
Abstract
Background
Avoiding operative intervention during the active phase of vasculitis is a central tenant of management of this pathology. For unusual presentations of vascular disease, the early diagnosis of vasculitis is imperative to guide treatment.
Methods
We present the case of a 68-year-old female who presented with a spontaneous brachial artery pseudoaneurysm and was found to have granulomatosis with polyangiitis.
Results and conclusion
The management of arterial complications of vasculitis are particularly difficult in the active phase of disease. Our patient had successful resolution of her pseudoaneurysm with ultrasound compression, avoiding open or endovascular intervention during the active phase of disease.
Introduction
Pseudoaneurysms (PSAs) predominantly arise iatrogenically secondary to vascular access attempts. They are more frequently encountered in the lower extremities, though, upper extremity PSAs can occur. Traumatic and iatrogenic PSAs of the brachial artery have been reported. Spontaneous brachial artery PSA are exceedingly rare. The differential includes numerous vasculitides.
In 2022, the American College of Rheumatology in conjunction with the European Alliance of Associations for Rheumatology published new point-based diagnostic criteria for granulomatosis with polyangiitis (GPA). This uses a combination of clinical criteria as well as imaging findings, lab findings, and histology. The most heavily weighted aspect of this system is a positive cytoplasmic antineutrophil cytoplasmic antibodies (cANCA) or anti-proteinase 3 (anti-PR3) antibodies. 1
Itnitial management of active vasculitis is primarily medical, with steroids followed by immune modulators. In the setting of major vascular involvement, interventions may be necessary to treat symptomatic stenosis or in the setting of rupture of aneurysm or pseudoaneurysms.2,3 Both endovascular and open interventions have historically been preferred only in the quiescent phase. In the active phase of disease, endovascular intervention can serve as a bridge to definitive open reconstruction.
