
Abstract
Background
Behçet’s disease (BD) is a rare form of systemic vasculitis that affects small to large vessels. It is characterized by mucocutaneous, pulmonary, cardiovascular, gastrointestinal, and neurological manifestations. Large vessel involvement may occur in a third of cases. Veins are usually more affected than arteries. Furthermore aneurysms are the most frequent arterial complication.
Case presentation
A 41-year-old man presented with multiple arterial aneurysms. He had previous medical history of a right popliteal aneurysm treated with a reversed femoro-popliteal venous bypass, long-term steroids and immunosuppressive treatment. On admission, diagnostic computed tomography angiography revealed multiple aneurysms, including an 87 mm aneurysm of the femoro-popliteal bypass and an abdominal aortic and left common iliac artery aneurysm. He received an intensification of medical treatment with methylprednisolone and infliximab intravenous infusion. Aorto iliac artery aneurysms were treated by infrarenal bifurcated stent graft implantation. The aneurysm of the venous femoro-popliteal bypass was treated by explantation and prosthetic repair. One month later, he presented with acute right limb ischemia related to occlusion of the right limb of the stent graft despite anticoagulation which was treated by mechanical thrombectomy.
Conclusions
Vascular BD can worsen the vascular outcome after surgery. Except in an urgent context, BD must be controlled before surgery. This case report illustrates the importance of combined medical and surgical management, with first BD activity control with corticosteroids and immunosuppressive treatment, then surgical or endovascular treatment.
Introduction
Behçet’s disease (BD) is an inflammatory disease that may present with vascular involvement of vessels of all sizes. 1 It is a heterogenous disease with chronic inflammatory condition and well-known clinical features of oral and genital ulcers, uveitis but also gastrointestinal, skin, and joint symptoms. Both genders are affected at roughly equal rates, but disease tends to be more severe for males. 2 There is no specific biological parameter to diagnose BD; during the acute phase, markers are usually moderately high, except where there is major organ or systemic involvement.
