
Abstract
Objective
To determine the association between the tortuosity of the internal carotid artery and vertebral artery and the occurrence of acute ischemic stroke based on a new quantitative method.
Methods
This retrospective case-control study was conducted on 63 patients diagnosed with acute ischemic stroke in the case group and 52 patients in the control group. All the participants underwent neck Computed Tomography Angiography. The images were retrospectively reviewed and the tortuosity index was measured for internal carotid and vertebral artery. Then, a multivariable binary logistic regression model adjusted for the potential confounders was performed to assess the independent effect of internal carotid/vertebral artery tortuosity on acute ischemic stroke.
Results
Analysis of the logistic regression model revealed a significant effect of the internal carotid artery tortuosity index on anterior territory infarction (odds ratio = 1.04, p = 0.01) as well as a significant effect of the vertebral artery tortuosity index on posterior territory infarction (odds ratio = 1.14, p < 0.001). The optimal cut-off points for the internal carotid and vertebral artery tortuosity were 16.91 and 22.96, respectively.
Conclusions
This study showed that tortuosity of extracranial portions of the internal carotid and vertebral artery could be an independent imaging predictor of acute ischemic stroke in anterior and posterior circulation territories, respectively.
Keywords
Introduction
Carotid abnormalities have been a well-known phenomenon since the beginning of the century. A number of etiologies have been reported such as age, gender, and congenital factors, but controversy persists regarding the etiology and clinical significance of carotid abnormalities. Stroke is the third leading cause of death in the United States, causing approximately 700,000 deaths each year. Ischemic stroke accounts for the majority of all strokes (88%). Although carotid stenosis of different degrees plays a critical role in developing major strokes, other risk factors than stenosis have been suggested in recent investigations. 1
The relationship between carotid tortuosity and ischemic stroke was first proposed in 1951, 2 but this association has been extensively debated. Despite the suggestion for the possible association between carotid artery tortuosity and atherosclerotic plaques, determining the role of carotid abnormalities in inducing ischemic stroke is yet a matter of controversy. 3 Few studies have demonstrated a possible relationship between Internal Carotid Artery (ICA) tortuosity and acute ischemic stroke, while this has not been the case in some other investigations.4,5,6
The etiology of the tortuous variants of ICA has been classified into acquired and congenital categories. The acquired type is much more common and its most important causes are atheroma, aging, and hypertension. Aging, together with atherosclerotic plaques, weakens the vessel walls, thereby making them more susceptible to hemodynamic stress.7,8 The congenital etiology, on the other hand, is more frequent in young adults and children. Additionally, hormonal factors may contribute to the marked predominance of tortuosity among female patients. 9
For decades, the evaluation of carotid tortuosity was based on qualitative methods such as geometrical model simulation 10 by expert radiologists to assess carotid morphology, which was limited by inter-observational and intra-observational variability. 11 Color duplex sonography measurements were also used, which were accompanied by similar limitations. 5 However, few recent studies, most of which were conducted in China, introduced a new quantitative method that involved the use of the Tortuosity Index (TI) based on carotid Computed Tomography Angiography (CTA) to assess carotid tortuosity. This new method seems to be replacing the old ones by providing more accurate and reliable results and being accompanied by fewer limitations.6,9,12
Considering what was mentioned above, it is of clinical importance to determine the association between the tortuosity of ICA and Vertebral Artery (VA) and the occurrence of acute ischemic stroke based on new quantitative methods. Therefore, the present study aims to assess the above-mentioned relationship so as to help in better patient risk assessment. To the best of our knowledge, this is the first study evaluating this association in an Iranian population using novel quantitative methods.
Materials and methods
This retrospective, case-control study was conducted on 115 patients; 63 patients diagnosed with acute ischemic stroke proven by Diffusion-Weighted Imaging (DWI) MRI in the case group and 52 patients with other neurological symptoms than acute ischemic stroke (mainly headache and dizziness) in the control group. All the case group patients met the inclusion and exclusion criteria. The inclusion criteria were the diagnosis of acute ischemic stroke confirmed by DWI sequence MRI among patients in their first episode of acute ischemic strokes, passage of at most seven days from onset to admission, and presence of clear neurological signs of acute ischemia at the time of admission. The exclusion criteria were suffering from strokes caused by cardiogenic embolism and emboli originating from the heart and aorta such as atrial fibrillation, cardiomyopathy, and valvular heart disease, presence of any special abnormalities in blood vessel morphology such as cerebrovascular malformations, intracranial aneurysm, and Moya Moya Disease (MMD), presence of vascular diseases with the etiology of connective tissue disorders such as Loeys–Dietz syndrome and Marfan syndrome, and special infections causing vascular disease such as syphilis. In the control group, the participants did not have any signs and symptoms of acute ischemic stroke either prior to or at the time of admission. There was also no evidence of acute ischemia on DWI sequence brain MRI. In addition, they had no underlying vascular diseases with the etiology of connective tissue disorders such as Loeys–Dietz syndrome and Marfan syndrome, no history of special infections causing vascular diseases such as syphilis, no underlying heart diseases causing distant embolism such as atrial fibrillation, cardiomyopathy, and valvular heart disease, and no special abnormality in blood vessels morphology such as cerebrovascular malformations, intracranial aneurysm, and MMD.
The collected clinical data includes age, gender, and presence of some important vascular risk factors such as hypertension (defined by systolic/diastolic blood pressure >140/90 mmHg or being on antihypertensive treatment), diabetes mellitus (defined by fasting blood glucose >110 mg/dl or being on antidiabetic treatment), and cigarette smoking. The presence of other atherosclerotic diseases and peripheral vascular diseases was assessed, as well.