Here, we present the case of a spontaneous brachial artery PSA secondary to granulomatosis with polyangiitis (GPA) presenting during the active phase of disease. In addition to medical management, it was treated with ultrasound-guided compression resulting in resolution. The patient consented to their information and imaging to be used for publication.
Case report
A 68-year-old female with a past medical history of hypertension presented to her outpatient hematologist with night sweats, fevers, weight loss, weakness, hearing loss, and persistent sinusitis that was responsive to steroids. Outpatient computed tomography (CT) demonstrated an anterior mediastinal mass, pericardial effusion, and lymphadenopathy prompting hospitalization. Initial lab work revealed an acute kidney injury, and an Anti-Nuclear Antibody (ANA) titer of 1:320 (normal <1:20). Physical exam revealed a pulsating mass in the proximal right upper arm. Arterial duplex demonstrated a partially thrombosed 2.6 cm PSA of the brachial artery (Figure 1). The PSA neck measured 0.34 cm wide x 0.67 cm long. The favorable length to width ratio, ∼2:1, influenced our decision in attempting compression. Given the favorable neck anatomy, had compression failed, thrombin injection would have been the subsequent step. Partially Thrombosed 2.6 cm PSA of the brachial artery demonstrating yin-yang sign on color duplex.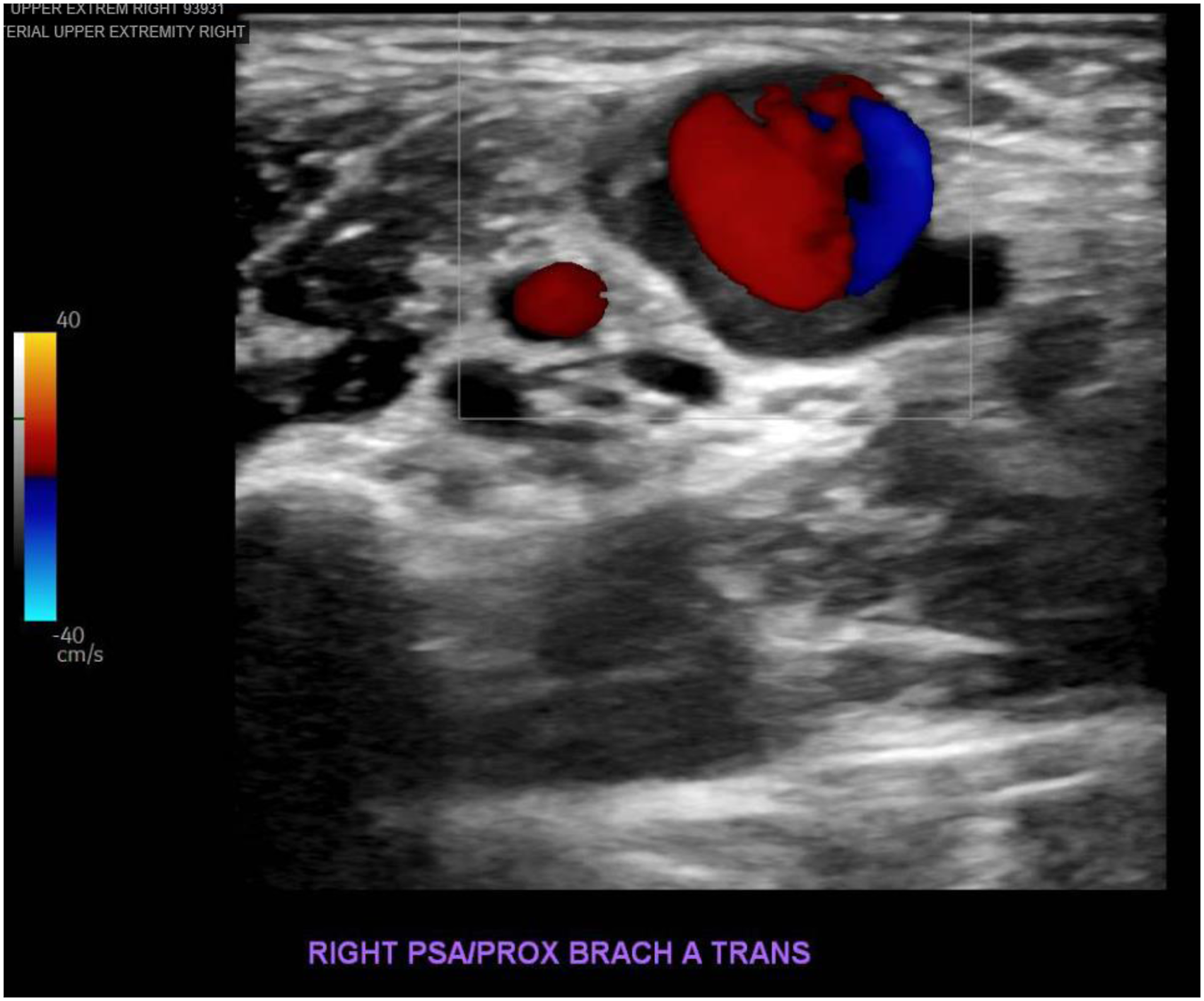
The patient had no ischemic symptoms in the hand, nor the stigmata of a thromboembolic event or median nerve compression. She underwent both renal biopsy and robotic total thymectomy with resection of the mediastinal mass while her rheumatology panel was pending. Her ANCA result was positive with a marked increase in her anti-PR3. Mediastinal mass pathology demonstrated foci of necrotizing granulomatous vasculitis involving small arteries. Renal biopsy demonstrated focal necrotizing and crescentic glomerulonephritis. Both findings were compatible with PR3-ANCA vasculitis, leading to the diagnosis of GPA.
