
Abstract
Objective
The purpose of our study was to describe perioperative kinetics of procalcitonin (PCT) in patients undergoing aortic surgery, to compare the kinetics in the open abdominal aortic aneurysm (AAA) repair and aortobifemoral bypass for aortoiliac occlusive disease (AIOD), and to evaluate the ability of PCT to detect intestinal ischaemia.
Methods
A prospective non-randomized observational cohort study in 80 patients (62 men and 18 women) undergoing elective aortic surgery was performed. Serum PCT was measured at baseline and defined intraoperative and postoperative timepoints up to postoperative day 7. MRI contrast-enhanced imaging was used to detect intestinal ischaemia.
Results
The comparison of the AAA and AIOD cohort did not show any significant difference in PCT levels. Patients with intestinal ischaemia had higher serum PCT at multiple timepoints postoperatively. The most accurate timepoints for early diagnosis were postoperative day 3, followed by 24 h after declamping of the vascular reconstruction, and postoperative day 7. The sensitivity and negative predictive values were 100% in all mentioned timepoints. However, event at the best timepoint the specificity was 89% and the positive predictive value 43%.
Conclusions
Procalcitonin levels in the postoperative period at proper timepoints might help to detect postoperative intestinal ischaemia. The limitation of this marker is its low specificity for intestinal ischaemia and low positive predictive value. The highest value of this marker is that it can rule out this complication because normal PCT levels mean that intestinal ischaemia is very unlikely.
Keywords
Introduction
Intestinal ischaemia is a well-known complication of abdominal aortic vascular surgery. The reported incidence of intestinal ischaemia in elective open abdominal aortic procedures ranges between 1% and 7% and rises to 5% to 9% if routine postoperative colonoscopy is performed.1,2 The mortality of this condition exceeds 50%. 3 The left colon is usually affected, but any part of the intestine might be involved. At present, we have no specific laboratory marker for the early detection of postoperative intestinal ischaemia.
Many new markers have been discussed lately, one of them being procalcitonin. 4 Procalcitonin (PCT) is a 116-amino acid precursor of calcitonin normally released by the C cells of the thyroid gland. In sepsis or other pathological conditions, multiple organs and tissues are involved in PCT production, and in a broader sense, the entire body becomes a calcitonin precursor producing endocrine gland. 5 Currently available data from experimental and clinical studies focussing on PCT as a marker of intestinal ischaemia show sensitivity, specificity and positive and negative values ranging between 72% and 100%; 68% and 91%; 27% and 90%; and 81% and 100%, respectively. 6 The majority of studies evaluate PCT levels in one or multiple timepoints without a precise relation to primary insult. Only a couple of studies used defined timepoints in animals or humans.7–11 Our knowledge of the perioperative kinetics of PCT is limited. The physiological value of PCT should be lower than 0.5 mg/L but the cut-off value indicative of intestinal ischaemia is unknown. 12
The purpose of our study was to describe intraoperative and postoperative kinetics of PCT in patients undergoing aortic surgery, to compare the kinetics of PCT in the open abdominal aortic aneurysm (AAA) repair and aortobifemoral bypass for aortoiliac occlusive disease (AIOD) and to evaluate the ability of PCT to detect intestinal ischaemia in the postoperative period. We hypothesized that PCT kinetics might differ in AAA and AIOD cohorts, PCT levels will be higher in cases of intestinal ischaemia, and the time relation to surgery will lead to differences in marker accuracy. This study was a part of a grant project focussing on multiple markers of mesenteric ischaemia.
Methods
Patients
We performed a prospective non-randomized observational cohort study on 80 patients being operated on between November 2017 and September 2020 in our department. The mean age of patients was 68.0 ± 8.4 years; 62 patients were men and 18 were women. The study was consecutively offered to all patients scheduled for elective aortic surgery for AAA or AIOD fulfilling the inclusion criteria to enrol 50 AAA patients and 30 AIOD patients. In the AAA group, we offered the study to patients where aneurysmatic or atherosclerotic disease affecting iliac arteries implied the need to construct at least one distal anastomosis on the femoral artery in the groin. The reason was to achieve a similar extent of operative trauma. In the AIOD group, we offered the study to patients with lifestyle-limiting intermittent claudication only (Rutherford classification 1–3) to exclude the potential influence of critical limb-threatening ischaemia on marker levels. The exclusion criterion was a contraindication for magnetic resonance imaging (MRI). The study protocol was approved by the Ethical Committee of St. Anne’s University Hospital Brno, ref. number 3 G/2017 and all patients were enrolled after they signed informed consent. The overall acceptance rate was 37% (80 of 216 patients offered to participate). Thirty-three percent of patients refused to participate in the study because they already felt the stress of an extensive aortic procedure and didn’t agree with any additional lab tests or imaging. Eight percent gave the fear of MRI imaging as a reason for refusal, three percent claimed that they had claustrophobia and nineteen percent didn’t want to participate in any research study.