All the participants underwent neck CTA at Namazi Hospital, Shiraz, Iran from September 2019 to September 2021 and the images were retrospectively reviewed. CTA examination of the neck included the bifurcation of the common carotid artery and origins of VAs and extracranial portions of both ICAs and VAs. The extracranial portion of ICA was measured from its origin from carotid bifurcation until the beginning of the petrous segment (C1 segment). The extracranial portion of VA was also measured from its origins until the level of C1-2 where the artery pierces the dura to form the intracranial portion (V3 segment).
All the patients were scanned using 16-slice General Electric light speed scan machine (GE Medical Systems, Milwaukee, WI, USA) and three-dimensional volume rendering reconstructions of blood vessels were provided. Using Maximum Intensity Projection (MIP) and curved multi-planar reconstruction (MPR) methods and surface-shaded display technique, an experienced board-certificated radiologist and a radiology resident used the blind method to measure the vascular tortuosity index (TI) separately, and a consensus was achieved. As shown in Figure 1, a line was drawn in the center of the vessel, which represented the “actual distance” between the two ends of the vessel. A vertical line was also drawn, which connected the two ends of the vessel and represented the “straight line distance.” Then, the vascular TI was calculated using the following formula: TI = the actual distance/straight line distance−1) × 100%. These measurements were done for extracranial portions of ICA and VA on both sides. Measurement of the tortuosity index. (a) A surface-shaded display image showing tortuosity of the internal carotid artery. Straight and actual line distances are drawn to calculate the tortuosity index. (b) Curved multi-planar reconstruction (MPR) and (c) straightened curved MPR methods are useful tools for the measurement of straight and actual distances between the two ends of the vessel.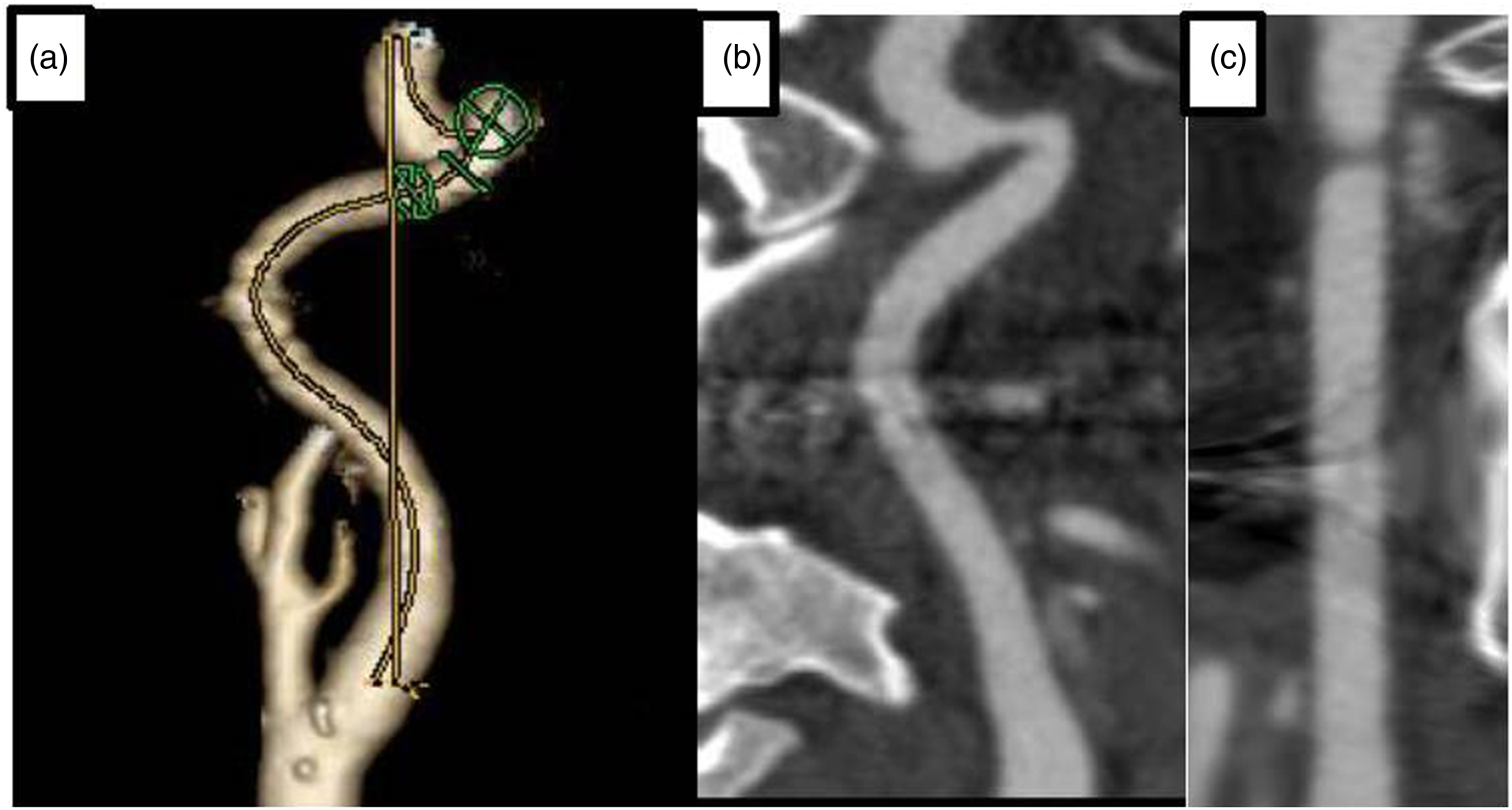
Statistical analyses were done using the SPSS 26.0 software (IBM Corporation, Armonk, NY, USA). The average TI of ICA was calculated by adding up the TIs of the right and left ICAs divided by two (TI_ICA). The average TI of the vertebral arteries was also calculated by the same method (TI_VA). The average TI of ICA and VA was computed, as well (TI_mean). To compare the study groups in terms of TI_VA, TI_ICA, and TI_mean, an independent sample t-test was used. Moreover, a binary logistic regression model adjusted for the potential confounders (age, sex, hypertension, smoking, and diabetes mellitus) was applied to determine the effect of TI_mean on the outcome. The variables with p < 0.2 in the binary logistic regression analysis were selected. Receiver Operating Characteristic (ROC) curve analysis was used for generating an optimal cut-off point to allocate the participants to the study groups. p < 0.05 was considered statistically significant.
