
Abstract
Objective
To analyze the feasibility and results of up-and-over access (UOA) for catheter-directed thrombolysis (CDT) in acute iliofemoral popliteal venous thrombosis (IFPVT).
Methods
From June 2020 to June 2021, a total of 26 patients (26 lower limbs) undergoing CDT for IFPVT were included. According to the vascular access, the patients were divided into UOA group (n = 11, 10 left limbs and 1 right limb) and ipsilateral popliteal vein (ILPV) (n = 15, 15 left limbs) access group. The differences in preoperative characteristics and technical details between the two groups were compared.
Results
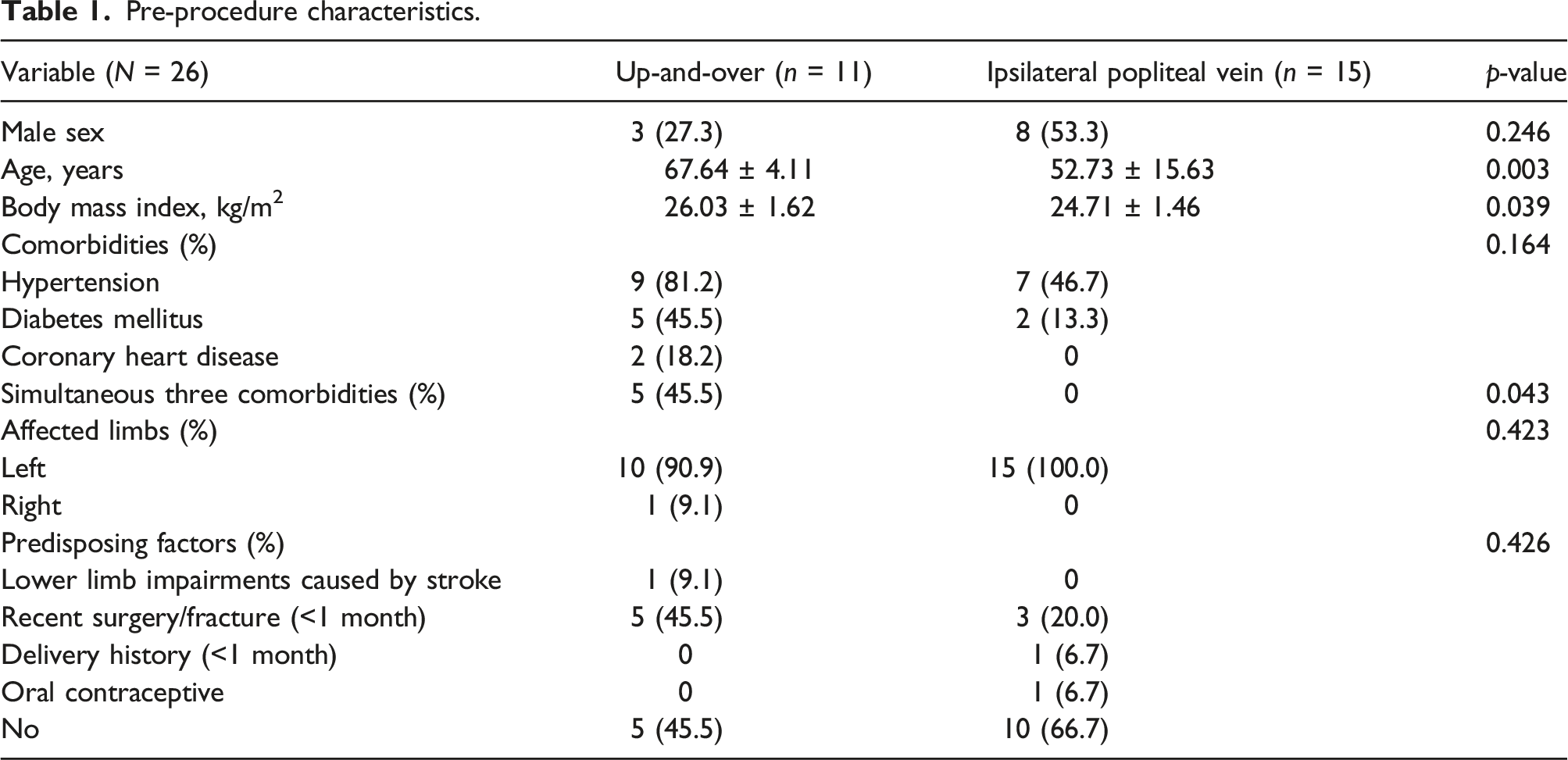
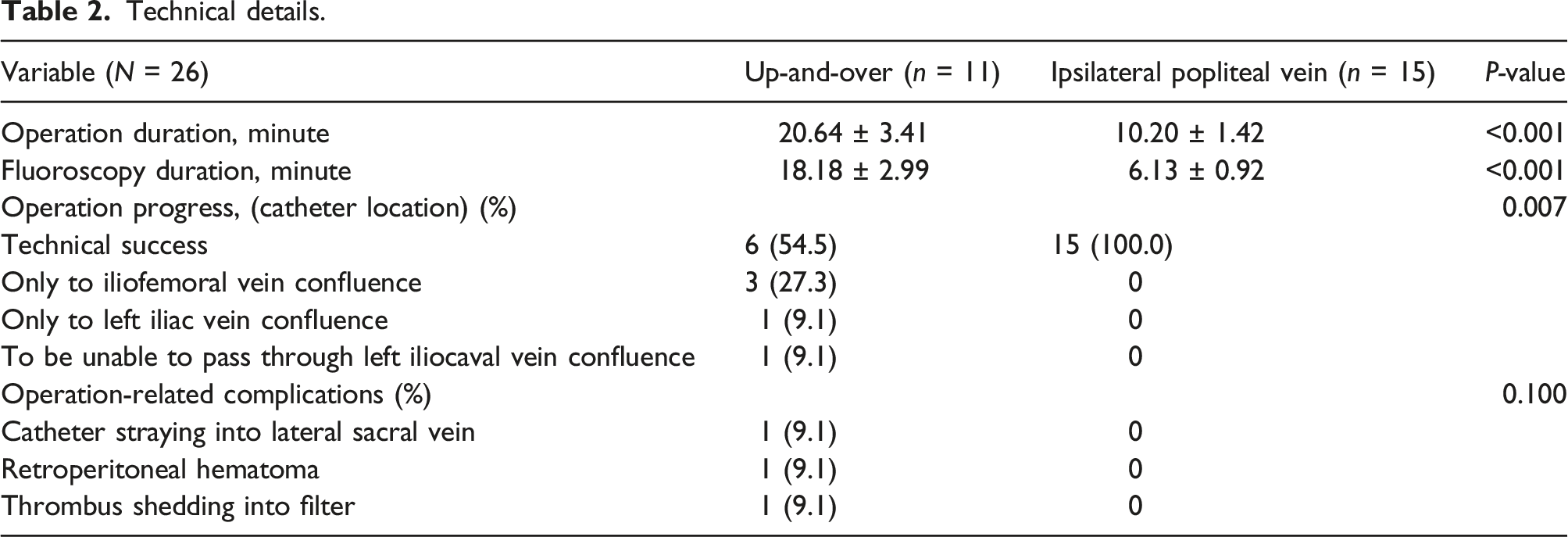
Patients in UOA group were older than those in ILPV access group (67.64 ± 4.11 years VS. 52.73 ± 15.63 years, p = .003). The BMI of UOA group was significantly higher than that of ILPV access group (26.03 ± 1.62 kg/m2 VS 24.71 ± 1.46 kg/m2, p = .039). There were significantly more patients with simultaneous three comorbidities in UOA group than in ILPV access group (45.5% vs. 0, p = .043). Compared with ILPV access group, the duration of operation and fluoroscopy of UOA group were significantly longer (20.64 ± 3.41 min vs. 10.20 ± 1.42 min, p < .001; 18.18 ± 2.99 min vs. 6.13 ± 0.92 min, p < .001), but the technical success rate was significantly lower (54.5% vs. 100%, p = .007). In UOA group, the operation-related complications occurred, including catheter straying into lateral sacral vein (9.1%), retroperitoneal hematoma (9.1%), and thrombus shedding into filter (9.1%).
Conclusion
The UOA may be attempted in patients who are unable to be prone, but this access is not an optimal pathway for CDT.
Introduction
Acute iliofemoral popliteal venous thrombosis (IFPVT) may easily lead to post-thrombosis syndrome (PTS) in the long term if the thrombus is not removed in time or there is still residual thrombus after removal.1,2 Early removal of thrombus may significantly reduce the severity of PTS.3–5 At present, percutaneous catheter-directed thrombolysis (CDT) is still very important method for early thrombus removal.6,7 The ipsilateral popliteal vein (ILPV) access of the affected limb in prone position is often used in the vascular access of CDT.3,5,8–10 However, it is difficult to perform CDT through ILPV access in patients who are unable to maintain prone position. Thus, the application of up-and-over access (UOA) to CDT has been reported.11,12 Nevertheless, the pros and cons of the technical details of UOA have not been reported.