The occurrence of large vessel involvement in BD is 7 to 38% and includes arterial and venous vasculitis with development of aneurysm (75%) and thrombosis (24.4%). Veins are usually more affected than arteries and superficial thrombophlebitis and deep vein thrombosis are the most common forms. Patients with previous episode of venous thrombosis might develop arterial involvement during follow-up. 3 BD affects superficial vein (55.3%), deep vein (29.8%), and the aorta and large arteries (3.6%). In arterial involvement, aneurysms are commonly seen rather than occlusive lesions. In a recent series, 10.2% of 441 BD patients had aneurysms. 3 The distribution of involved arteries was 33.3% abdominal aorta, 30.8% pulmonary arteries, 25.6% iliac arteries, 12.8% femoral arteries, and 10.3% thoracic aorta; 38.5% of the aneurysms were saccular.
Case presentation
A 41-year-old man was admitted for right leg pain. His only cardiovascular risk factor was active smoking. He had extensive BD, diagnosed at the age of 26, with history of deep vein thrombosis, cerebral vein thrombosis, pulmonary embolisms and multiple arterial aneurysms. Seven years earlier, he presented with rupture of a right popliteal artery aneurysm (41 mm, Figure 1(a)), treated emergently by a reverse venous femoro-popliteal bypass with cephalic vein (saphenous veins were pathologic). CT angiography: (a) sagittal cross-section of popliteal aneurysm, (b) sagittal cross-section of right femoral bypass aneurysm; (c) coronal section of left common iliac saccular aneurysm and abdominal aortic aneurysm.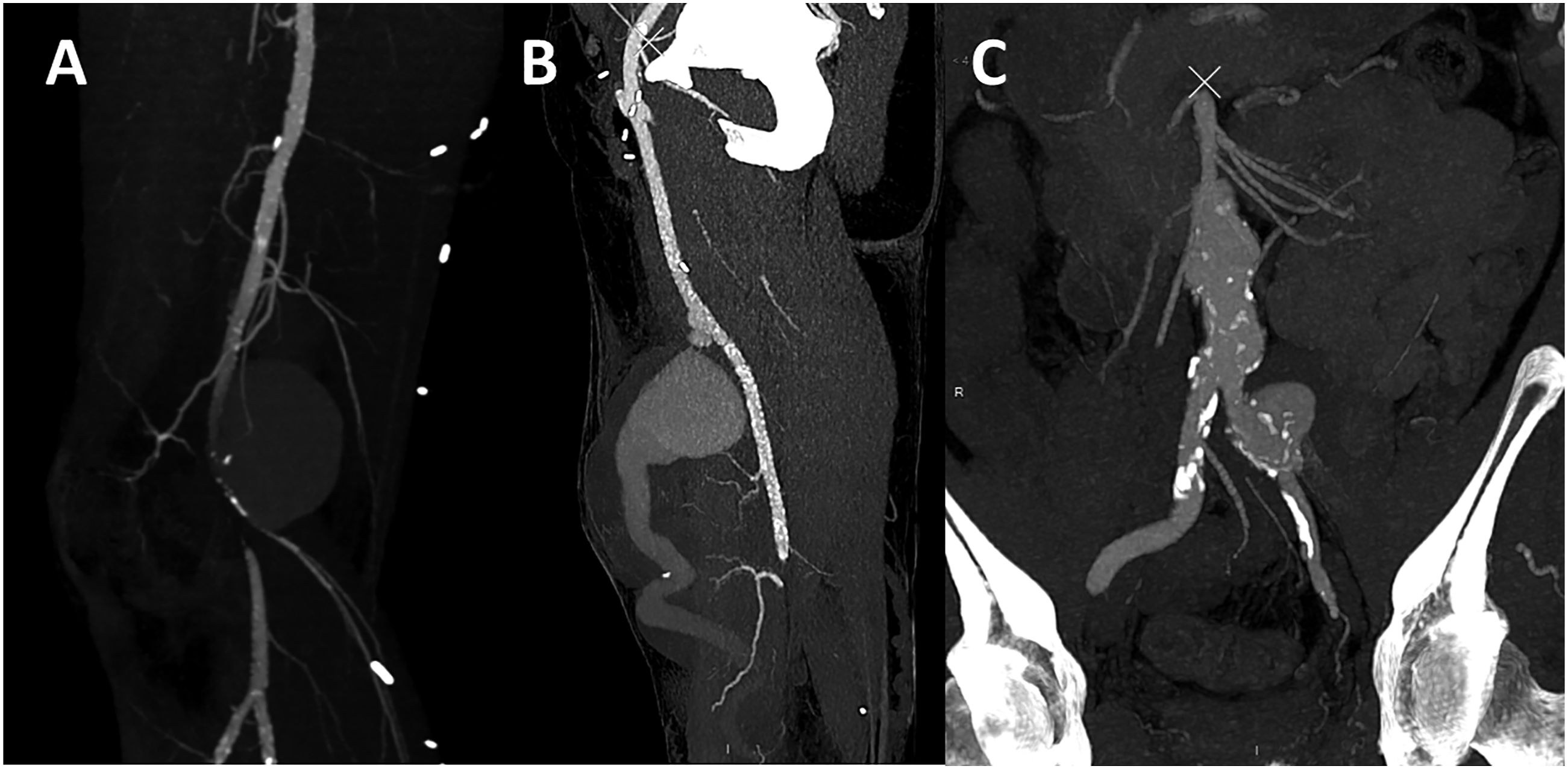
Then, his medical follow-up was sporadic and his medical treatment on admission was aspirin and wafarin. Steroids and immunosuppressive (IS) (azathioprine, cyclophosphamide) had been stopped for 4 years.