It must be noted that this study was approved by the Ethics Committee of Shiraz University of Medical Sciences. Written informed consent for patient information and images to be published was provided by the patients or a legally authorized representative.
Results
The participants’ characteristics based on the study groups.
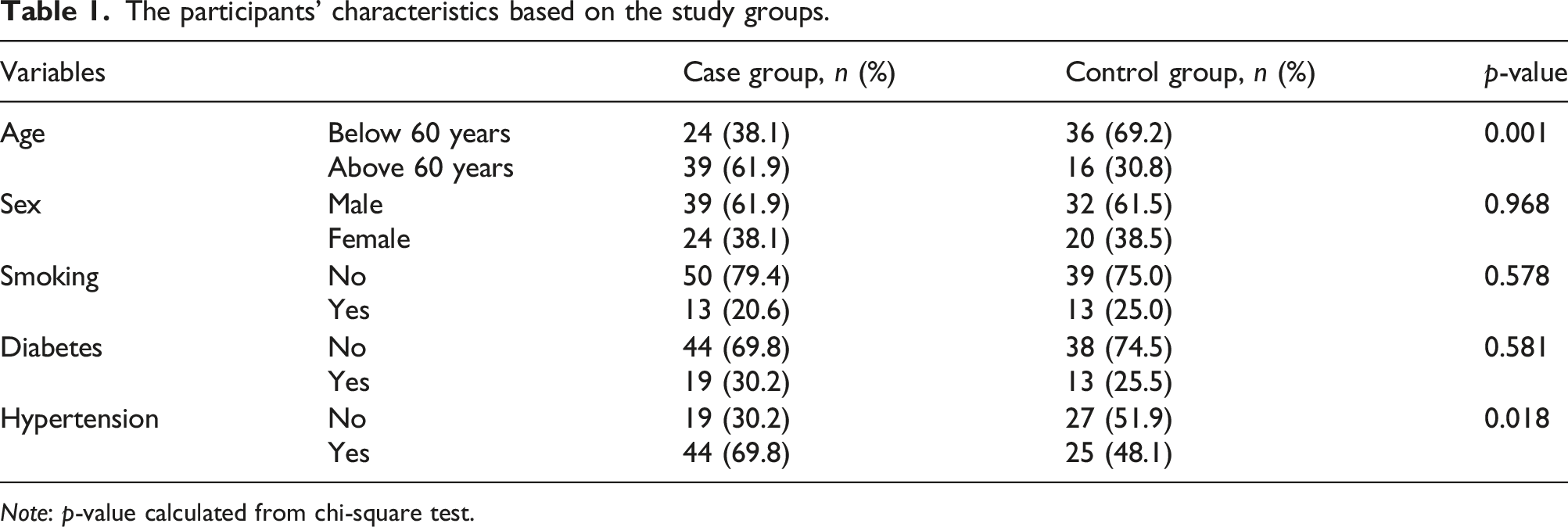
Note: p-value calculated from chi-square test.
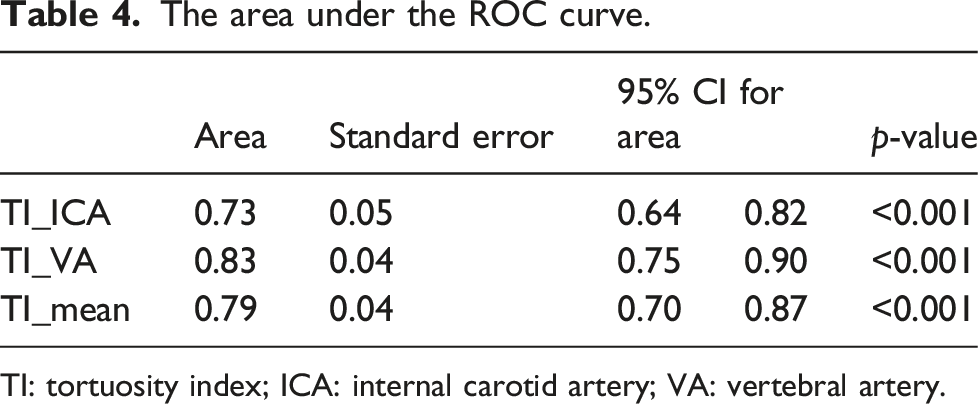
The average tortuosity index of ICA and VA based on the study groups.