Surgical technique
Both, open AAA repair and aortobifemoral bypass in AIOD patients were performed without any specific study modification. Procedures were conducted under general anaesthesia and the aorta was exposed using a transperitoneal approach through a midline laparotomy. The aneurysm was replaced using Dacron graft (Ra bv K graft, VUP Medical, Czech Republic) with the proximal anastomosis in an end-to-end fashion. We perform inferior mesenteric artery reimplantation in case of intraoperative colonic ischaemia, presence of large dominant inferior mesenteric artery, bilateral internal iliac occlusion and prior colon surgery. The decision was on the operating surgeon. The inferior mesenteric artery in the AAA group was ligated in all cases. Distal anastomoses were performed in end-to-end fashion to the iliac artery and end-to-side fashion to the common femoral artery (26%) or in an end-to-side fashion to both common femoral arteries (74%). We used the same Dacron graft for aortobifemoral bypasses. In aortoiliac occlusive disease, we prefer the end-to-side proximal anastomosis (93%) but in two cases we performed end-to-end anastomosis (7%). The inferior mesenteric artery was ligated just in one case where the proximal end-to-end anastomosis was performed. In all other AIOD cases, we preserved the artery. Distal anastomoses to femoral arteries were in all cases performed in an end-to-side fashion.
Sample collection and PCT measurement
We have collected eight venous blood samples from the central venous line per patient. The timing of sample collection was as follows. One hour before surgery, we collected sample S-BL (timepoint BL, BaseLine). Two samples were collected during the procedure. Sample S-CL1H was taken 1 hour after aortic cross-clamping or just immediately before the complete declamping of vascular reconstruction, which came sooner (timepoint CL1H, CLamping 1 Hour). Sample S-DC10M was collected 10 min after complete declamping of vascular reconstruction (timepoint DC10M, DeClamping 10 Minutes). The postoperative samples S-DC3H, S-DC6H and S-DC24H were taken 3 h, 6 h and 24 h after complete declamping (timepoints DC3H, DeClamping 3 Hours; DC6H, DeClamping 6 Hours; and DC24H, DeClamping 24 Hours), respectively. Samples S-POD3 and S-POD7 were collected on postoperative days 3 and 7 at 7 a.m. (timepoints POD3, PostOperative Day 3; and POD7, PostOperative Day 7). The samples were immediately processed and PCT levels were analysed using electrochemiluminescence immunoassay (Elecsys BRAHMS PCT, Roche).
MRI imaging
MRI sequences used in the study.