Consequently, in this study, we sought to compare the results of technical details of ipsilateral popliteal access and contralateral up-and-over access for the management of iliofemoral popliteal acute deep venous thrombosis.
Methods
Patients
From June 2020 to June 2021, a total of 26 patients undergoing CDT for IFPVT were included in this study. Acute IFPVT was confirmed by symptom duration of less than 2 weeks, Doppler ultrasonography (DUS), and D-Dimer level. The extent of thrombus involvement was verified simultaneously by using DUS and digital subtraction angiography (DSA). According to the vascular access, the patients were divided into UOA group and ILPV access group. The need for informed consent to be included in this study was waived given the retrospective and anonymized nature of the data collection process.
Procedures
Noninvasive blood pressure monitoring of upper arm cuff was performed during the procedure. If the intraoperative blood pressure was too high, it would be adjusted to about 140/90 mmHg, and then CDT would be performed. Heparinization was performed by intravenous injection of unfractionated heparin (100 U/kg) throughout the operation. All patients underwent retrievable inferior vena cava filter placement (Denali, Bard Peripheral Vascular, Inc.) through the healthy contralateral femoral vein access before CDT. All the filters were successfully removed within 3 months after placement
Up-and-over access group
Patients who were unable to perform prone movements, such as advanced age or limited physical mobility, or who were unable to accept the prone position, were preferentially considered for UOA approach. The patients were in the supine position. After successful placement of filter, the filter delivery introducer sheath (8.4 Fr–55 cm) was replaced with an 8 Fr–10 cm introducer sheath (Terumo Corp.). Under the guidance of road map, a 5 Fr Cobra catheter or vertebral artery catheter was introduced into the lower segment of inferior vena cava with a 0.035 inch–150 cm Radiofocus angled soft hydrophilic guidewire (Terumo Corp.), and then selected to enter into the iliofemoral popliteal vein of the affected limb. Then, after replacing with a 0.035 inch–260 cm Radiofocus angled stiff hydrophilic guidewire (Terumo Corp.) and withdrawing the angiographic catheter, a 30 cm or 40 cm-length Uni-fuse catheter (Angiodynamics, Inc.) was introduced into the iliofemoral popliteal vein of the affected limb. When the angiographic catheter could only be advanced to the iliofemoral vein confluence or left iliac vein confluence, a 20 cm or 10 cm-length Uni-fuse catheter was introduced.
Ipsilateral popliteal vein access group
The patients were in the prone position. The popliteal vein was punctured anterogradely at the popliteal fossa of the affected limb and a 5 Fr introducer sheath (Terumo Corp.) was placed. Then, a 5 Fr vertebral artery catheter accompanied by a 0.035 inch-150 cm Radiofocus soft guidewire was sent to the inferior vena cava through the femoral iliac vein. In the same procedure as above, a 30 cm or 40 cm-length Uni-fuse catheter was introduced.
Technical success was defined as the complete coverage of iliofemoral venous thrombosis by the Uni-fuse catheter.
Statistical analysis
Continuous variables were reported as mean ± standard deviation and evaluated using two independent samples t-test or separate variance estimation t-test according to Levene’s test for equality of variances. Categorical variables were expressed as percentages and evaluated using Fisher’s exact test. Statistical significance was accepted with a p < .05. All analyses were conducted with SPSS v25.0 software (SPSS Inc, IBM Company).
Results
Study patients
Pre-procedure characteristics.
Technical details
Technical details.