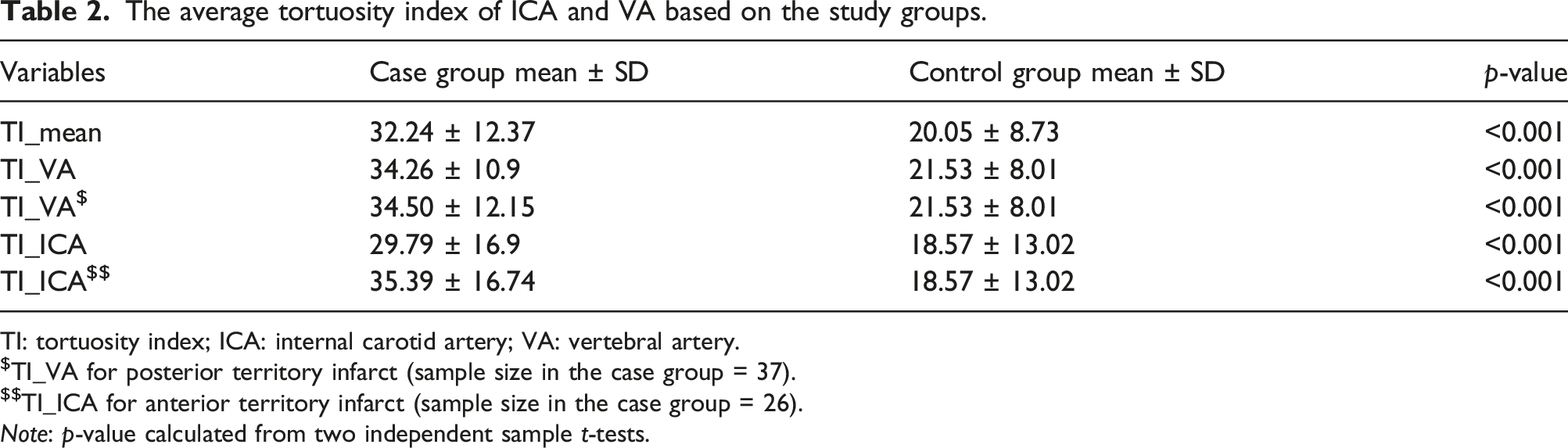
TI: tortuosity index; ICA: internal carotid artery; VA: vertebral artery.
$TI_VA for posterior territory infarct (sample size in the case group = 37).
$$TI_ICA for anterior territory infarct (sample size in the case group = 26).
Note: p-value calculated from two independent sample t-tests.
Modeling of the outcome (patient and control groups) based on tortuosity index adjusted for age and hypertension.
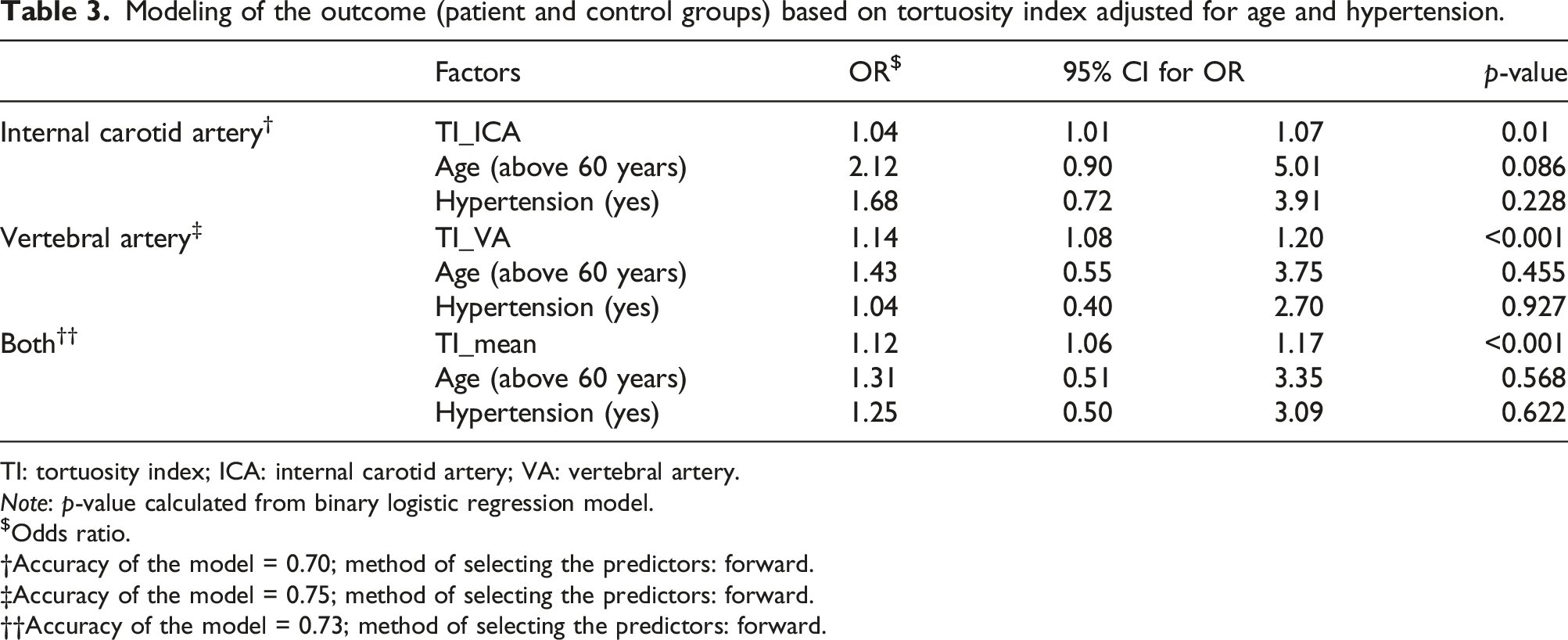
TI: tortuosity index; ICA: internal carotid artery; VA: vertebral artery.
Note: p-value calculated from binary logistic regression model.
$Odds ratio.
Accuracy of the model = 0.70; method of selecting the predictors: forward.
Accuracy of the model = 0.75; method of selecting the predictors: forward.