The brachial PSA was treated with ultrasound-guided compression. The arm was positioned for adequate exposure and supported with pillows to minimize strain on the patient. The PSA and its neck were visualized on ultrasound and compressed until there was collapse of the neck and no flow was seen in the PSA. This was held for 30 minutes. The patient tolerated the compression well without significant discomfort. Upon release, there was no demonstrable flow. A formal follow-up ultrasound the following day confirmed thrombosis (Figure 2). She was discharged on high-dose oral steroids with plan to transition to Rituximab. Follow-up Ultrasound after compression demonstrating thrombosed PSA with no flow.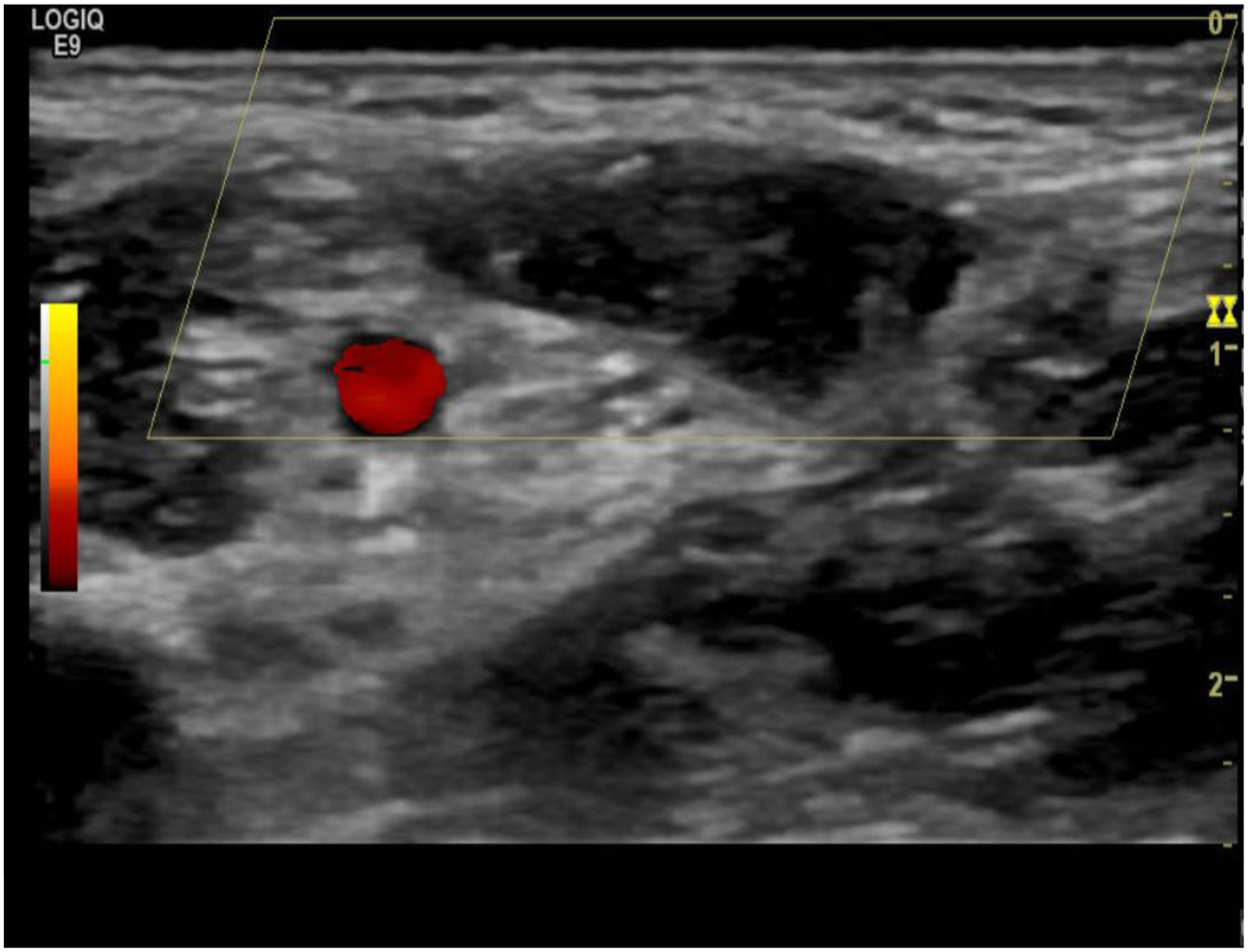
Two months after ultrasound compression of the PSA, repeat arterial duplex demonstrated an obliterated PSA and normal brachial arterial waveforms (Figure 3). Follow-up ultrasound at 2 months demonstrating obliterated PSA with normal brachial arterial waveforms.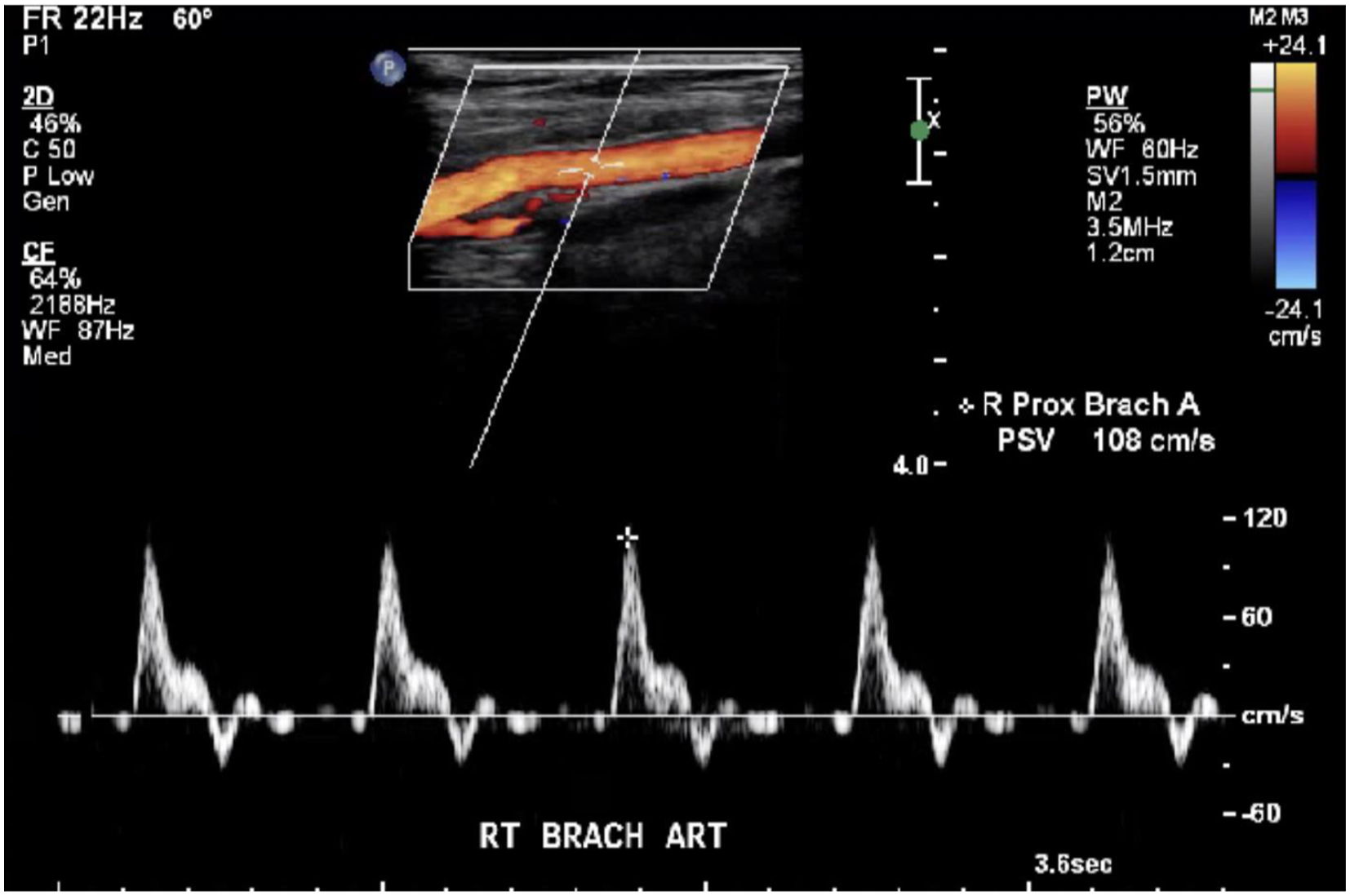
Discussion
GPA, previously Wegener’s granulomatosis, is a rare autoimmune condition of unknown etiology. It can present with a triad of necrotizing granulomas of the respiratory tract, necrotizing or granulomatous vasculitis of small-to-medium vessels, and progressive glomerulonephritis.4–6 This can present with a myriad of nonspecific symptoms such as: fever, cough, arthritis and sinusitis. However, symptoms falling under the more classic triad previously described include: glomerulonephritis, pulmonary infiltrates, and conjunctivitis. 5 PR3-ANCA is positive in 95% of patients with generalized GPA, making it highly specific for diagnosis.4–6 PR3 expression on the surface of neutrophils has been implicated in the pathogenesis of GPA. PR3-ANCA can then bind to this glycoprotein and activate a proinflammatory cascade resulting in endothelial cytotoxicity. 6