On examination, the right ankle-brachial index was 0.45 with occlusion of the anterior tibial artery. On imaging, multiple aneurysms were diagnosed, including a distal 87 mm aneurysm of the femoro-popliteal venous bypass (Figures 1(b) and 2), a small abdominal aortic aneurysm and a left common iliac artery aneurysm (33 mm) (Figures 1(c) and 2). There was no evidence of infection. He was in an acute phase of his disease with elevated C-reactive protein (CRP: 210 mg/L) and contrast enhancement of the aneurysm wall on CT was in favor of extensive parietal inflammation. He first underwent an intensification of his medical treatment with methylprednisolone and infliximab intravenous infusion that allowed CRP normalization (5 mg/L). Three months later, due to the risk of arterial rupture, the left iliac artery aneurysm was treated with a bifurcated infrarenal stent graft implantation, then the aneurysm of the venous bypass was treated by removal and PTFE prosthetic repair. The choice of endovascular repair strategy was made in order to limit vascular incisions that can trigger a relapse of BD, and also to limit the risk of locoregional infection in this highly immunocompromised patient. Moreover, the patient had no vein conduit available to perform a venous bypass. The anatomy was favorable for an endovascular repair, with long and healthy proximal and distal sealing zones. The oversizing of the stent graft was 15%, to reduce the risk of excessive oversizing and wall enlargement. Volume-rendered reconstruction CT angiography with right femoral bypass aneurysm and irregular-shaped saccular aneurysm left common iliac artery.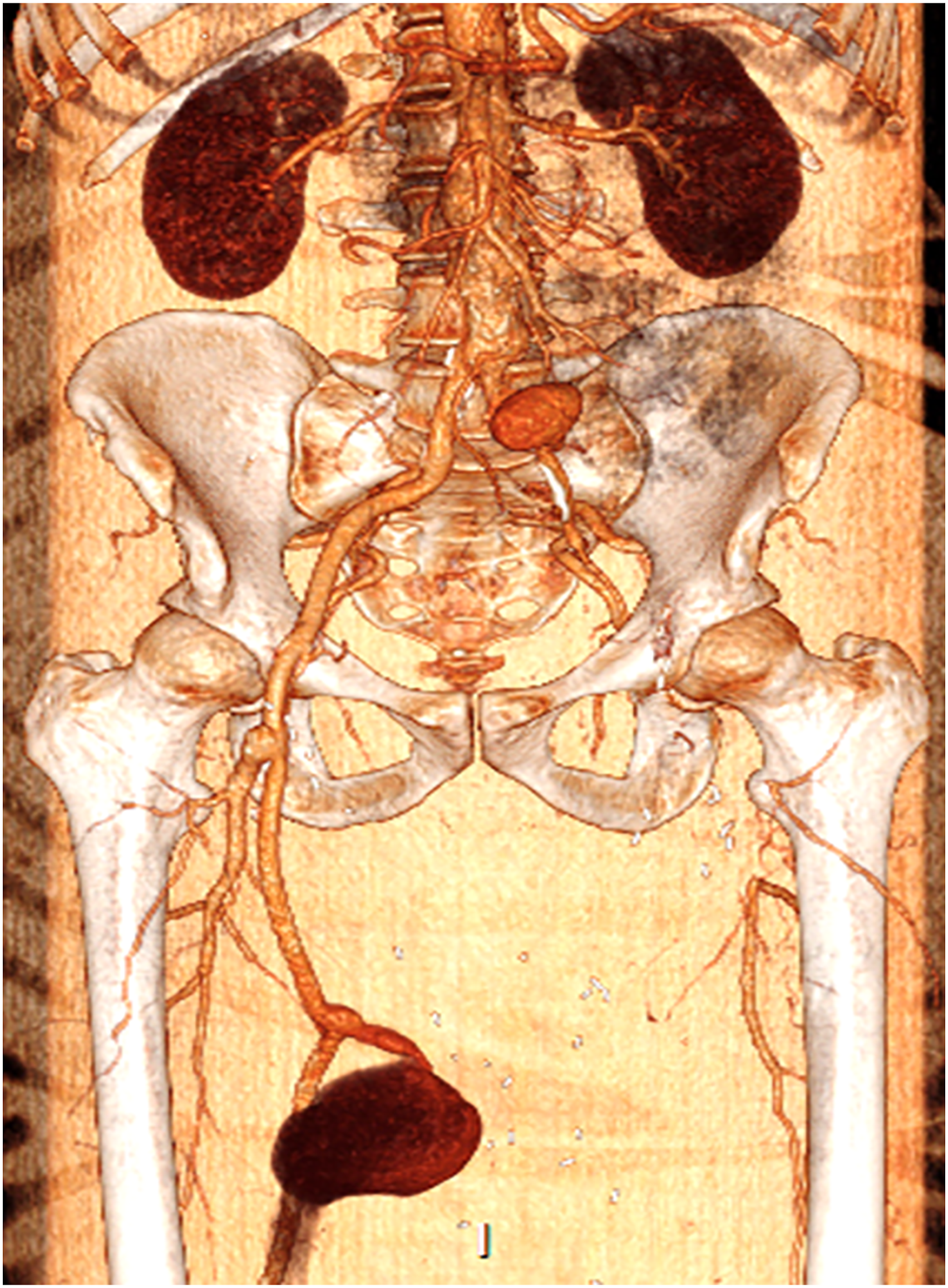
Warfarin was replaced by tinzaparin, aspirin was increased from 75 to 160 mg/d and perindopril was increased to 8 mg/d. One month after the surgery, despite anticoagulation, he presented with acute right limb ischemia related to a right distal bypass anastomosis thrombosis treated by thrombectomy.