††Accuracy of the model = 0.73; method of selecting the predictors: forward.
The results of the logistic regression model revealed the significant effect of TI_ICA (ORadj = 1.04, p = 0.01), TI_VA (ORadj = 1.14, p < 0.001) and TI_mean (ORadj = 1.12, p < 0.001) on ischemic stroke. Therefore, TI_ICA, TI_VA and TI_mean could be considered significant predictors of the outcome.
To find an optimal cut-off point to allocate the participants to the case and control groups, ROC curve analysis was applied (Figure 2 and Table 4). The Area Under the Curve (AUC) of ROC was 0.73 for TI_ICA, which indicated the significant accuracy of TI_ICA for assigning the participants to the two study groups (p < 0.001; Table 4). In the same way, AUC was 0.83 for TI_VA and 0.79 for TI_mean that indicated the significant accuracy of TI_VA and TI_mean to allocate the participants into the two study groups (p < 0.001; Figures 3 and 4 and Table 4). Receiver operating characteristics curve to illustrate the diagnostic ability of the logistic regression model based on TI_ICA, as a strong predictor (TI, tortuosity index; ICA, internal carotid artery). The area under the ROC curve. TI: tortuosity index; ICA: internal carotid artery; VA: vertebral artery. Receiver operating characteristics curve to illustrate the diagnostic ability of the logistic regression model based on TI_VA, as a strong predictor (TI, tortuosity index; VA, vertebral artery). Receiver operating characteristics curve to illustrate the diagnostic ability of the logistic regression model based on TI_mean, as a strong predictor (TI, tortuosity index).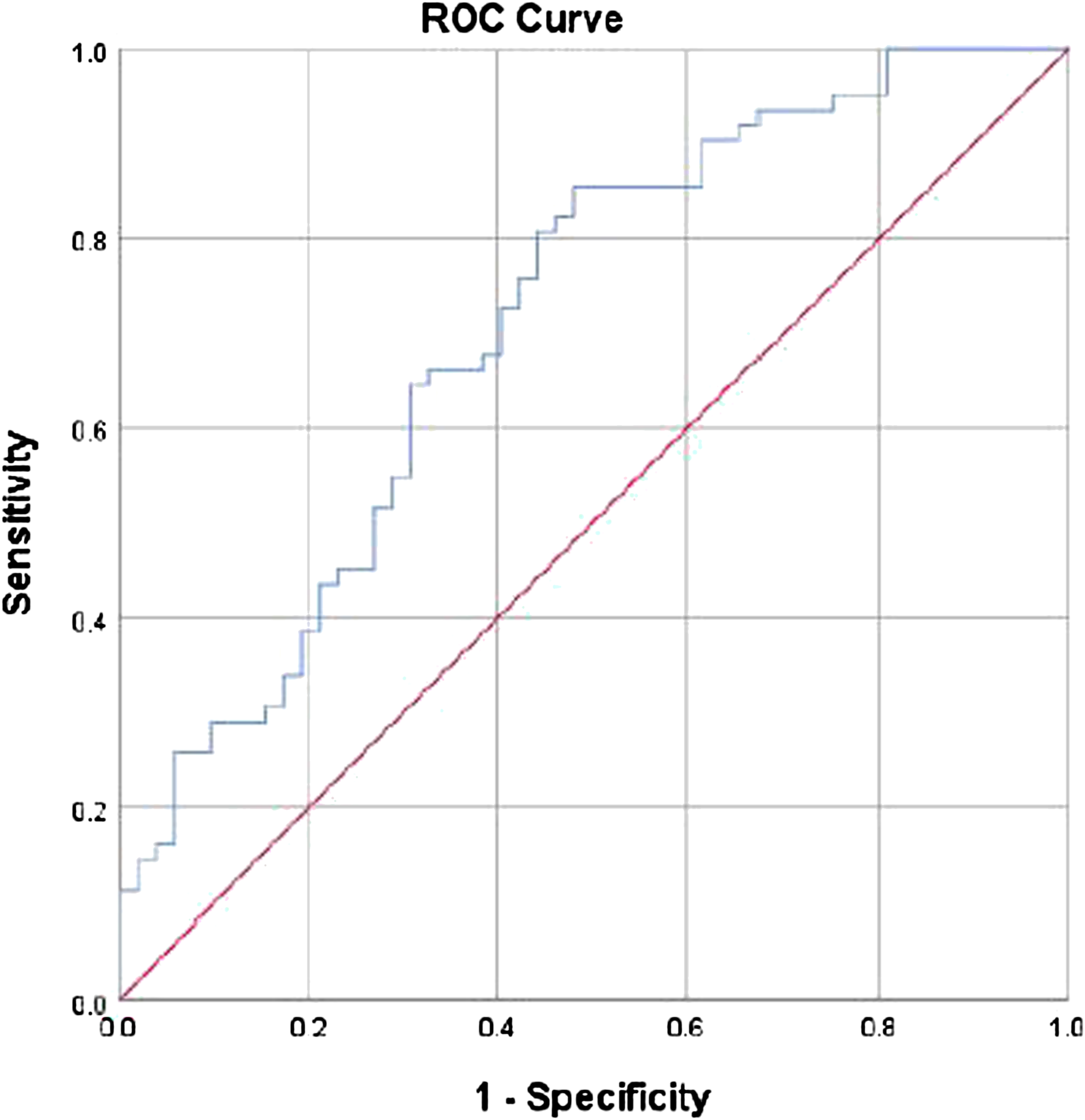
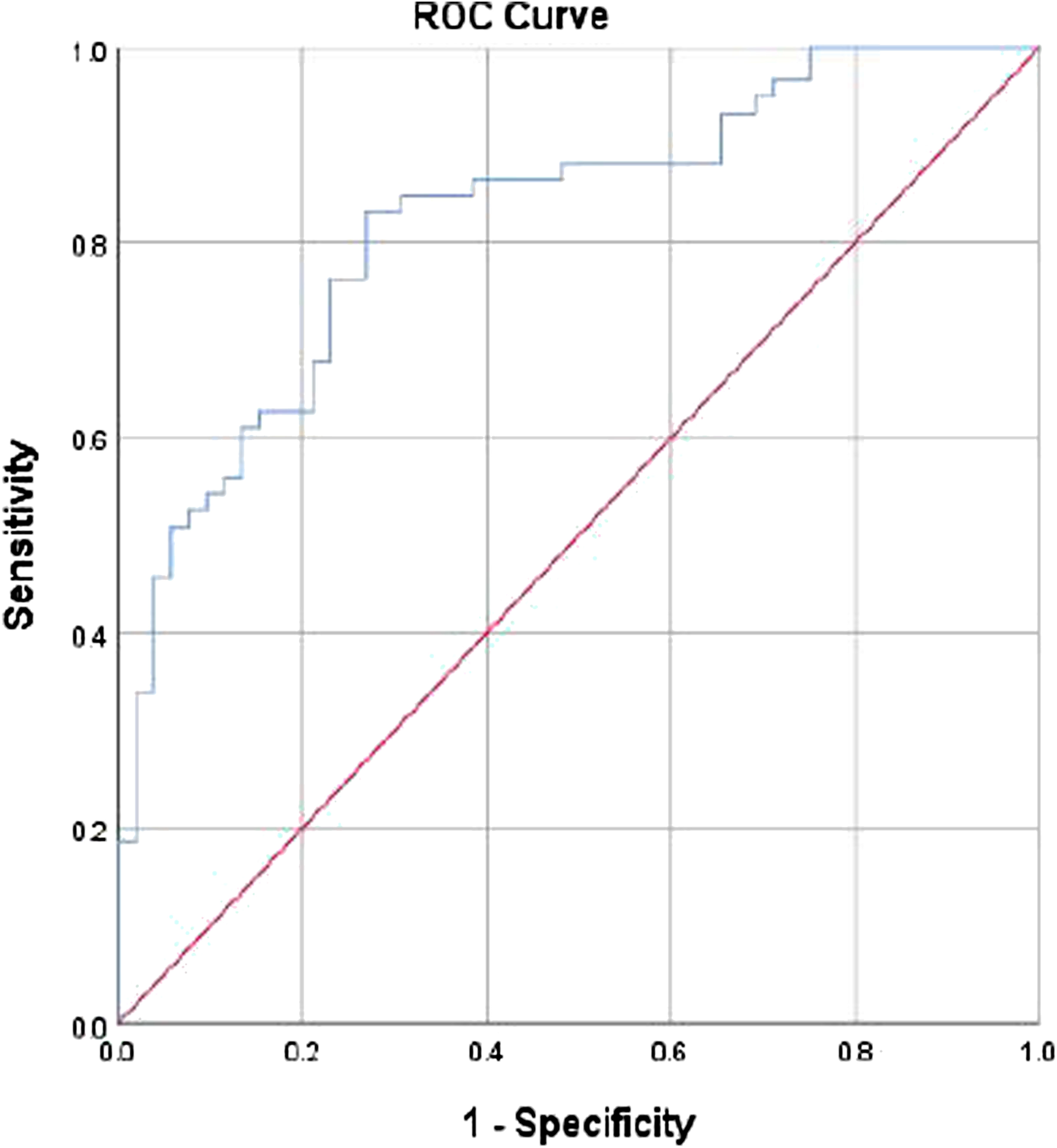
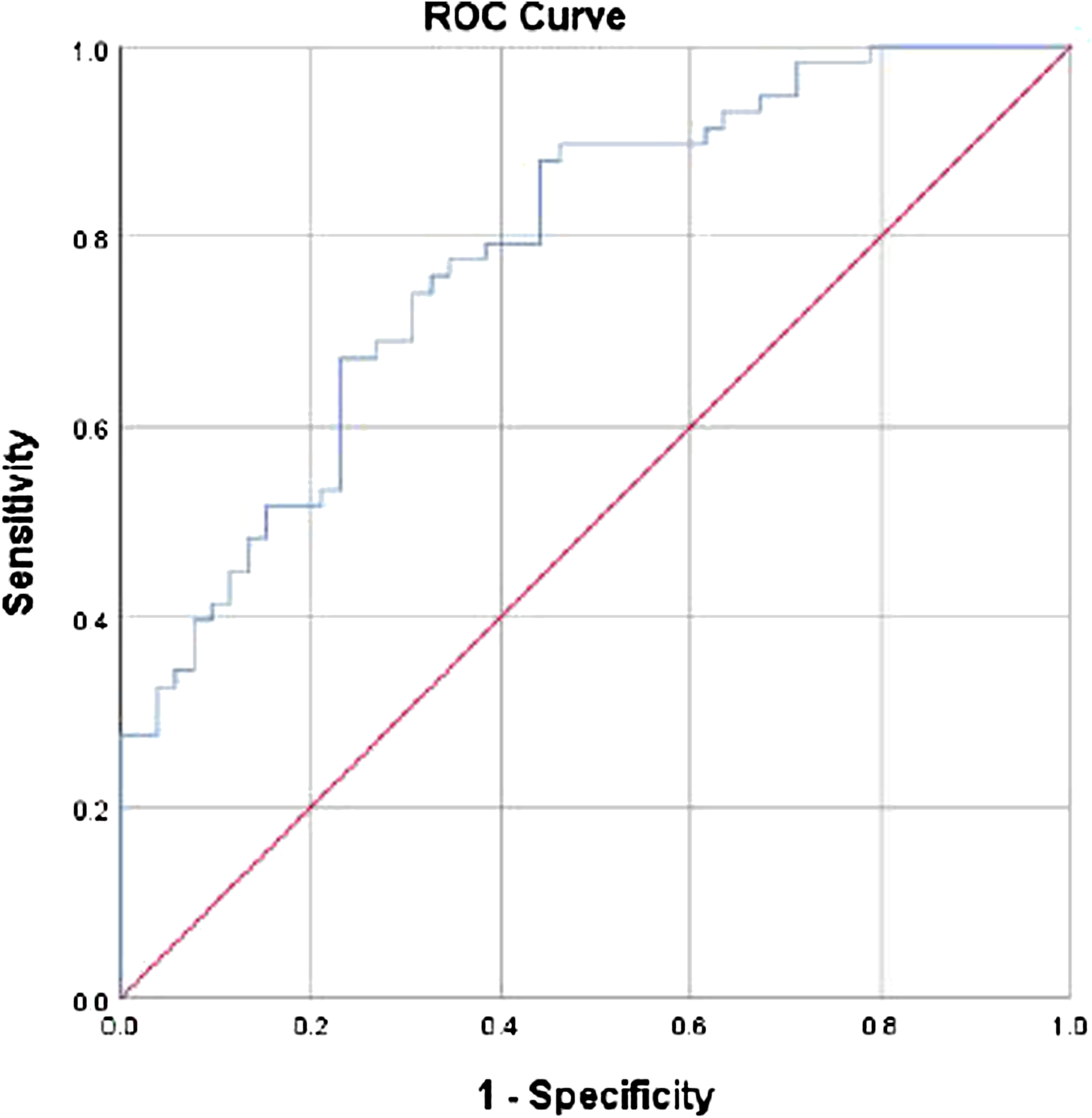