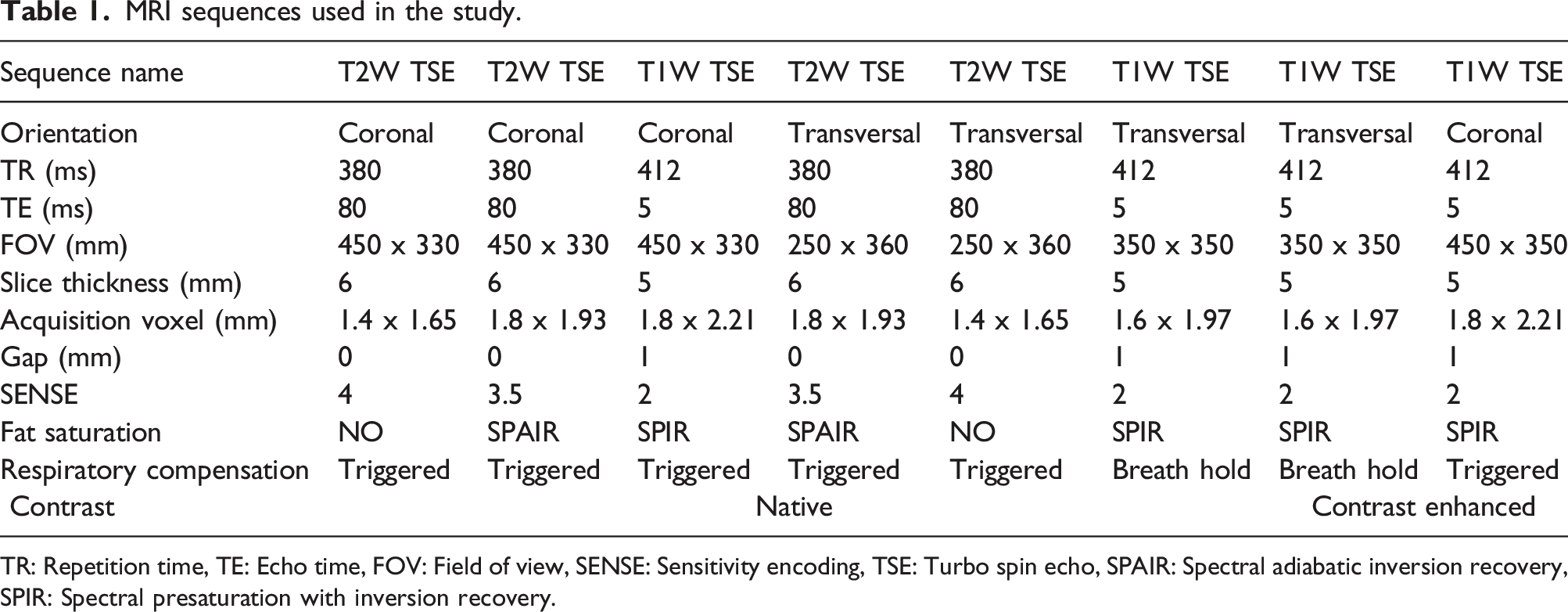
TR: Repetition time, TE: Echo time, FOV: Field of view, SENSE: Sensitivity encoding, TSE: Turbo spin echo, SPAIR: Spectral adiabatic inversion recovery, SPIR: Spectral presaturation with inversion recovery.
Intestinal ischaemia detection
The intestinal ischaemia was primarily diagnosed by MRI imaging (performed according to study protocol). The diagnosis might have been established before MRI by other methods (CT imaging, surgical procedure) if they had been performed sooner in the postoperative course based on the clinician’s decision. This happened twice in the study. In one case the complication was detected by the computed-tomography imaging performed before the planned MRI, and in one case by the surgical exploration (transmural ischaemia leading to peritonitis).
Data analysis
All data analyzes were performed in R. 14 Univariate analyses were performed using the Fisher exact test for qualitative variables and logistic regression models for continuous predictors. Spearman correlation coefficient was applied for pairs of continuous variables. ROC (receiver operating characteristic) curves were applied for threshold identification. Statistical significance was set at level alpha = 0.05.
Results
Cohort description and comparison of AIOD and AAA group.
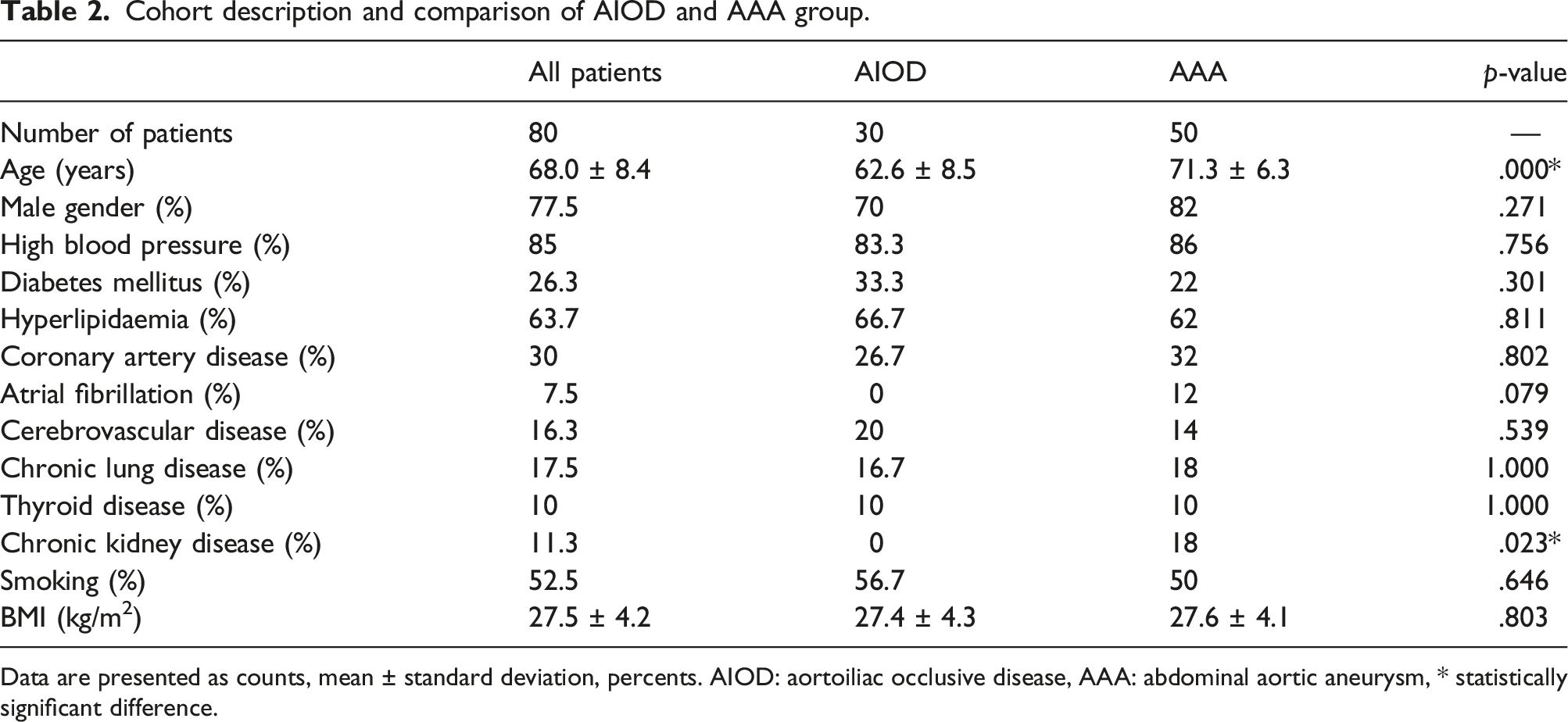
Data are presented as counts, mean ± standard deviation, percents. AIOD: aortoiliac occlusive disease, AAA: abdominal aortic aneurysm, * statistically significant difference.