Unfortunately, he developed a femoro-popliteal bypass graft infection, and 3 weeks later, had a rupture of the distal anastomosis which was treated by antibiotics and redo surgery with prosthetic graft. Rupture was likely secondary to a combination of infection and compromise of the tissues from long-term steroid therapy. A few weeks after the surgery, local evolution was unfavorable with severe skin infection and arterial occlusion due to aneurysmal degeneration of the distal anastomosis likely from infection. It required a below-the-knee amputation.
Discussion
The vascular surgeon should consider BD when the patient has arterial aneurysms and a history of oral or genital aphtha’s ulcers, when arterial and venous aneurysms are present or in the case of multiple aneurysms in a young patient. This case shows a very rare arterial BD complication with multiple concomitant arterial aneurysms and surgical complications in active BD. It is a rare condition and only up to 18% patients may develop arterial lesions that require surgical intervention. 4 BD aneurysms are saccular and present a high risk of rupture, without correlation with aneurysm size. The pathophysiology of aneurysm formation is different than in degenerative atherosclerotic disease. 5 Except in case of life or limb threatening condition, BD control must be obtained prior to surgery in order to reduced surgical complications, infection or BD post-operative flare-up. Recent recommendations have standardized Behcet’s peri-operative treatment with IS adaptation to minimize the recurrence at surgical site (post-operative complication rate decrease significantly with treatment versus none, RR 0.08) and decreased flare-up risk. 6 For the management of arterial aneurysms, high-dose glucocorticoids and cyclophosphamide are recommended.1,7 In patients with refractory or relapsing arterial involvement, anti-TNF agents may be helpful.1,7 The IS are essential to control vasculitis and prevent recurrence and growth of arterial aneurysms in order to avoid surgical procedures.
Many cohorts have reported that on medical therapy’s impact on recurrence. Shen et al. 8 compared endovascular and open surgery in BD and reported only pre-operative IS was a significant factor to reduce the risk of aneurysm recurrence. The choice for the repair (endovascular or open surgery) did not influence the long-term prognosis. Fei et al. 9 showed in a cohort of 796 patients, the importance of medical treatments, including aspirin and corticosteroid, on improvement in all BD patients before surgery and do not perform a surgery in vasculitis active phase because of the high risk of post-surgical arterial complications such as pseudoaneurysm.
Regarding the technical repair, the choice depends on aneurysm location. For aorto-iliac location, an aorto-bi-iliac bypass was the preferred surgical repair. 10 Besides, great saphenous vein has been reported to be ideal for repairing arterial lesions in arteries of small to medium diameter. 4
Concerning complications, a retrospective study of 33 BD patients, 4 with a follow-up of almost 4 years, showed that saccular aneurysm rate was lower with stent grafts than synthetic or saphenous vein bypasses (none in endograft group, versus 20% in saphenous vein and 38% in synthetic group).
Conclusion
This case reports rare multiple aneurysmal complications in BD. It underscores the utmost importance of combined medical and surgical management, with primary BD activity control with corticosteroids and immunosuppressant, then open or endovascular surgical treatment.
Footnotes
Author contributions
JS and OE: study concept and design, data collection, drafting of the manuscript, and supervision; BM data collection and critical review; all the authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient consent
The patient provided written consent
Ethical approval
This study has been conducted in compliance with the Declaration of Helsinki principles