The ROC curve analysis generated an optimal TI_ICA value of 16.91. Thus, the TI_ICA values equal to and greater than 16.91 indicated patient groups with a sensitivity of 0.71 and specificity of 0.60. Besides, the ROC curve analysis generated an optimal TI_VA value of 22.96. So, TI_VA values equal to and greater than 22.96 indicated patient groups with a sensitivity of 0.85 and specificity of 0.70. In addition, the ROC curve analysis generated an optimal TI_mean value of 23.53. Hence, TI_mean values equal to and greater than 23.53 indicated patient groups with a sensitivity of 0.74 and specificity of 0.70.
Modeling of the outcome (anterior/posterior territory infarct-control groups) based on TI_ICA and TI_VA adjusted for age and hypertension.
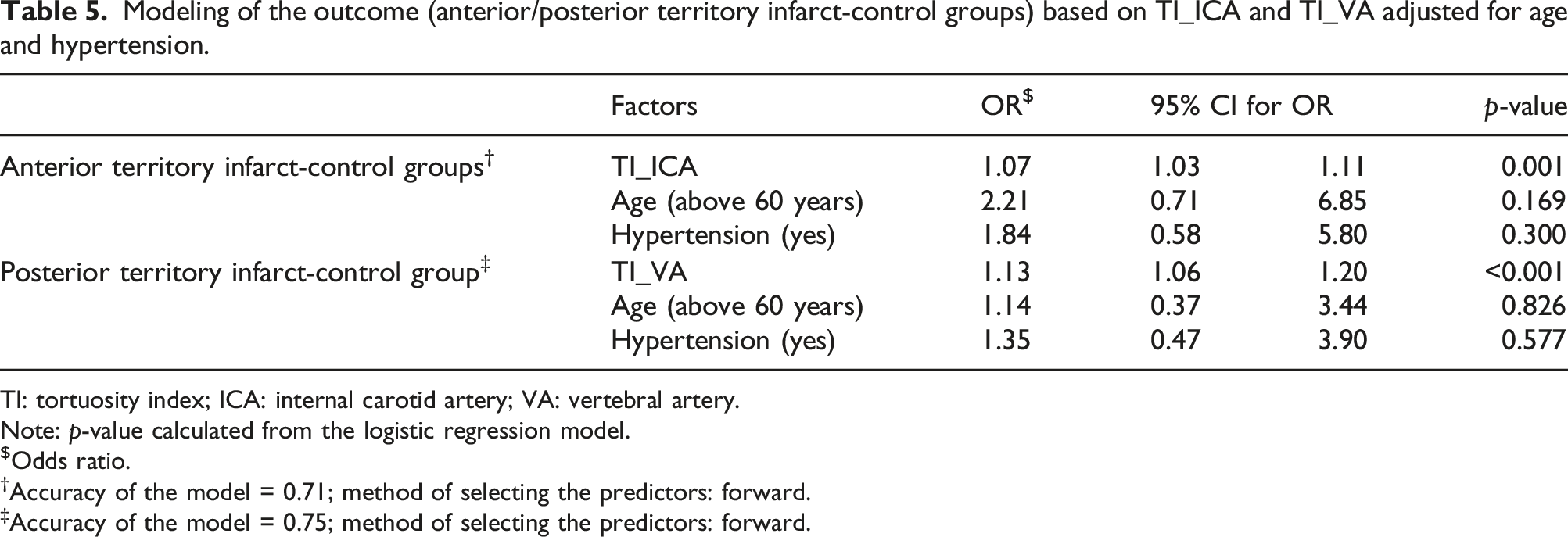
TI: tortuosity index; ICA: internal carotid artery; VA: vertebral artery.