The MRI imaging was performed in 79 patients (excluding the patient with transmural necrosis). The imaging was fully completed in 71 cases, the remaining eight MRI investigations were of lower quality or incomplete due to patients’ inability to cooperate in the postoperative period. All poor-quality or incomplete MRI examinations did not show any signs of intestinal ischaemia. We have decided to add up intestinal ultrasound in these patients, which was originally not a part of the study protocol. The results were normal in all cases. In one patient we performed postoperative computed tomography based on clinical suspicion of peripheral arterial embolism. This was not a part of the protocol and there were no signs of intestinal ischaemia. In the 30-day postoperative follow, no clinical signs of intestinal ischaemia developed in these eight patients.
The comparison of postoperative kinetics of PCT in AAA and AIOD groups gave no significant results. Therefore, we considered the whole cohort of all aortic surgery patients uniform for other analyses.
As already mentioned, there were two statistical differences in demographics between AIOD and AAA groups. We performed posthoc subanalyses to evaluate the influence of age and CKD on PCT levels in studied cohorts. Spearman correlation analysis for age gave a significant result for sample S-POD7 (p = .002). The older patients had higher PCT levels at this timepoint, but the absolute differences were negligible. The influence of CKD on PCT levels was significant in S-CL1H (p = .025). The absolute difference between averages was smaller than 0.02 ng/L.
Vessel patency, imaging, intraoperative findings and PCT positive timepoints in patients with intestinal ischaemia.
