mural thrombus has been consistently associated with a more rapid rate of aneurysm growth.1–3 Intraluminal thrombus has been linked experimentally to reduced oxygen diffusion to the aortic wall, inducing tissue hypoxia and contributing to wall weakening.13,14 Despite lower peak wall pressure, aneurysms with higher thrombus burden tend to rupture at modestly higher rate than equally sized aneurysms with less thrombus. 15 On a molecular level, AAAs with more extensive mural thrombus have increased levels of matrix metalloproteinase, elastin degradation, and smooth muscle cell apoptosis.16–18
Our overall impression regarding aortic mural thrombus is that of an association with increased aneurysm growth and cardiovascular morbidity before aneurysm repair, and equivalent long-term survival after aneurysm repair.
We found larger AAA diameter at the time of surgery to be strongly associated with reduced 5-year survival. Patients with AAA 6 cm or larger experienced over two-fold higher 5-year mortality (42% vs 21% in those < 6 cm). Mean diameter in the 5-year mortality cohort was 61.36 mm relative to 56.99 mm in 5-year survivors (p < 0.01). This is very consistent with extensive existing literature.4–6 This is owed to higher rates of co-morbidity in patients with larger aneurysms with increased rates of CAD, CHF, renal disease, COPD, and malignancy in patients with larger aneurysms. Our own prior institutional review of patients undergoing EVAR had revealed higher operative risk profile in patients with larger aneurysms. 19
Advanced age was another statistically significant predictor of 5-year mortality we encountered (mean age = 76.18 vs 72.34, p < 0.01). Patients over 72 years were nearly twice as likely to experience 5-year mortality relative to the younger cohort (31% vs 19%). This finding is as expected and consistent with prior reports. 20 Aging is associated with increased rates of malignancy, frailty, stroke, and vulnerability to respiratory failure.
Renal insufficiency and ESRD were associated with reduced long-term survival at a statistically significant rate. Patients with baseline eGFR < 60 mL/min/1.73 m2 experienced 5-year mortality at a higher rate than those with normal renal function (43% vs 20%). Throughout the vascular literature, patients with ESRD undergoing major arterial intervention have reduced long-term survival relative to cohorts with normal renal function.20–22 Only 12 patients in our study were on dialysis at the time of surgery and 75% of them experienced 5-year mortality. This re-affirms the importance of completing thorough risk assessment before recommending elective aneurysm repair. SVS guidelines should particularly be adhered to when performing AAA repair in ESRD patients. 8
Other common co-morbidities of smoking history, CAD, history of CHF, COPD, elevated BMI, abnormal EKG, stroke, and hypertension did not predict long-term mortality.
With respect to potential clinical implications of our analysis, recognizing the demographic predictors of long-term mortality after AAA has potential utility. Cardiovascular-related events are the leading cause of long-term mortality in AAA patients. Emphasizing the critical nature of compliance with medications, smoking cessation, blood pressure control, and regular follow-up with primary care physicians is particularly vital for patients with advanced age, renal insufficiency, and larger aneurysms.
We did identify weaknesses in our study. An ideal analysis would involve investigating echocardiogram and stress test findings. This would allow for comparison of functional cardiac data amongst patients with various extents of mural thrombus and survival durations. Unfortunately, the EMR did not consistently capture this data in the early years of the cohort. Any single institutional review is subject to treatment and outcome biases and may not be universally applicable to outside facilities. That stated, our long-term survival rate is consistent with that in other robust analyses.20–25 We excluded patients who experienced 30-day mortality as the primary purpose of the study was to investigate the effects of extent of mural thrombus on long-term survival. Our study design was that of a one-time binary outcome of alive versus deceased at each yearly interval up to 5 years. Nevertheless, this does not undermine statistical validity of our binary logistic regression outcome analysis. We were unable to obtain social security death index access for this study, and thus, all of the survival data was obtained via electronic medical records review. Some of this included using the “care everywhere” feature. Therefore obtaining precise date of mortality for all patients was not feasible, and we were unable to perform Cox regression based on time-to-event analysis. We were, however, able to determine in what postoperative year mortality did occur. Any patient who was lost to follow-up or did not have survival status documented was excluded. Therefore, all of the data and outcomes presented in the study are based on hard data with no censored “prospecting” in the survival curves. Binary logistic regression analysis of a single yes/no outcome is very much statistically valid when the data is complete without censoring. It is important to note that the data on our survival curves are point-to-point actual (not actuarial) data at yearly intervals and not censored Kaplan Meier analysis survival prediction curves.
Conclusions
In our experience, the extent of mural thrombus in AAA does not influence long-term survival after elective repair. AAA repair may provide protection against circulating components of mural thrombus which have the potential to promote atherosclerotic-related adverse events. Patients with renal insufficiency and larger AAA have increased risk of mortality 5 years after elective repair.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.