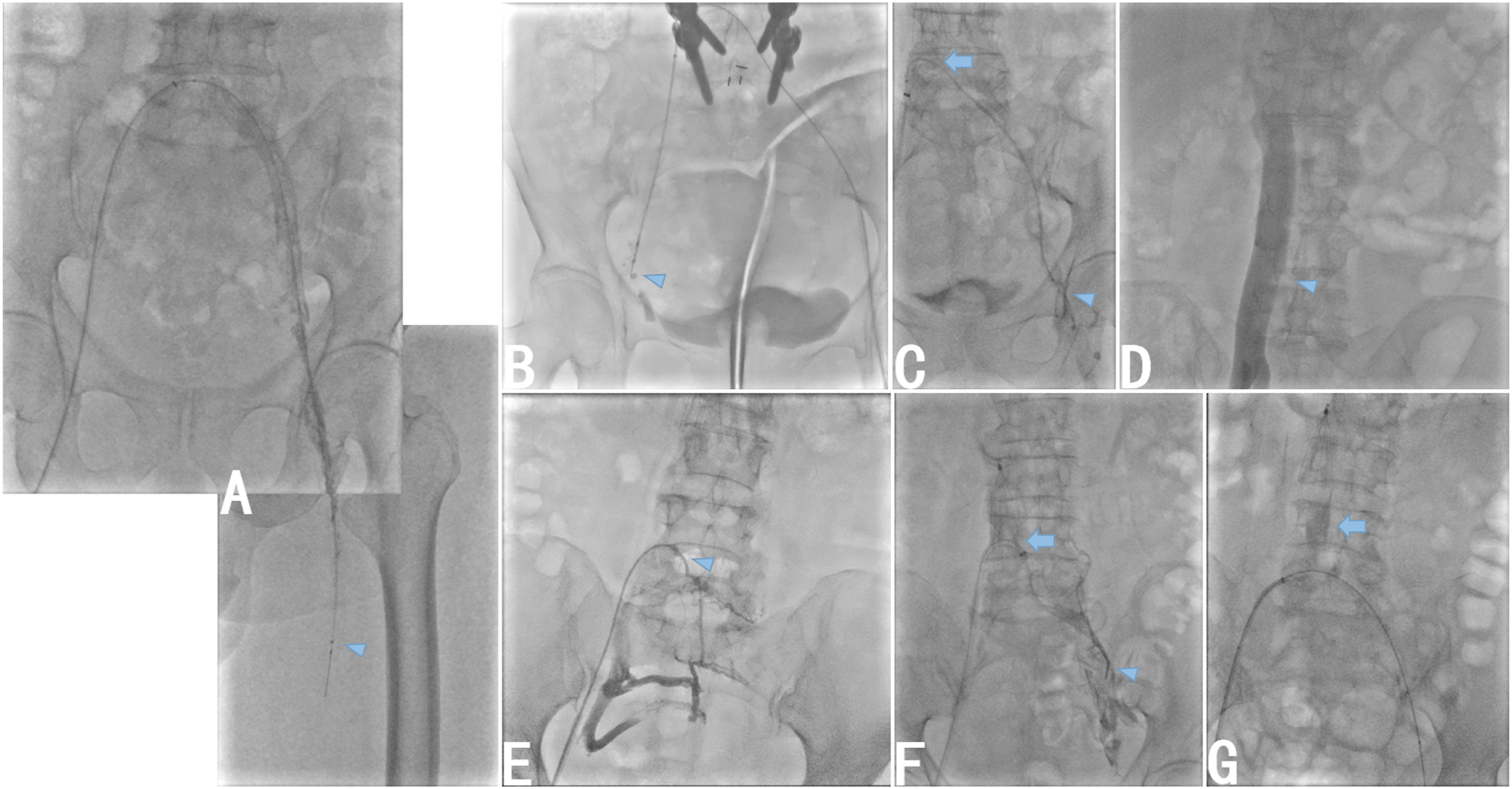
Up-and-over access A. A 30 cm-length Uni-fuse catheter was successfully introduced into iliofemoral vein segment. B. A 10 cm-length Uni-fuse catheter was only advanced to the right iliofemoral vein confluence. C. A 20 cm-length Uni-fuse catheter could not follow-up synchronously with the stiff guidewire, and the distal segment of the catheter looped into the inferior vena cava. D. The left iliocaval vein confluence had no notch during angiography, which a catheter could not enter into. E. A catheter strayed into lateral sacral vein. F. A catheter was only advanced to the left iliac vein confluence and the distal segment of catheter was in contact with the filter. G. Retroperitoneal hematoma occurred (contrast agent retention).
Discussion
Rapid thrombus removal may prevent the progression of acute IFPVT to severe PTS, which has become one of the effective treatment schemes for acute IFPVT.3,13 Although there are many methods for rapid thrombus removal, such as Aspirex®S and AngioJet system, CDT still plays an indispensable role in the treatment of acute IFPVT.14,15 The popliteal vein access of the affected limb has become the classic access for CDT.10,11,16,17 Additionally, the application of UOA for CDT has been occasionally reported.11,12,16 Nevertheless, the difficulties that may be encountered in the operation of UOA have not been reported. In this work, the duration of operation and fluoroscopy of UOA group were significantly longer than those in ILPV access group, whereas the technical success was only 54.5%. This indicates that UOA may not be the optimal pathway for CDT.