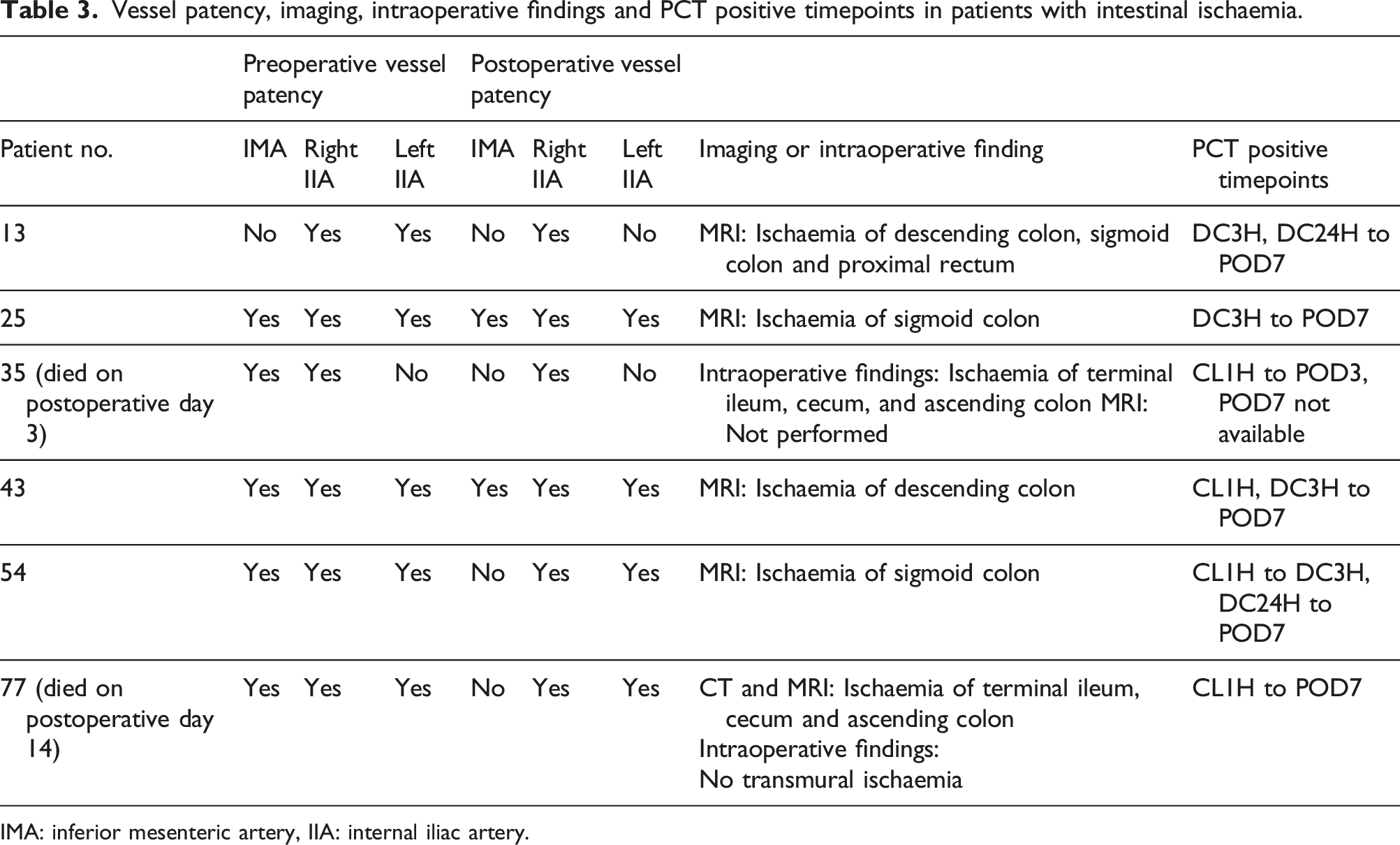
IMA: inferior mesenteric artery, IIA: internal iliac artery.
The differences in artery patency between patients with or without mesenteric ischaemia were not statistically significant. The celiac trunk was patent in all patients in both groups, there were three ostial stenoses, all in the non-ischaemic group. Similarly, the superior mesenteric artery was patent in all patients in both groups with three cases of ostial stenosis in the non-ischaemic group. No patient had both stenoses in our cohort. The inferior mesenteric artery was patent in 75.7% preoperatively and 31.1% postoperatively in the non-ischaemic group. In the ischaemic group, the preoperative and postoperative patencies were 83.3% and 33.3%, respectively. The internal iliac arteries were both patent in 85.1%, one occluded in 5.4% and both occluded in 9.5% preoperatively and both patent in 74.3%, one occluded in 9.5%, and both occluded in 16.2% postoperatively in the non-ischaemic group. The patients with mesenteric ischaemia had both internal iliac patent in 83.3% and one occluded in 16.7% preoperatively and both patent in 66.7% and one occluded in 33.3% postoperatively.