This inflammation can result in aneurysmal changes; however, this is a very rare complication of GPA. Commonly affected vessels included those of large and medium sizes, as well as branches of the celiac and renal arteries.5,6 While GPA can affect medium sized vessels, the brachial artery is not well described. As our patient’s PSA was discovered incidentally on physical exam in the setting of thin body habitus, it is unclear if this is due to the artery being unaffected in GPA or if they are asymptomatic and remaining undetected. In contrast to aneurysms, PSAs are not bounded by all three layers of the arterial wall. Instead, PSAs occur when the arterial wall is injured, resulting in either an outpouching of turbulent flow between the tunica media and tunica adventitia or a focal contained rupture in which the surrounding tissues encase the bleeding, preventing external hemorrhage or significant tracking tissue planes. While PSAs may be caused by inflammation and iatrogenic causes, such as post catheterization, most PSAs are due to trauma. They may be clinically silent, present with local signs due to the mass itself, or may present with distal ischemia or embolization. However, the most feared complication is rupture.7,8,9 Those presenting with mass effect require not only intervention but also decompression of the cavity in order to relieve the compression. In our patient, there was no mass effect, allowing for the option of a non-invasive intervention and avoiding surgery in a patient with acute vasculitis.
A spontaneous brachial pseudoaneurysm has been reported previously by Demircioglu et al. In that instance, a 13-year-old girl presented with 3 months of swelling and pain in her right upper arm with nerve deficits. She had facial acneiform lesions, recurrent oral ulcerations and a family history of Behçets disease. Workup revealed a 12.2 × 8.4 cm PSA for which steroids were initiated followed by azathioprine, colchicine, and eventual bypass. 10
Color DUS is the first-line imaging modality used to assess a PSA. It can identify a PSA and assess the size its neck, follow the blood flow associated with it, as well as assess the integrity of nearby vessels and presence of loculations. Color DUS is classically sufficient in diagnosing PSAs, as in our case. However, US is limited by user dependence. In some circumstances, other imaging modalities such as MRA, multidetector CT, and digital subtraction angiography may be more suitable.