Note: p-value calculated from the logistic regression model.
$Odds ratio.
†Accuracy of the model = 0.71; method of selecting the predictors: forward.
‡Accuracy of the model = 0.75; method of selecting the predictors: forward.
Discussion
The study findings demonstrated that the tortuosity of the extracranial portions of ICA and VA could be considered an independent imaging predictor of acute ischemic stroke in anterior and posterior circulation territories, respectively. The optimal cut-off point of the ICA tortuosity was 16.91 (values greater than 16.91 might indicate an increased chance of anterior territory infarction with a sensitivity of 0.71 and specificity of 0.60) and the optimal cut-off point of the VA tortuosity was 22.96 (values greater than 22.96 might indicate an increased chance of posterior territory infarction with the sensitivity of 0.85 and specificity of 0.70).
Tortuosity of blood vessels, as a common angiographic finding, was correlated to vascular pathologies and might be a sign of systemic diseases such as hypertension and diabetes mellitus.13,14,15 A primary failure of elastin rather than collagen in vessel walls has been mentioned as the main cause of developing tortuosity. 16 Tortuosity is generally found in a large number of blood vessels and has been investigated in retinal and coronary arteries. Tortuosity in brain vessels was associated with atherosclerosis and MMD.17,18 Moreover, ICA anomalies might be a risk factor for massive bleeding and dissection. 11
Kliś et al. 17 reported in their study that TI of ICA was significantly higher in patients with aneurysms than in the control group. These associations could be secondary to metaplasia of tunica media, leading to the substitution of muscular and elastic tissues for loose connective tissues. 19
In several previous studies, the female gender was found to be an independent risk factor for vessel tortuosity.6,9 Tortuosity can also increase with age. Although the effect of age on tortuosity is still controversial, several studies have shown the possibility of an association between the two variables.7,8,13,20 For instance, the prevalence of carotid artery kinking was three times higher among the aged population and four times higher in the aged hypertensive population. Tortuosity in other vessels such as the thoracic and abdominal aorta and even extremity vessels was also shown to be significantly related to age.7,8 Several clinical studies have demonstrated hypertension as a risk factor for arterial tortuosity.21,22 Moreover, tortuous carotid arteries have been often reported in hypertensive patients.4,7 Thus, hypertension can be simultaneously the cause and the effect of this situation. Considering the possible correlations between vessel tortuosity and some other variables such as age, sex, diabetes mellitus, hypertension, and smoking (based on the previous studies), these factors were regarded as confounding variables in the assessment of the possible association between ICA/VA tortuosity and acute ischemic stroke in the present research. In this study, a binary logistic regression model adjusted for the potential confounders was performed to determine the independent effect of ICA/VA tortuosity on acute ischemic stroke. Additionally, instead of other qualitative descriptive methods, TI as a more accurate method was used to evaluate the severity of ICA tortuosity. According to the results, TI of ICA was significantly higher in the case group with acute anterior territory ischemic stroke compared to the control group. The same results were obtained in the comparison of the case group with posterior territory ischemic stroke to the control group regarding the TI of VA. These results were compatible with those of another study conducted in China. In 2017, Cao et al. 6 explored the correlation between the tortuosity of extracranial ICA and VA and acute ischemic stroke. CTA was used to measure multiple vascular morphological indices. The results revealed higher indices in the stroke group in comparison with the control group.
The pathophysiology of cerebral ischemia secondary to ICA/VA tortuosity is not clear yet, but there are some possible explanations for this association. First of all, the resistance of blood vessels is directly related to the length of the vessels. On the other hand, blood flow is inversely associated with the resistance of blood vessels. Thus, an increase in the ICA/VA length (which shows an increase in the TI of ICA/VA) can reduce cerebral perfusion and may lead to cerebral ischemia. For example, reduction of blood pressure during sleep can decrease cerebral blood flow and may lead to transient ischemic attacks or minor ischemic strokes. Elongated and tortuous cervical vessels are also prone to transient occlusion after the sudden rotation of the head and neck. ICA/VA tortuosity can change the normal laminar flow to turbulent flow within the lumen of vessels. A reduction in blood flow can also be observed at the site of ICA/VA kinking. These hemodynamic changes may lead to blood stasis in tortuous vessels, which increases the chance of thrombosis and may also be a source of emboli to the brain.23,24
One of the study limitations was the existence of some missing clinical data. Another study limitation was the poor performance of the auto measurement techniques for drawing the central vessel line (for the actual distance), which was caused by the poor quality of the images and low contrast density in some parts of the vessels that were mostly caused by the patients’ bad conditions. Attempts were made to minimize this limitation by using the most accurate manual method to draw the central line. Another study limitation was its small sample size and the fact that the control group consisted of participants with other neurological symptoms than cerebral ischemia (mainly headache and dizziness). Hence, future studies with larger sample sizes are required to compare the results of several centers.
Conclusion
The study results demonstrated that there is a statistically significant difference between the Tortuosity index of the extracranial portions of the carotid and vertebral arteries in the patients with acute ischemic stroke comparing to control group. So, tortuosity of extracranial portions of the internal carotid and vertebral artery could be an independent imaging predictor of acute ischemic stroke in anterior and posterior circulation territories, respectively. Considering the clinical importance of the situation, further studies are recommended to investigate this association for better risk assessment.
Footnotes
Acknowledgments
The authors would like to thank M. Hadipour M.D. at the Healthy Policy Research Center of Shiraz University of Medical Sciences for helping with data analysis and Ms A. Keivanshekouh at the Research Consultation Center (RCC) of Shiraz University of Medical Sciences for improving the use of English in the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The Authors declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.