Finally, we have evaluated the ability of PCT to detect acute intestinal ischaemia. The univariate logistic regression comparing patients with and without intestinal ischaemia showed statistically significant differences between samples in multiple timepoints (Figure 1). Sample S-CL1H was the first statistically significant timepoint and S-DC10M was the most significant. Perioperative kinetics of procalcitonin in patients without (grey) and with (red) intestinal ischaemia. Statistically significant results marked with an asterisk.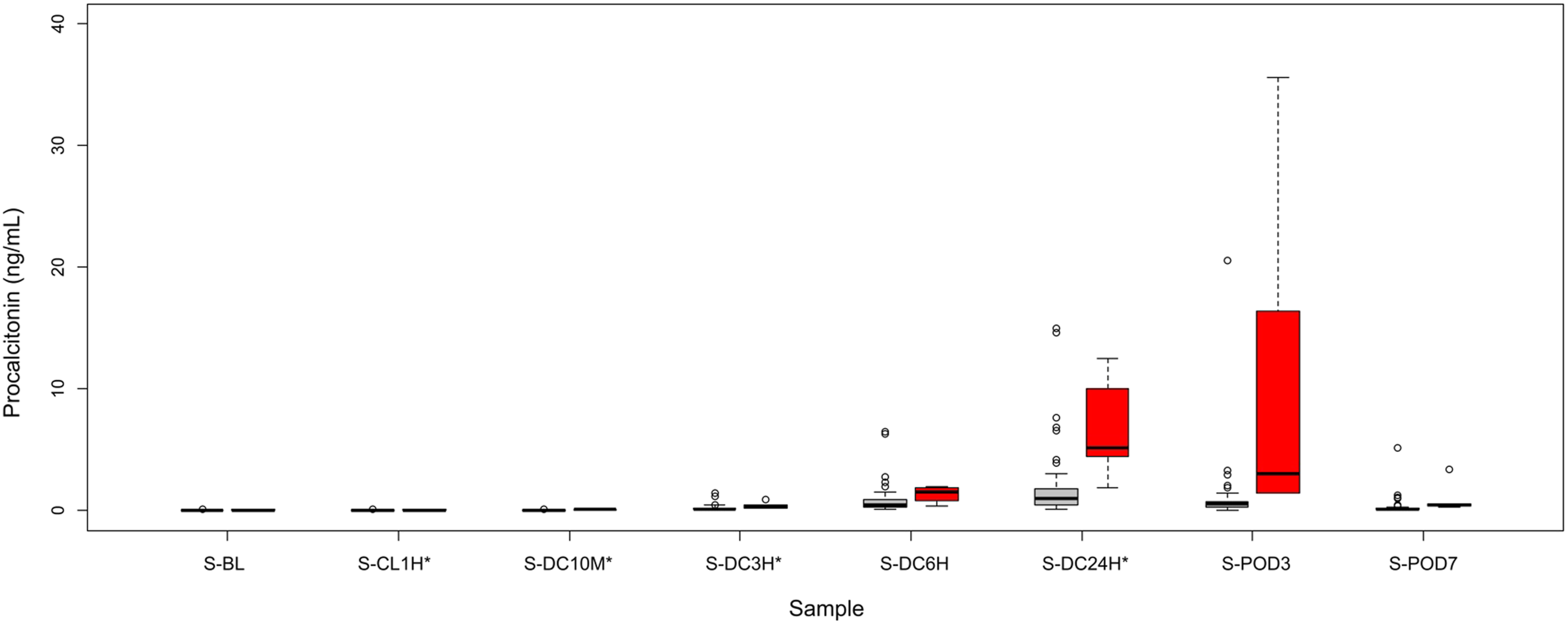
Receiver operating characteristic analysis of PCT levels for discrimination between groups with and without intestinal ischaemia in all.