Moreover, majority previous studies using UOA for CDT did not explain the indications of this access. Qian C and colleagues reported that patients who could not be converted to a prone position or who had suspected thrombus in popliteal vein selected an UOA for CDT. 16 Similarly, in this work, the age, BMI, and the number of comorbidities of patients in UOA group were significantly higher than those in ILPV access group. It revealed that the physical condition of the patients in UOA group was relatively poor. Therefore, we believed that if patients did not accept or tolerate prone position, an UOA might be selected.
Nonetheless, unlike the up-and-over technique for lower limb arteries,18,19 the same operation for lower limb veins was unsuccessful due to resistance in the iliac vein lumen. This study showed that in 45.5% of cases, the catheter could not advance to the femoral popliteal vein segment with UOA. During our operation, the Radiofocus soft guidewire in some cases could not pass through the iliofemoral vein confluence or left iliac vein confluence. In other cases, although the Radiofocus soft guidewire passed through the two segments, the catheter could not follow-up synchronously. Even if the Radiofocus soft guidewire was replaced with a stiff guidewire, the catheter still could not move forward. If the catheter was pushed forward by force, the distal segment of the catheter formed a loop at iliocaval vein segment and then contacted with the inferior vena cava filter just placed. This suggests that CDT may not be performed in these cases. Even when a Uni-fuse catheter was placed, it did not cover the entire venous thrombus segment. Additionally, operation-related complications, such as catheter straying into collateral branches, retroperitoneal hematoma, and thrombus shedding, occurred. Up to now, there are no data in the literature to analyze the cause of these problems. We believe that fresh thrombus in the vascular lumen was not the main reason for hindering the advancement of the catheter or guidewire. Jayaraj A and Raju S reported the analysis of nonthrombotic iliac vein lesions (NIVL) by intravascular ultrasound, that is to say, NIVL lesions are typically subsegmental and focal, occurring in areas where compression by the overlying artery or ligament occurs. 20 Specifically, the classic proximal NIVL lesion occurs in the left common iliac vein posterior to where it is crossed by the right common iliac artery; the distal lesion on the left side occurs posterior to the left hypogastric artery crossing; on the right side, both proximal and distal lesions underlie the right common iliac artery; compression by the inguinal ligament is also a source of stenosis. 20 Therefore, the forward resistance of catheter may be closely related to the anatomical characteristics of external pressure of the iliac vein. On the other hand, LePage PA and colleagues found valvular structures in the common iliac vein in 1.2% of the population and the external iliac vein in 26.2% of the population at autopsy. This may also be one of the reasons why the catheter cannot move forward. 21 Thus, we speculate that based on the above anatomical characteristics of iliac vein, acute iliofemoral vein thrombosis caused inflammatory swelling of the vascular wall, which may aggravate the stenosis of the lumen. So, the forward resistance of catheter was significant.
However, in this work, the technical success rate in ILPV access group was 100%. According to our operating experience, the Radiofocus soft guidewire and catheter in ILPV access group had low resistance in moving forward in iliofemoral vein. This cannot be explained by the above anatomical characteristics of iliac vein compression. Another explanation is that in ILPV access group, the force pushing the catheter forward was in the linear direction with the catheter, whereas in UOA group, the catheter formed an angle after entering into the iliocaval vein confluence, so that the force could not be fully transmitted to the tip of the catheter.
Once the UOA fails, other accesses can be selected to perform CDT. Some accesses in the supine position, including jugular or below the knee vein access, have been reported.16,17,22,23 In the real world, several patients became more nervous and fatigued after long-time up-and-over operation and voluntarily gave up further CDT treatment.
Limitations
There are several limitations in our work. First, this is a retrospective study. Because the choice of access for CDT was based on the patient’s physical condition or willingness, it was difficult to conduct prospective research. Second, the sample size of this study is small, which may not fully reflect the advantages and disadvantages of UOA. Due to the low technical success rate of UOA, we did not routinely use this access for CDT. This is the reason for the low sample size in this study.
Conclusion
When using CDT for acute IFPVT, the UOA may be attempted in patients who are unable to be prone, but this access is not an optimal pathway for CDT.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.