Management of any PSA is dependent on size, location, and pathogenesis. Surgical treatments of PSAs have been widely replaced by the minimally invasive techniques. The most widely used methods today are US-guided compression and US-guided percutaneous injection of thrombin into the PSA. Contraindications to US-guided compression are infection, coexisting large hematomas with impending compartment syndrome, limb and skin ischemia, patient discomfort, and unsuitable anatomy. The presence of these factors favors surgical repair of the PSA, which can range from primary repair, patch angioplasty, or in the setting of infection can include: bypass and ligation of the native artery. Complications of this procedure are uncommon with several studies reporting complication rates between 0 and 4.3%. Anticoagulation status is that main factor that can adversely affect this procedure’s success, in which percutaneous thrombin injection is indicated instead. Contraindications to US-guided thrombin injection, outside of the contraindications for US-guided compression, may include allergy to thrombin or similar compound, body habitus or location of the PSA, or unfavorable anatomy that may increase the risk of thromboembolic complications such as: short/wide neck of the PSA, or inability to achieve compression that occludes the neck and halts PSA flow while permitting injection.11,12 Complication rates for thrombin injection have been reported to be around 1.3% with embolic events occurring at a rate of 0.5%.13 Successful PSA thrombosis has been reported as high as 92–100% for ultrasound guided thrombin injection compared to 50–98% with ultrasound-guided compression.11,13 The favorable anatomy of our patient’s PSA and intact overlying skin integrity allowed for ultrasound compression to be used and forego an initial open surgical repair. The longer narrow PSA neck also facilitated easier compression without causing significant patient discomfort.
Conclusion
The management of arterial complications of vasculitis are particularly difficult in the active phase of disease. Our patient had successful resolution of her pseudoaneurysm with ultrasound compression, avoiding open or endovascular intervention during the active phase of disease.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.