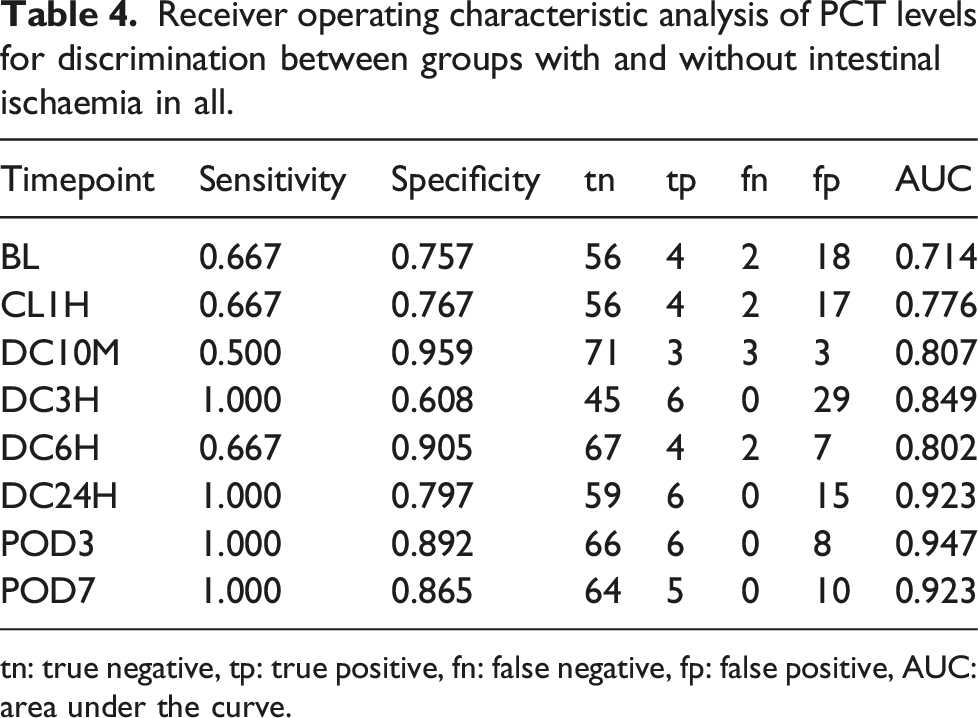
tn: true negative, tp: true positive, fn: false negative, fp: false positive, AUC: area under the curve.
Discussion
Postoperative intestinal ischaemia in elective aortic surgery is a rare but serious complication with high mortality. Early diagnosis is crucial for treatment, but its establishment based on clinical symptomatology and standard laboratory tests is very unreliable. The recommended imaging for the diagnosis of intestinal ischaemia is an abdominal CT with contrast. 15 In critically ill patients the imaging should be used judiciously because of possible adverse events during the transport and examination itself. 16 Colonoscopy or sigmoidoscopy is recommended for the final confirmation of colon ischaemia. 15 But they are not without the risk of complications. Therefore, there is an ongoing discussion on biomarkers and their potential to diagnose intestinal ischaemia.
Procalcitonin is one of the markers giving conflicting results in different types of studies focussing on intestinal ischaemia. This study evaluated postoperative kinetics of PCT at defined timepoints after aortic surgery. We have analysed two cohorts of aortic patients, where we might expect this complication.
The overall incidence of intestinal ischaemia was 7.5% and we were in the upper part of literally reported incidence. The incidence of intestinal ischaemia in the AIOD group seemed high as well. These numbers have led us to check the operative results of all aortic patients within the study timeframe. We have found that after the inclusion of patients who refused the study or did not fulfil inclusive criteria the incidence of intestinal ischaemia was lower. Considering the size of the cohort, the error on small numbers had at least a partial influence on the result. One of the two AIOD patients was asymptomatic and the diagnosis would be probably missed without imaging. The MRI imaging performed in study patients might have led to higher incidences similarly to routinely performed colonoscopy. 3
The use of MRI imaging for intestinal ischaemia detection performed in all but one patient of our cohort should be discussed as well. The most sensitive and specific method for the confirmation of colonic ischaemia is colonoscopy and it would be the most optimal method for the study. However, it is an invasive method with potential complications and during the study planning we performed a survey in our aortic patients and the majority of them were unwilling to participate if the colonoscopy would be a part of the study protocol. The study enrolment would be very slow and not feasible within the grant project timeframe. Therefore, we have decided to use noninvasive imaging. The recommended imaging for the diagnosis of colon ischaemia is CT with intravenous and oral contrast. 15 The meta-analysis of CT imaging of mesenteric ischaemia showed a pooled sensitivity of 93.3% and a pooled specificity of 95.9%. 17 The MRI imaging is not commonly used to diagnose intestinal ischaemia. Only a couple of studies compared MRI and CT imaging13,17,18 but the results support the adequacy of these two methods. We do not expect MRI to become the diagnostic tool in an acute setting. The price is higher, availability lower, the time of the imaging is substantially longer (leading to lower tolerance of examination) and the patient’s cooperation is needed. The quality of MRI and CT imaging is very similar, so there is no reason to switch from CT to MRI except in specific cases. The main reason for the choice of this modality in our study was not to expose the study subjects to unnecessary radiation.
The comparison of the AAA and AIOD groups, in the beginning, was a logical step as we know that there might be differences in PCT kinetics after various types of surgery.19,20 We did not find any significant differences between our study cohorts and the posthoc analyses focussing on age and CKD (the two factors significantly different in both cohorts) did not show any clinically relevant difference as well. The hypothesis of the difference of PCT kinetics between AAA and AIOD groups was rejected and so we consider the whole study uniform for further analyses.
The evaluation of the ability of PCT levels to help in the diagnosis of postoperative intestinal ischaemia was the main goal of our study. Two intraoperative timepoints were chosen based on animal studies as there are no data available on human subjects. The intraoperative PCT elevation is reported between 30 and 360 min after the onset of artificial ischaemia.8,21 The analysis showed statistically significant differences in both intraoperative timepoints but the absolute differences were negligible. We doubt the potential value of intraoperative PCT levels for the diagnosis of intestinal ischaemia.
In the postoperative period, we have assessed two early timepoints at 3 and 6 h after complete reconstruction declamping and three later timepoints at 24 h after declamping, and postoperative days 3 and 7. The choice of timepoints was based on available data on humans. Zogheib and colleagues used 0, 3 and 6 h and postoperative days 1 and 2 for their proposed PALM score estimating the risk of intestinal ischaemia. 22 Klingele and colleagues used baseline and postoperative day 1 samples, showing that PCT levels on a postoperative day 1 might help to diagnose non-occlusive mesenteric ischaemia. 23 Nagata and colleagues collected samples on postoperative days 1, 2 and 7, and found that the postoperative day 2 PCT levels were the most reliable for colonic ischaemia detection. 10
Statistical analysis showed significant differences in sample S-DC3H and S-DC24H. Sample S-DC3H with ROC analysis giving AUC 0.85 might be interesting. However, there was still a lot of false-positive results and the average difference in PCT levels was 0.23 ng/mL. Considering the size of our cohort, a larger study to confirm the value of S-DC3H is needed.
The most accurate timepoints for postoperative intestinal ischaemia detection using PCT levels were postoperative day 3, followed by 24 h after declamping and postoperative day 7. We consider timepoints DC24H and POD3 as the clinically most important. With the AUC higher than 0.9, we conclude that PCT might help in postoperative intestinal ischaemia detection as a supportive test. The issue is the low specificity of this marker. It is questionable to perform a CT scan or colonoscopy based on PCT elevation in the postoperative period. The highest value of this marker is the exclusion of intestinal ischaemia because normal PCT levels below 0.5 ng/mL mean that the diagnosis of intestinal ischaemia is very unlikely. For the proper establishment of ideal cut-off value in clinically most relevant timepoints between POD1 and POD3 large-scale studies are needed.
Our study has of course some limitations. Only 80 patients were enrolled in the study and there were only 6 endpoints. Another limitation is the use of MRI imaging for the diagnosis of intestinal ischaemia and no confirmation by invasive measures like a colonoscopy. The strengths of the study are that this study was prospective with exactly defined timepoints for PCT sampling and only one sample missing (sample S-POD7 of patient no. 35 who died on postoperative day 3). The cohorts of patients were well defined, the procedures were elective and standardly performed, and all the patients except patient no. 35 (who was diagnosed by surgery) underwent medical imaging to detect intestinal ischaemia.
Conclusion
Procalcitonin levels in the postoperative period at proper timepoints might help to detect postoperative intestinal ischaemia. The limitation of this marker is its low specificity for intestinal ischaemia and low positive predictive value. The highest value of this marker is that it can rule out this complication because normal PCT levels mean that intestinal ischaemia is very unlikely.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Ministry of Health of the Czech Republic, grant no. 17-29701A. All rights reserved.